Clinical and Chest Computed Tomography Features in Children with SARS-COV-2 Respiratory Infection
Objective: Pulmonary infections due to SARS-CoV-2 (severe acute respiratory syndrome coronavirus 2) virus have rapidly spread all over the world, causing a global pandemic. In this study, representation of clinical and radiological findings due to SARS-CoV-2 in pediatric patient population was aimed. Materials and Methods: Clinical and radiological results of 16 patients who admitted to our Pediatric Emergency Unit between March 2020 and January 2021, whose diagnosis of SARS-CoV-2 infection was confirmed by real-time reverse transcriptase polymerase chain reaction (RT-PCR) test, who had an appearance consistent with SARS-CoV-2 infection on chest computed tomography (CT) and followed-up in inpatient setting were examined retrospectively in this study. Results: Of these patients who were hospitalized with suspicion of SARS-CoV-2 infection; 35% underwent chest CT. 18% of these were found to have findings in CT of chest consistent with SARS-CoV-2 infection. The most common findings in chest CT included ground glass opacities in 15 (94%) patients and consolidations in 10 (62%) patients. The most common presenting symptoms were cough (62%), fever (44%), and dyspnea (44%). The median duration of hospital stay of the patients was 7 (5-16). Conclusion: Primary respiratory system involvement in SARS-CoV-2 and some limitations in RT-PCR tests and other radiological methods have made chest CT an auxiliary diagnostic method.
Introduction
The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection pandemic, which is caused by new coronavirus (COVID-19) and was first identified in Wuhan province of China, has led to many deaths and remains to be a very important health issue [1]. SARS-CoV-2 infection is usually presented with symptoms including fever, cough, respiratory distress, myalgia, and diarrhea in children, and rate of worsening and laboratory and radiological findings differ from those in adult patients [2].
Diagnosis of the disease is established by real-time reverse transcriptase polymerase chain reaction (RT-PCR) taken from a combined oropharyngeal-nasopharyngeal swab. This test is specific to the disease, although it has a sensitivity ranging between 30-60%, particularly early in the disease course [3]. Since these tests take time to result and unavailability of this test in some regions, other methods for early diagnosis have been sought. Primary respiratory system involvement in SARS-CoV-2 has made pulmonary examinations, particularly chest computed tomography (CT) a commonly preferred auxiliary diagnostic method [4]. Sensitivity of the chest CT procedure is quite higher compared to that of RT-PCR [5].
While there are several studies including radiological results of adult patients diagnosed with SARS-CoV-2, the literature including pediatric age group is still limited. In this study, clinical and radiological results of pediatric patients, whose diagnosis of SARS-CoV-2 infection was confirmed by real-time reverse transcriptase polymerase chain reaction (RT-PCR) test, who had an appearance consistent with SARS- CoV-2 infection on CT of chest and followed-up in inpatient setting, were reported.
Materials and Methods
Study Design and Data Collection
The study was conducted in a single center (University of Health Sciences, Bursa City Training and Research Hospital, Department of Pediatrics) as a retrospective observational cohort study. Pediatric patients under 18 years of age whose diagnosis of SARS-CoV-2 infection was confirmed by real- time reverse transcriptase polymerase chain reaction (RT- PCR) test between 15.03.2020-31.12.2020, who had an appearance consistent with SARS-CoV-2 infection on chest CT and followed-up in inpatient setting were included in the study.
Patient’s records entered in the hospital’s electronic system and admission files were examined retrospectively after approvals from local ethics committee and Ministry of Health was obtained. The patients who were above 18 years of age, whose files could not be reached, or who had files with severe lack of knowledge were excluded from the study.
All patients were evaluated in terms of epidemiological and demographic data, as well as laboratory and radio diagnostic tests, and treatment features and outcomes. These data were reviewed by two trained physicians (MFK and SEB).
