Keratitis Ichthyosis Deafness Syndrome and Communication Disorders: A Case Report
Keratitis-Ichthyosis Deafness (KID) syndrome is an atypical genetic, multi-system disorder characterised by defects of corneas surface, thickened plaques of skin and sensorineural hearing impairment. As it is a multifaceted syndrome, children with KID require a comprehensive examination of all the affected systems, including continuous monitoring of speech and language abilities, as it is associated with sensorineural hearing impairment. However, the KID syndrome being a rare condition, the speech, language and hearing abilities are less explored. Thus, it is attempted to portray those speech, language and hearing abilities affected in them by describing a case report of a 5-year old child diagnosed with KID syndrome. This case report also highlighted on the importance of early identification and rehabilitation in such cases
Introduction
KID syndrome, also known as Deafness Syndrome, is a rare genetic congenital disorder with the clinical signs of hearing loss, dry scaly skin and progressive vascularised keratitis [1]. To date, no more than 100 cases are reported in the literature with the incidence of <1 in 100,000 live births [2]. Earlier evidence reports that the mutation of the connexin-26 gene (GJB2) localised on chromosome 13 throughout the body, including the inner ear, gives rise to the clinical traits symptoms [3, 4]. Among the affected children, 90% to 93% have reported a pre-lingual bilateral sensorineural hearing loss of severe to profound degree [2, 5, 6].
The syndrome can be identified based on the physical appearance of skin scaling and erythroderma [1] that expedite early identification of hearing loss. However, it has been observed that, the early initiation of treatment/ rehabilitation is not carried out, it leads to a delay in speech- language and learning skills, poor social interaction, and lack of academic abilities. This case report emphasised the importance of early identification and rehabilitation by highlighting the child’s speech, language, and hearing skills.
Case Report
A 5-year old female child diagnosed with KID syndrome reported with limited speech output and hard of hearing. On observation, the child had dry scaly skin (Figure 1) and there was a limited auditory response during the general conversation. Parents reported that the child had no significant prenatal, natal or post-natal abnormalities. However, second-degree consanguinity was reported with no hereditary conditions running in the families. Unlike the literature reports, the child had no visual abnormality. The child was subjected to audiological evaluation, oro-motor examination, and speech-language assessment.

Audiological Assessment
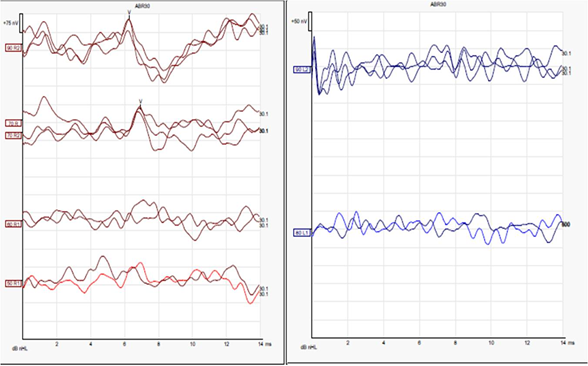
Behavioural conditioning audiometry was performed initially to measure the severity of the child’s hearing ability. However, due to the child’s poor performance on behavioural tests, the physiological tests were administered, including immittance, otoacoustic emission (OAE), and Auditory Brainstem Response (ABR). Results of 226 Hz Tympanometry showed ‘A’ type in the right ear, suggesting normal functioning and ‘Cs’ type in the left ear, indicating negative pressure in the middle ear. The outer hair cell’s integrity in the inner ear assessed using OAE showed poor signal-to-noise ratio confirming outer hair cell dysfunction in the right ear. On the other hand, the outer hair-cell integrity could not be established in the left ear due to the indication of middle ear dysfunction. Acoustic reflex threshold (ART) and ABR were performed to check the auditory pathway’s integrity and the severity of the hearing loss. ART showed no response between 500 Hz and 4000 Hz in both ipsilateral and contralateral pathways. ABR responses for click stimulus were presented till 70 dBnHL in right ear, indicating a moderate hearing loss in the right ear and absence at 90 dBnHL in the left ear, indicating severe hearing loss (Figure 2). Overall, the audiological evaluation indicated a cochlear hearing loss, and the child was fitted with Behind-The-Ear digital hearing aid on both sides. Post-hearing aid fitting, it was recommended to get the speech-and language assessment.
