Neonatal Atrial Flutter: Adenosine Dilemma
Background: Atrial flutter (AFl) is a rare type of neonatal tachyarrhythmia, which is recognized by saw-tooth waves on electrocardiogram (ECG), and an atrial rate of up to 500 beats/minute. The mechanism of AFl is sustained by a macro-reentrant circuit pathway which is limited to the atrial wall, however the atrioventricular (AV) node is not involved of the reentrant circuit. Case Presentation: A 2-day-old, full term, male infant was born to a hypertensive mother, by cesarean section, presented to the pediatric emergency department at Maternity and Children hospital with history of cyanosis and decrease oral intake. At the physical examination, both tachypnea (70/min) and tachycardia (218/bpm) were determined. An electrocardiogram confirmed atrial flutter with 3:1 atrioventricular conduction. AFl didn’t respond to adenosine administration, therefore, electrical cardioversion was required. After conversion to normal sinus rhythm, amiodarone and propranolol therapy were started to maintain sinus rhythm afterward. With no further incidence of AFl or other arrhythmias, the infant was discharged at 9th day of life and in good general state with propranolol therapy, and was followed in the cardiac clinic. Conclusion: Electrical cardioversion with energy of (0.5-1 J/Kg) proved to be the most effective in establishing sinus rhythm, and is safe for neonatal patients. Adenosine doesn’t treat tachycardia of atrial origin, such as AFl. However, adenosine administration may help in identifying AFl, demonstrating the arrhythmia-characteristic saw-tooth waves in the ECG.
Emad Bamurshed1*, Abdullah Alsharif1, Ganadiel AlSulami2 and Enshrah Radwan1
Introduction
Neonatal arrhythmia is defined as an abnormal heart rhythm in the neonatal period [1]. There is no uniformity of classification for neonatal arrhythmias, some classify it according to the rhythm to tachyarrhythmias or bradyarrhythmias, and others classify it to benign non-life threatening arrhythmia and nonbenign arrhythmia which is sudden and need urgent recognition and treatment [2].
Supraventricular tachycardia (SVT) is considered a nonbenign rhythm, caused by re-entrant circuit in neonate [3], and is one of the most common arrhythmias in the neonatal period [2], where it present with a heart rate between 220-300 beats per minute (bpm) [3].
Atrial flutter (AFl) is a rare type of neonatal tachyarrhythmia, which is recognized by saw-tooth waves on electrocardiogram (ECG), and an atrial rate of up to 500 beats/minute [4]. The mechanism of AFl is sustained by a macro-reentrant circuit pathway which is limited to the atrial wall, however the atrioventricular (AV) node is not involved of the reentrant circuit [5].
Since the AV node is not involved in the re-entrant circuit, AV block doesn’t terminate AFl, and because of this, adenosine cannot terminate AFl but unmask the flutter waves by causing AV block [4, 6]. There are no large studies representing the incidence of AFl in the neonatal population [7]. The low incidence and small number of publications about the best treatment, and prognosis makes it difficult to carry out studies.
The aim of this study was determining the best treatment options, and prognosis. We also reviewed the literature regarding AFl in neonate. An informed consent was obtained from the parents.
Case Presentation
A 2-day-old, full term, male infant was born to a hypertensive mother, by cesarean section. At the physical examination, both tachypnea (70/min) and tachycardia (218/bpm) were determined.