Procedures
Diagnosis, follow-up, and treatment of COVID-19 were carried out in accordance with recommendations in the guideline published by Republic of Turkey Ministry of Health Science Committee [6]. Combined naso-oropharyngeal RT- PCR swab samples were taken from the patients meeting the criteria.
From the patients from whom samples were taken, complete blood count, serum biochemical test (including renal and liver function, lactate dehydrogenase, and electrolytes), myocardial enzymes, coagulation profile, erythrocyte sedimentation rate, C-reactive protein, and procalcitonin were requested at admission. The patients underwent posteroanterior chest x-ray. The patients whose respiratory findings could not be explained by chest x-ray or who had clinical worsening, however, underwent chest CT. All the images were stored in the picture archiving and communication system and reviewed by an experienced radiologist. The CT features were evaluated as follows: a) Ground glass opacities, b) Consolidations, c) Crazy-paving, d) Vascular Engorgement, e) Air bronchograms, f) Bronchial wall thickening and bronchiectasis, g) Reticulation, h) Subpleural lines, linear opacities, i) Fibrosis, j) Halo sign and nodules and k) Pleural thickening.
A control RT-PCR swab samples were taken at 48th hour of hospitalization in patients followed-up in an inpatient setting and their follow-up continued until detection of a negative result. The discharge criteria were absence of fever at least 48 hours, substantial improvement in both laboratory tests and clinical remission of respiratory symptoms, and at least one negative sample for SARS-CoV-2 RT-PCR.
The treatment protocol of hospitalized patients included general supportive care; monitoring of pulmonary, hepatic, renal, and cardiac functions; active control of high temperature; anti biotherapy; hydroxychloroquine or antiviral treatment if the patient had lung-related clinical worsening and oxygen support (delivery of oxygen with nasal cannula at a rate of 2-4 lt/min in patients with an oxygen saturation of <92% in the room air), and administration of systemic and inhaled corticosteroids.
Results
During this period, there were a total of 35,158 admissions to our pediatric emergency unit. Number of patients from whom RT-PCR samples were taken on the suspicion of SARS-CoV-2 infection was 6,971 (20%). 1,745 (25%) positive results were detected in the samples taken. All cases had at least one family member positive for SARS- CoV-2 infection.
Of the patients hospitalized with detected SARS-CoV-2
infection; 86 (35%) underwent chest CT. Patients (18%), however, were found to have findings on chest CT suggestive of SARS-CoV-2 infection. The most common presenting complaints were cough (62%), fever (44%), and dyspnea (44%). None of our patients were determined to have any neurological finding or evidence of cardiac, hepatic, or renal failure.
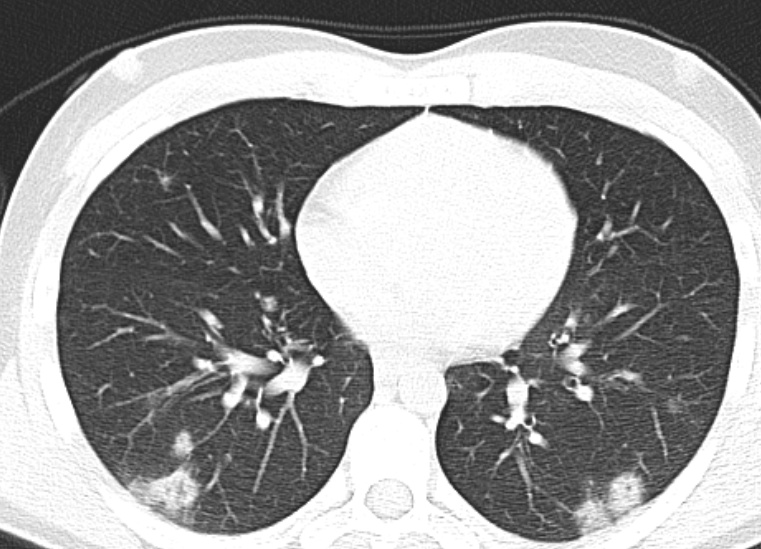
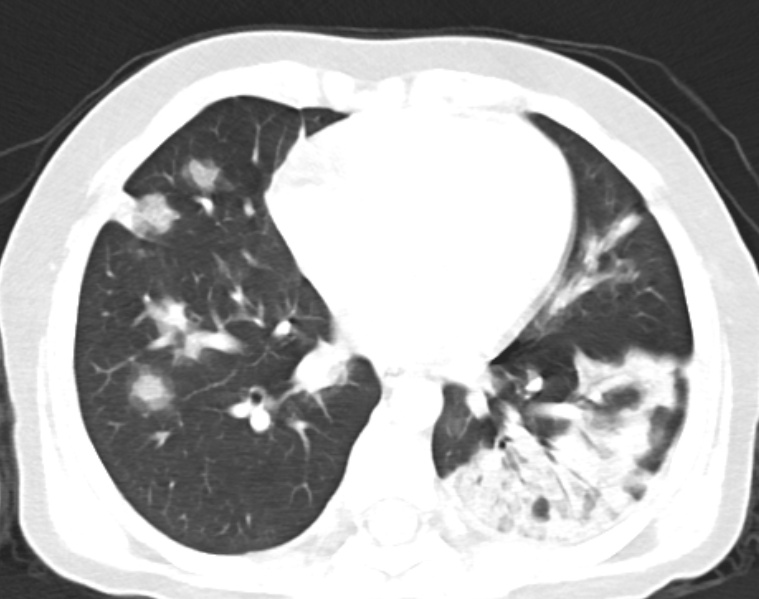
