Spontaneous Neonatal Gastric Perforation: About Two Cases Treated with Success in Cotonou
Neonatal gastric perforation is rare with a serious prognosis. Over a period of 10 years we had two cases successfully treated in our departments. Cases: It was a girl and a boy, vaginely delivered in the same year. The pregnancy was well followed in the first case and badly in the second. APGAR score at birth, at 2700 g girl was 10-10-10, and at 2900 g boy at 7-7-8 after resuscitation. On admission, newborns were cyanotic, tachycardic and tachypnotic; there was abdominal distension with diffuse abdominal tympanism, occurring on the second day, and scrotal swelling in addition for the boy. The abdominal X-rays objectified a massive pneumoperitoneum in the shape of a saddle horse. Laparotomy found gastric perforation in the area of parietal hypoplasia in both cases. An excision suture had been performed. The postoperative course was simple. Conclusion: Spontaneous neonatal gastric perforation is rare. Early diagnosis and management had resulted in a favourable outcome of the cases.
Introduction
Neonatal gastric perforation is rare, with still serious prognosis [1, 2]. Several etiological hypotheses have been advanced, including gastric hypoplasia and perinatal distress [2, 3]. The authors report two (02) cases treated in the two (02) paediatric surgery departments in Cotonou.
Case I
The female newborn weighing 2700g was vaginally born. The pregnancy of 38 weeks was well monitored. There was no neonatal resuscitation (APGAR score 10-07-08). The meconium had been released and she was fed. On the second day of life, the sudden appearance of abdominal distension followed by dyspnoea and fever prompted a consultation in the paediatric surgery. The entrance examination found a newborn in poor general condition, cyanotic, tachycardic (150 beat/min) and polypneic (60 cycles/min). The abdomen was distended (Figure 1a) with diffuse tympany. The abdominal X-rays revealed a massive pneumoperitoneum in the shape of a “saddle horse” (Figure 1b). The diagnosis of peritonitis by perforation of a hollow organ was suggested, hence the indication for surgery. After preoperative resuscitation the laparotomy found a gastric perforation of 2 cm large, leaving saliva as whitish viscous foam (Figure 1c). The perforation was in an area of parietal hypoplasia measuring about 6 cm long axis, on the anterior face close to the large gastric curvature. Excision of hypoplasic tissue was performed and
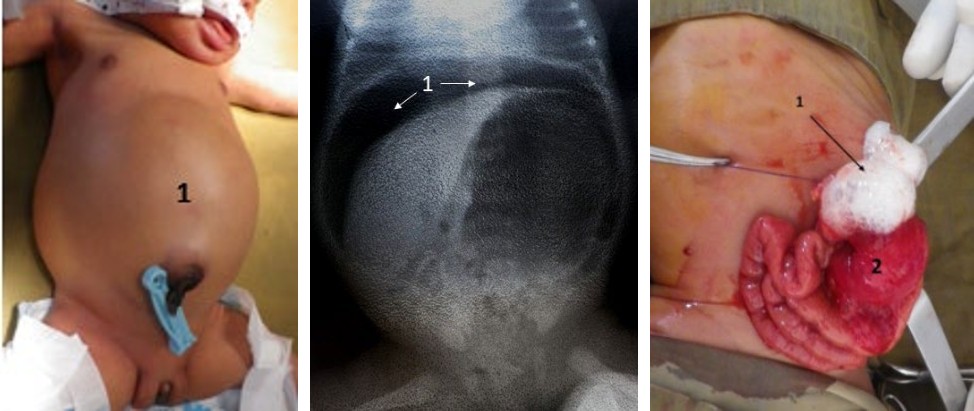
(a) (b) (c) Figure 1a: Abdominal distension (1) in case 1. Figure 1b: abdominal X-ray without preparation in case I revealing a voluminous pneumoperitoneum shaped saddlehorse (1). Figure 1c: Intraoperative image in case I showing a protrusion of saliva (1) through a perforation in a hypoplasic area of the gastric wall (2).