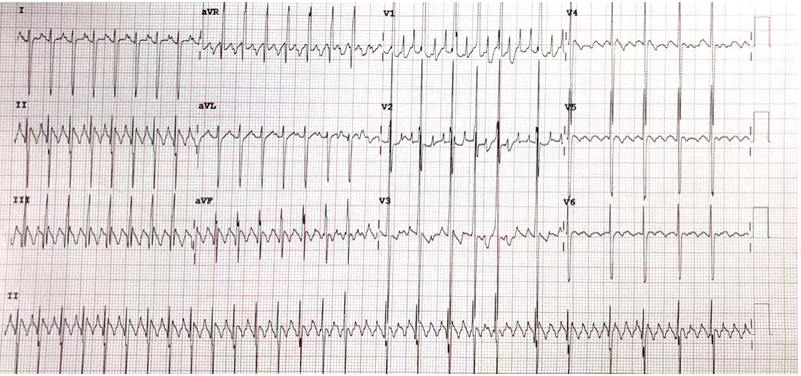
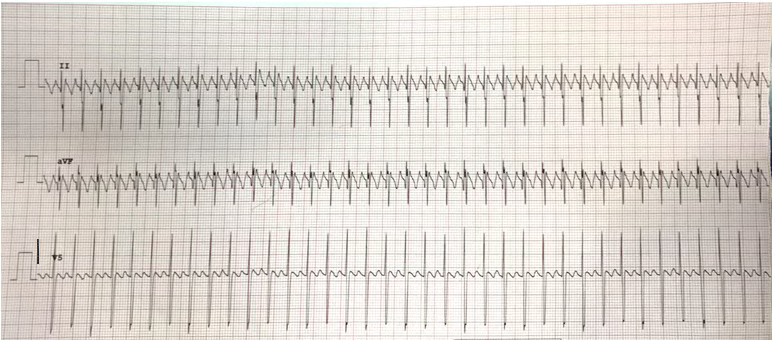
An electrocardiogram (ECG) was obtained in the emergency department which confirmed atrial flutter with 3:1 atrioventricular conduction, with atrial rate of 300 bpm, and a ventricular rate of 214 bpm. An echocardiogram showed small secundum atrial septal defect (ASD). The patient was admitted under the neonatal intensive care unit (NICU), and cardiology team was consulted regarding the AFl. Intravenous adenosine therapy was started with a dosage of 0.1 mg/kg for three times with no response. Amiodarone therapy with loading dose (5mg/kg) was initiated but, the infant’s blood pressure dropped to (38/25) so, amiodarone infusion was stopped, and cardiology team was contacted. Because of persistence of AFl, direct current cardioversion (1 J/kg) was performed for once. After conversion to normal sinus rhythm, amiodarone and propranolol therapy were started to maintain sinus rhythm afterward.
After 24 hours without AFl attack, intravenous amiodarone therapy was replaced with oral treatment. With no further incidence of AFl or other arrhythmias, the infant was discharged at 9th day of life and in good general state with propranolol therapy, and was followed in the cardiac clinic. AFl didn’t repeat in the time of follow-up, and cardiac evaluation was reported as normal (Figures 1 & 2).
Discussion
AFl in neonate may be resistance to first-line treatment, therefore, second-line agents such as cardioversion is required. Neonates with AFl are likely to be found born macrosomic or born to diabetic mothers [8], which wasn’t present in our case. The decision of treating the infant with intravenous adenosine, following failure of vagal maneuvers followed the pediatric advanced life support guidelines [9], as it is considered first line drug treatment in termination of SVT.
Our case didn’t respond to administration of adenosine and the heart rate remained between 220-230 bpm, similar reported cases showed no response to adenosine administration as well [10, 11, 12, 13]. Therefore, following discussion with the cardiology team, a decision was made to treat infant with synchronized direct current cardioversion.
According to two studies conducted by Casey FA, et al. [14] and Konak M, et al. [15] after administration of adenosine, the diagnosis of AFl was established, revealing classic flutter waves. Adenosine triphosphate is the first choice of drug for acute termination of SVT, and the mechanism of the drug is related to AV node block [16]. So, it does not convert AFl to sinus rhythm because the AV node is not involved in the reentrant circuit [4, 6].
A normal saline bolus of 10ml/kg was administered to this infant to rule out sinus tachycardia caused by hypovolemia, with no improvement. We used amiodarone, propranolol, and cardioversion. Our case was resistance to amiodarone, and AFl was stopped with cardioversion.
Amiodarone is reported to be effective in some cases of AFl as a premedication to cardioversion and to maintain sinus rhythm afterward [7, 17]. Direct current cardioversion is considered the most effective in establishing sinus rhythm with reported success rate to be around 90% [13]. The first successful direct current cardioversion of neonatal atrial flutter was reported in 1965 [18]. Therefore, it is being a good option for treatment.
The diagnosis is often simple with an ECG showing classic “saw tooth” pattern, better observed in leads ll, lll, aVF. The prognosis of neonatal AFl is often dependent on the presence or absence of congenital heart disease, however, neonatal AFl generally has a good prognosis once sinus rhythm is established, with low risk of recurrence, and a long-term antiarrhythmic medication is unlikely to be required.
Conclusion
In this reported case, electrical cardioversion with energy of 1J/Kg proved to be the most effective in establishing sinus rhythm, and is safe for neonatal patients. Adenosine doesn’t treat tachycardia of atrial origin, such as AFl, as described in this article. However, adenosine administration may help in identifying AFl, demonstrating the arrhythmia-characteristic saw-tooth waves in the ECG.