When laboratory findings of the cases were examined, it was observed that three (19%) patients had neutropenia and six had (38%) lymphopenia. No significant increase was observed in C-reactive protein results. When findings in chest CT of the cases were examined, the most common findings were ground glass opacities in 15 (94%) patients and consolidations in 10 (62%) patients (Figures 1-3).

None of the patients included in our study required admission to pediatric intensive care unit. Median duration of hospital stay of the patients was 7 (5-16) days. All patients were discharged with cure without developing any complications. Summary of demographic, clinical features and chest CT findings of pediatric patients with SARS-CoV-2 were presented in (Table 1).
| Patient | Gender | Age | Presenting History | Days from Admission | CRP at Admission, mg/L | WBC, x109/L | Lenfo cyte, x109/L | Chest CT Findings | Length of Hospi tal stay | Treatment |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | F | 17 y | Cough, dyspnoea | 2 | 10.1 | 8.24 | 3.41 | Ground glass opacities, consolidation, vascular engorgement | 8 days | Antibiotics |
| 2 | F | 15 y | Fever, cough, myalgia | 4 | 0.6 | 5.44 | 1.18 | Ground glass opacities, consolidation | 16 days | Antibiotics, hydroxy chloroquine, oxygen inhalation |
| 3 | M | 17 y | Fever, cough, dyspnoea | 2 | 0.1 | 6.54 | 2.54 | Ground glass opacities, consolidation | 5 days | Antibiotics |
| 4 | M | 17 y | Vomiting, diarrhea | 2 | 15.3 | 11.94 | 0.87 | Ground glass opacities, subpleural lines | 9 days | Antibiotics, antivirals |
| 5 | M | 17 y 3 m | Fever, inability to taste | 3 | 3 | 3.79 | 1.41 | Ground glass opacities, consolidation | 7 days | Antibiotics, antivirals |
| 6 | M | 13 y | Asymptomatic | 8.2 | 3.46 | 1.58 | Ground glass opacities, consolidation | 10 days | Antibiotics, hydroxychloroquine | |
| 7 | M | 15 y 4 m | Fever, dyspnoea | 3 | 0.7 | 8.13 | 2.77 | Ground glass opacities, vascular engorgement | 6 days | Antibiotics, hydroxychloroquine |
| 8 | M | 9 y 6 m | Fever, cough | 3 | 25.7 | 7.45 | 1.82 | Ground glass opacities, consolidation, crazy-paving, vascular engorgement, air bronchograms, pleural thickening | 8 days | Antibiotics, hydroxychloroquine |
| 9 | M | 16 y | Fever, cough | 2 | 10.8 | 4.14 | 0.72 | Ground glass opacities | 6 days | Antibiotics, antivirals |
| 10 | M | 14 y | Fever, cough, myalgia | 3 | 4.5 | 3.63 | 1.49 | Ground glass opacities, consolidation, crazy- paving, air bronchograms, halo sign, pleural thickening | 6 days | Antibiotics, hydroxychloroquine |
| 11 | F | 17 y 5 m | Dyspnoea | 2 | 2 | 5.77 | 1.92 | Consolidation | 8 days | Antivirals |
| 12 | M | 11 y | Cough, dyspnoea | 5 | 1.6 | 6.95 | 3.2 | Ground glass opacities | 5 days | Antibiotics, inhaled corticosteroids, oxygen inhalation |
| 13 | M | 12 y | Cough | 1 | 0.4 | 8.44 | 3.54 | Ground glass opacities | 5 days | Antibiotics |
| 14 | F | 17 y 4 m | Cough, myalgia, dyspnoea | 5 | 0.5 | 4.8 | 1.64 | Ground glass opacities | 5 days | Antibiotics |