Case II
The male newborn baby with two days of life weighing 2900g was vaginally born. The pregnancy of 37 weeks was poorly monitored. He was resuscitated for five minutes at birth without material device and naso-oral tube. The APGAR score was 7-7-8. Meconium had been normally released. By the second day of life, there was progressive distension of the abdomen associated with right scrotal swelling (Figure 2a). The entrance examination found a newborn in poor general condition, cyanotic, tachycardic (140 beat/min) and (a) (b) (c) Figure 2a: Abdominal distension (1) and scrotal pneumatocele (2) in case II. Figure 2b: Abdominal X-ray without preparation for case II showing a large pneumoperitoneum (1), subcutaneous emphysema (2) and scrotal pneumatocele (3). Figure 2c: Peroperative image of case II showing a perforation of the anterior surface of the antrum close to the small curvature (1).
the stomach was sutured. The postoperative follow-up was simple. After a thirty-month delay, there was good stature- weight growth.
polypneic (55 cycles/min). The abdomen was distended with a perception of collateral venous circulation. There was a snowy crackling of the right anterolateral wall of the abdomen and a diffuse tympanism. Abdominal X-rays revealed a massive pneumoperitoneum in the shape of a “saddlehorse”, with mass effect on the abdominal organs, and right scrotal infiltration (Figure 2b). The diagnosis of peritonitis by hollow organ perforation was established. After preoperative resuscitation, the laparotomy found an antral perforation about 4 cm long, close to the small arch, on a hypoplasic gastric wall (Figure 2c).
An excision of the edges, gastric suture and omentoplasty were carried out with cavity drainage. The parietal hypoplasia was confirmed on an anatomopathological analysis of the surgical specimen. The postoperative follow-up was simple with twenty-seven months of follow-up, the staturo-weight growth was good.
Discussion
The first report of gastric perforation was made by Siebold in 1825. Since then, more than 300 cases have been reported in the literature [4, 5]. The term “spontaneous” or “idiopathic” is used to define a specific entity and excludes gastric perforations associated with distal obstruction [2, 6]. This is applied to the present reported cases as well. Although spontaneous, idiopathic or primitive neonatal gastric perforation accounts for 10 to 16% of neonatal gastrointestinal perforations [1]. The publications on this pathology in West Africa are rare; Mihlouedo-Agbolan KA, et al. [7] reported 03 cases in 12 years that is concordant with our results. Lacusso, et al. [6] reported 02 cases in 09 years in Italy and Yong Hoon Cho, et al. [8] in Korea, 11 cases in 10 years.
The age of occurrence is variable and ranges from two to seven days of life with a peak on the third day [9]. This corroborates with the two days of age in our cases, first days for Naji A, et al. [1], three days for Kayanda, et al. [10] and a mean age of 5.33 days for Mihlouedo-Agbolan KA, et al. [6]. While male predominance was noted in the literature [3, 4, 10], our two cases were of different sexes.
Fetal distress could be the cause of anoxic-ischaemic disorders which could explain the perforation of an already hypoplastic gastric wall [2]. For the second newborn, fetal distress could be an additional risk factor. Other associated risk factors are with the condition, prematurity, low birth weight, amniotic infection or caesarean section [9, 11]. None of these had been found in our newborns.
The most common clinical pathognomonic signs found in the literature are abdominal distension, acute respiratory distress, and subcutaneous emphysema, scrotal pneumatocele in boys or labia majora infiltration in girls [7, 12, 13]. That was the case in ours newborns. This pneumatocele as “a silent sign” of gastric perforation can be misdiagnosis as a vaginal hydrocele [10, 13]. The timely release of meconium, and normally feeding, eliminated neonatal gastric perforations secondary, to obstructive intestinal occlusions [3, 11, 12]. Others modes of revelation of gastric perforation would be a massive digestive haemorrhage, and peritonitis [7, 14, 15]. Massive pneumoperitoneum, as a constant radiological sign of gastric perforation, [1, 2, 7, 12] was also a finding in both of our reports.
The type of peroperative lesions differ according to aetiologies. The punctiform perforations of the anterior or posterior gastric wall, point to ischaemic, mechanical, medicinal or functional causes, whereas the lesions with a linear tear at the level of the large curvature, result from agenesis of the gastric musculature [11, 12, 13]. This was typically the result in the first reported case. In the second, the hypoplasia found during surgery, was confirmed by anatomopathological analysis.
The perforation suturing after debridement of the hypoplasic or necrotic edges [1, 2, 3] was generally performed, as in our cases. Some recommendations are purse-suturing [10], partial or total gastrectomy in cases too large necrosis [15]. The abdominal cavity drainage performed for the second newborn is controversial [1, 8, 10].
Poor prognostic factors such as prematurity, low birth weight and sepsis [9, 15, 16] were not identify in both cases. The evolution has been satisfactory, although in the literature, gastric perforations are still dominated by a high mortality rate of 45 to 58% [15, 17].
Conclusion
Spontaneous neonatal gastric perforation is a rare surgical emergency. In the perinatal period, the occurrence of progressive abdominal distension, subcutaneous emphysema, and massive pneumoperitoneum should suggest it. Early recourse to laparotomy, with removal of the dysplasic area and suture, improves the prognosis.