References
-
Isik DU, Celik IH, Kavurt S, Aydemir O, Kibar AE, et al. (2016) A case series of neonatal arrhythmias. J Matern Fetal Neonatal Med 29(8): 1344-1347.
-
McMullen SL (2016) Arrhythmias and Cardiac Bedside Monitoring in the Neonatal Intensive Care Unit. Crit Care Nurs Clin North Am 28(3): 373-386.
-
Woo J, Khan O, Caldarelli L, Williams P (2015) Tachycardia in the Neonate. Pediatr Ann 44(10): 247-250.
-
Ban JE (2017) Neonatal arrhythmias: diagnosis, treatment, and clinical outcome. Korean J Pediatr. 60(11): 344-352.
-
Jaeggi E, Ohman A (2016) Fetal and Neonatal Arrhythmias. Clin Perinatol 43(1): 99-112.
-
Roumiantsev S, Settle DM (2017) Atrial Flutter in the Neonate: A Case Study. Neonatal Netw 36(5): 313-317.
-
de Almeida MM, Tavares WGdS, Furtado MMAA, Fontenele MMFT (2016) Neonatal atrial flutter after the insertion of an intracardiac umbilical venous catheter. Rev Paul Pediatr 34(1): 132-135.
-
Pike JI, Krishnan A, Kaltman J, Donofrio MT (2013) Fetal and neonatal atrial arrhythmias: an association with maternal diabetes and neonatal macrosomia. Prenatal diagnosis 33(12): 1152-1157.
-
Maconochie IK, de Caen AR, Aickin R, Atkins DL, Biarent D, et al. (2015) Part 6: Pediatric basic life support and pediatric advanced life support: 2015 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations. Circulation 132(16 S1): 177-203.
-
Ergul Y, Ozturk E, Guzeltas A (2018) Atrial flutter and nonconducted bigeminy premature atrial contraction in a neonate with cardiac rhabdomyoma. Turk Kardiyol Dern Ars 46(4): 313-317.
-
Gulletta S, Rovelli R, Fiori R, Bella PD (2012) Multiple external electrical cardioversions for refractory neonatal atrial flutter. Pediatr Cardiol 33(2): 354-356.
-
Umeh M, Klutse T, Richards J, Kulkarni A (2017) Electrical direct current cardioversion for the treatment of atrial flutter in extremely premature neonate. Arch Dis Child Fetal Neonatal Ed 102(5): F466-F467.
-
Yilmaz-Semerci S, Bornaun H, Kurnaz D, Cebeci B, Babayigit A, et al. (2018) Neonatal atrial flutter: Three cases and review of the literature. Turk J Pediatr 60(3): 306-309.
-
Casey FA, McCrindle BW, Hamilton RM, Gow RM (1997) Neonatal atrial flutter: significant early morbidity and excellent long-term prognosis. Am Heart J 133(3): 302- 306.
-
Konak M, Alp H, Tarakci N, Baysal T, Ors R (2014) Successful treatment of atrial flutter with propafenone and synchronized cardioversion in a newborn. Indian J Pediatr 81(4): 413-414.
-
Camm AJ, Garratt CJ (1991) Adenosine and supraventricular tachycardia. N Engl J Med 325(23): 1621-1629.
-
Crochelet AS, Jacquemart C, Massin M (2015) [Repeated electrical cardioversions and amiodarone for recurrent neonatal atrial flutter]. Arch Pediatr 22(10): 1032-1034.
-
Hassenrueck A, Chojnacki B, Barker HJ (1965) Cardioversion of Auricular Flutter in a Newborn Infant. The American Journal of Cardiology 15(5): 726-731.
- Understanding Pediatric Multiple Sclerosis: Clinical Presentation, Diagnostic Criteria, Therapeutic Advances, and Supportive Care Approaches
- Hemophilia in Children
- Xia-Gibbs Syndrome- A Case Report
- A Study to Assess Effectiveness of Play Therapy in Reducing Post-Operative Pain among Children Age 2 To 5 Year who have Undergone General Surgeries in Selected Pediatric Hospitals of Vadodara
- Preterm Birth: Scope of the Problem, Cost of Care, Potential Complications and Current Guidelines for Management
- Noradrenaline: Can we Use it to Manage Hemodynamic Instability among Neonatal Septic Shock at the NICU?