| 15 | F | 13 y | Fatigue, dyspnoea | 3 | 5.1 | 4.17 | 1.06 | Ground glass opacities, consolidation | 10 days | Antibiotics, hydroxychloroquine |
| 16 | F | 16 y 6 m | Cough | 7 | 2.1 | 4.97 | 2.88 | Ground glass opacities, consolidation, air bronchograms | 7 days | Antibiotics, antivirals |
Table 1: Summary of demographic, clinical features and chest CT findings of pediatric patients with SARS-COV-2.
Abbreviations: CRP: C-reactive protein; CT: Computed tomography; F: Female; M: Male; m: months; WBC: White blood cell; y: years. Table 1: Summary of demographic, clinical features and chest CT findings of pediatric patients with SARS-COV-2.
Discussion
Although many epidemiological, clinical and radiological studies on SARS-CoV-2 pneumonia have been carried out, a very few of these studies include pediatric patients. This may be because pediatric patients usually had an asymptomatic or milder clinical course and CT examinations are not routinely recommended in children due to radiation exposure.
Chest x-ray is the imaging method of choice particularly for pediatric patients, as it is easy to perform, has the possibility of bed-side imaging with portable devices and emits lower dose of radiation. However, its sensitivity seems to be lower compared to that of CT, especially early in the disease and in patients with mild pneumonia [7]. Bilateral peripheral consolidations and ground glass opacities are the most common findings [8].
Although ultrasonography is recommended especially for children and pregnant women regarding triage due to some advantages like not emitting radiation and possibility of bed-side imaging, it has not been clarified due to risk of spread of infection and requiring experience of performed [9, 10].
Reduction of sensitivity of SARS-CoV-2 RT-PCR tests up to 60%, limited availability of the test and failure to get the desired results with the other aforementioned radiological methods have created urgent need for an alternative diagnostic tool. In this case, potential of chest CT to be used as a helpful and screening tool for suspected patients has arisen [11]. CT findings of SARS-CoV-2 pneumonia vary among pediatric patients and ground glass opacities, which are considered as findings of mild pneumonia, are common findings [12]. The predominant pattern is presence of ground glass opacities usually in lower lobes rather than in centrilobular or peribronchial areas, unlike in adults [3]. In addition, isolated consolidations, consolidations accompanying ground glass opacities or interlobular septal thickenings are seen in children [13]. Although mild cases are common in children, clinical pictures may worsen in some patients. In these patients, the ground glass opacities may enlarge, transforming into multiple consolidations. Furthermore, interstitial pulmonary changes different from the previous ones may occur [14]. In very rare cases, diffuse pulmonary consolidation develops and the appearance of “white lung” is observed. In resorption phase, the lung lesions may completely resolve or leave minimal linear opacities [15].