Conflicts of Interest
The authors do not declare any conflict of interest.
Authors’ Contribution
All the authors contributed to this work. All of them have read and approved the manuscript.
References
-
Naji A, Elkarout Y, Benjiba N (2015) Neonatal spontaneous gastric perforation: about a case. Pan Afr Med J 21: 61.
-
Dupont P, Trentesaux A, Guillemin M, Petit T, Jeanne- Pasquier C, et al. (2003) Idiopathic gastric perforation in neonates: about 2 cases. . Gastroenterol clin biol 27: 1160-1162.
-
Fatima Zahra A, Maha O, Houria K, Younes T, Hasna B, et al. (2017) Idiopathic gastric perforation in neonates: about a case. Pan African Medical Journal 27:136.
-
Kothari P, Jiwane A, Kumar T, Deshmukh A, Kulkarni B (2002) Spontaneous gastroduodenal disruption in neonate. Pediatr Surg Int 18: 181-183.
-
Daniel B, Sobel MD (1998) Neonatal gastric perforation. Arch Pediatr Adolesc Med 152 : 599-600.
-
Lacusso C, Boscarelli A, Fusaro F, Bagolan P, Morini F (2018) Pathogenetic and prognostic factors for neonatal gastric perforation: Personal experience and systematic review of the literature. Frontiers in Pediatrics 6: 61.
-
Mihlouedo-Agbolan KA, Boumé MA, Adabra K, Sanni YS, Akakpo-Noumado GK, et al. (2014) Gastric perforations in children at the Sylvanus Olympio University Hospital in Lomé (Togo). J Afr Chir Ped 4: 185-193.
-
Chung MT, Kuo CY, Wang JW, Hsieh WS, Huang CB, et al. (1994) Gastric perforation in the neonate: clinical analysis of 12 cases. Acta Paediatr Sin 35: 460-465.
-
Rakoto-Ratsimba HN, Rakotoarisoa B, Samison LH, Belalahy V, Ranaivozanany A (2004) Spontaneous gastric perforation in a neonate: a case report. Archives de pediatrie 11(9): 1067-1069.
-
Nafatalewa DK, Misenga JB, Mbuya ME, Monga YP, Tshibangu MD, et al. (2018) Spontaneous neonatal gastric perforation: about a case. Pan African Medical Journal 30: 72.
-
Terui K, Iwai J, Yamada S, Takenouchi A, Nakata M, et al. (2012) Etiology of neonatal gastric perforation: a review of 20 years’ experience. Pediatr Surg Int 28(1): 9-14.
-
Jawed AJ, Al-Rabie A, Hadi A, Al-Sowailem A, Al-Rawaf A, et al. (2002) Spontaneous neonatal gastric perforation. Pediatr Surg Int 18(5-6): 396-399.
-
Govani DR, Patel RR, Patel RV, More B, Bhimni SD (2014) Pneumo-omentocele - a Sign of Silent Lethal Neonatal Posterior Gastric Perforation. Austin J Clin Case Rep 1(8): 1038.
-
Mallet EC, Robillard PY, Randrianaly H, Boumahni B, Edmar A, et al. (2000) Perforation gastrique néonatale spontanée. Arch pediatr 7(1): 94-95.
-
Tembely S, Dieth AG, Yaokreh JB, Soro L, Odehouri- Koudou TH, et al. (2013) Péritonite par perforation gastrique du nouveau-né. Rev Int Sc Med 15(2): 104-107.
-
Durham MM, Ricketts RR (1999) Neonatal gastric perforation and necrosis with Hunt-Lawrence pouch reconstruction. J Pediatr Surg 34(4): 649-651.
-
Kshirsagar AY, Vasisth GO, Ahire MD, Kanojiya RK, Sulhyan SR (2011) Acute spontaneus gastric perforation in neonates: A report of three cases. Afr J Paediatr Surg 8: 79-81.
- Understanding Pediatric Multiple Sclerosis: Clinical Presentation, Diagnostic Criteria, Therapeutic Advances, and Supportive Care Approaches
- Hemophilia in Children
- Xia-Gibbs Syndrome- A Case Report
- A Study to Assess Effectiveness of Play Therapy in Reducing Post-Operative Pain among Children Age 2 To 5 Year who have Undergone General Surgeries in Selected Pediatric Hospitals of Vadodara
- Preterm Birth: Scope of the Problem, Cost of Care, Potential Complications and Current Guidelines for Management
- Noradrenaline: Can we Use it to Manage Hemodynamic Instability among Neonatal Septic Shock at the NICU?