In our study, most common findings in chest CT of the cases were ground glass opacities in 15 (94%) patients and consolidations in 10 (62%) patients. Ground glass opacities are the most common involvement with a rate of up to 98% especially in adults, which is usually observed early in the disease or mild pneumonia. Although it may be unilateral, it is mostly observed as bilateral, multifocal, and adjacent to visceral pleural surfaces, including the fissures [16, 17]. Consolidations, however, are usually observed late in the disease course, 10-12 days after onset of the symptoms. They are most commonly bilateral, multifocal and located adjacent to visceral pleural surfaces including the fissures. They usually co-exist with ground glass opacities [18]. Apart from these findings, our patients were found to have appearances of vascular engorgement, crazy-paving, air bronchograms, pleural thickening, and halo sign. Atypical findings such as cavitation, tree-in-bud pattern, pleural effusion, and lymphadenopathy were not observed [19].
Absence of complications or need for admission to pediatric intensive care unit in all patients included in our study and a 7-day median duration of hospital stay of the cases support milder clinical findings, more common normal imaging and milder pneumonia in children compared to adults, as reported by previous studies.
Our study has some limitations. The sample size was relatively small because COVID-19 is less common in children and their rate of admission to hospital and undergoing chest CT is lower, as they have milder symptoms. The single-center and retrospective design of our study are another limitations. The fact that the clinical, laboratory and radiological results evaluated in our study were the results obtained only at admission to hospital and absence of follow-up results in another limitation. We are in thought of that better understanding of effectiveness of chest CT in children will be provided in the future with multi-center studies conducted with larger patient groups.
Conclusion
The SARS-CoV-2 infection has a milder course in pediatric patients compared to adults. Findings in chest CT in children usually include ground glass opacities and consolidations, and atypical findings in chest CT are rarely observed.
Clinical and laboratory tests for SARS-CoV-2 infection are nonspecific. Limitations of RT-PCR tests and other radiological methods make chest CT important for early and accurate diagnosis. Considering radiation exposure, low- dose chest CT, if possible, will be an important diagnostic tool in selected pediatric cases.
Disclosure of Interest
The authors declare that they have no competing interest.
References
-
Nino G, Zember J, Sanchez‐Jacob R , Gutierrez MJ, Sharma K, et al. (2021) Pediatric lung imaging features of COVID‐19: A systematic review and meta‐analysis. Pediatric Pulmonology 56(1): 252-263.
-
Xia W, Shao J, Guo Y, Peng X, Li Z, et al. (2020) Clinical and CT features in pediatric patients with COVID-19 infection: Different points from adults. Pediatr Pulmonol 55(5): 1169-1174.
-
Duan YN, Zhu YQ, Tang LL, Qin J (2020) CT features of novel coronavirus pneumonia (COVID-19) in children. Eur Radiol 30(8): 4427-4433.
-
Pekcevik Y, Belet U (2020) Patient Management in the Radiology Department, the Role of Chest Imaging During the SARS-CoV-2 Pandemic and Chest CT Findings Related to COVID-19 Pneumonia. The Journal of Tepecik Education and Research Hospital 30: 195-212.
-
Fang Y, Zhang H, Xie J, Lin M, Ying L, et al. (2020) Sensitivity of Chest CT for COVID19: Comparison to RT- PCR. Radiology 296(2): E115-E117.
-
Korkmaz MF, Ture E, Dorum BA, Kilic ZB (2020) The Epidemiological and Clinical Characteristics of 81 Children with COVID-19 in a Pandemic Hospital in Turkey: an Observational Cohort Study. J Korean Med Sci 35(25): e236.
-
Wong HYF, Lam HYS, Fong AH, Leung ST, Chin TWY, et al. (2020) Frequency and Distribution of Chest Radiographic Findings in COVID-19 Positive Patients. Radiology 296(2): E72-E78.
-
Ai T, Yang Z, Hou H, Zhan C, Chen C, et al. (2020) Correlation of Chest CT and RT-PCR Testing in Coronavirus Disease 2019 (COVID-19) in China: A Report of 1014 Cases. Radiology 296(2): E32-E40.
-
Soldati G, Smargiassi A, Inchingolo R, Buonsenso D, Perrone T, et al. (2020) Is there a role for lung ultrasound during the COVID-19 pandemic? J Ultrasound Med 39(7): 1459-1462.
-
Ture E, Korkmaz MF, Aksoy FD, Demirbas BC, Menekse B, et al. (2021) Point-of-care lung ultrasound findings in the pediatric emergency clinic during the COVID-19 pandemic. J Clin Ultrasound 49(2): 85-90.
-
Goyal M, Sen KK, Panda S, Jagadeesh K, Dubey R, et al. (2021) HRCT Chest Imaging in Pediatric, Adult, and Geriatric COVID-19 patients, with analysis of clinical presentation- A study conducted in Odisha COVID Hospital, KIMS, India. International Journal of Health and Clinical Research 4(4): 133-139.
-
Caro-Dominguez P, Shelmerdine SC, Toso S, Secinaro A, Toma, et al. (2020) Thoracic imaging of coronavirus disease 2019 (COVID-19) in children: a series of 91 cases. Pediatric Radiology 50(10): 1354-1368.
-
Ma H, Shao J, Wang Y, Zhai A, Zheng N, et al. (2020) High resolution CT features of novel coronavirus pneumonia in children. Zhonghua Fang She Xue Za Zhi 54: E002.
-
Chen F, Liu ZS, Zhang FR, Chen Y, Cheng XF, et al. (2020) First case of severe childhood novel coronavirus pneumonia in China. Zhonghua Er Ke Za Zhi 58(3): 179- 182.
-
Li HJ, Liu SY, Xu HB, Cheng JL (2020) Guideline for medical imaging in auxiliary diagnosis of coronavirus disease 2019. Chin J Med Imaging Technol 36(3):321- 331.
-
Prokop M, van Everdingen W, van Rees Vellinga T, van Ufford HQ, Stoger L, et al. (2020) CO-RADS - A categorical CT assessment scheme for patients with suspected COVID-19: definition and evaluation. Radiology 296(2): E97-E104.
-
Liang T, Liu Z, Wu CC, Jin C, Zhao H, et al. (2020) Evolution of CT findings in patients with mild COVID-19 pneumonia. Eur Radiol 30(9): 4865-4873.
-
Ding X, Xu J, Zhou J, Long Q (2020) Chest CT findings of COVID-19 pneumonia by duration of symptoms. Eur J Radiol 127:109009.
-
Kanne JP (2020) Chest Ct findings in 2019 novel coronavirus (2019-NCoV) infections from Wuhan, China: Key points for the radiologist. Radiology 295(1): 16-17.
- Understanding Pediatric Multiple Sclerosis: Clinical Presentation, Diagnostic Criteria, Therapeutic Advances, and Supportive Care Approaches
- Hemophilia in Children
- Xia-Gibbs Syndrome- A Case Report
- A Study to Assess Effectiveness of Play Therapy in Reducing Post-Operative Pain among Children Age 2 To 5 Year who have Undergone General Surgeries in Selected Pediatric Hospitals of Vadodara
- Preterm Birth: Scope of the Problem, Cost of Care, Potential Complications and Current Guidelines for Management
- Noradrenaline: Can we Use it to Manage Hemodynamic Instability among Neonatal Septic Shock at the NICU?