Speech and Language Assessment
A few studies have reported abnormal teeth and palate structure that could impair speech production in KID syndrome [7]. However, in the child, no oral structural and functional abnormalities were observed. Thus, the delay in the child’s speech and language skills could be due to the presence of sensorineural hearing loss. ‘Scales of early communication skill for hearing impaired’ test was administered to assess the child’s current receptive and expressive language abilities. It was found that the receptive and expressive language ages ranged from 2 to 2.11 years. The child could comprehended gestures and had produced a few non-meaningful utterances such as /avva:/, /abba:/.
Discussion
Earlier studies have shown that the onset of the problem varies, and the features are progressive in nature [1, 6, 8]. In the present case study, the child had no significant clinical trait apart from scaly skin and hearing loss. It is well-established that normal hearing is critical for the development of speech and language skills. In addition, the literature also highlights the importance of early identification and rehabilitation [9, 10]. Untreated hearing loss has shown to cause an adverse effect on the children’s speech-language development, leading to poor academic performance and delays in acquiring linguistic, social, and sensory capabilities [11, 12]. The literature also indicates confirmed progressive hearing loss in such children [6, 8]. Thus, immediate intervention in terms of fitting of hearing aids/ cochlear implant and a specialised speech-language therapy are of utmost necessity in children with KID syndrome. However, genetic diagnostic testing is warranted to confirm the clinical diagnosis of KID syndrome.
Secondly, language learning requires good visual ability. Literature reports that about 80% of children with KID syndrome develop vision loss either in the pre-lingual or later stages [13]. However, due to the absence of such vision abnormalities in the current child, the prognosis is predicted to be better.
Conclusion
The available literatures on KID syndrome have majorly focused on medical treatment, whereas the present study emphasises on the importance of early identification and timely rehabilitation for acquiring age-appropriate speech and language skills. This accentuates the urgent need for appropriate recommendation and monitoring of the clinical presentations in terms of their severity and outcomes. In addition, the involvement of audiologist and speech- language pathologists in either the multi-disciplinary or inter-disciplinary team could support children with KID syndrome to improve their speech, language and hearing abilities. Future studies are required to monitor the effect of rehabilitation at different levels of severity and other associated problems. Also, replication of such case studies would validate the results of the present study.
References
-
Shanker V, Gupta M, Prashar A (2012) Keratitis Ichthyosis Deafness syndrome: A rare congenital disorder. Indian Dermatol Online J 3(1): 48-50.
-
Caceres Rios H, Tamayo Sanchez L, Duran Mckinster C, De La Luz Orozco M, Ruiz-Maldonado R (1996) Keratitis, ichthyosis, and deafness (KID syndrome): Review of the literature and proposal of a new terminology. Pediatr Dermatol 13(2): 105-113.
-
Maintz L, Betz RC, Allam JP, Wenzel J, Jaksche A, et al. (2005) Keratitis ichthyosis deafness syndrome in association with follicular occlusion triad. Eur J Dermatol 15(5): 347-352.
-
Richard G, Brown N, Rouan F, Bale SJ, Jouni U, et al. (2003) Genetic heterogeneity in erythrokeratodermia variabilis: Novel mutations in the connexin gene GJB4 (Cx30.3) and Genotype-phenotype correlations. J Invest Dermatol 120(4): 601-609.
-
Sundaram S, Willoughby C, Itin P (2003) The clinical spectrum of Keratitis Ichthyosis Deafness syndrome. J Invest Dermatol 121: A660.
-
Szymko Bennett YM, Russell LJ, Bale SJ, Griffith AJ (2002) Auditory manifestations of Keratitis-Ichthyosis-Deafness (KID) syndrome. Laryngoscope 112(2): 272-280.
-
De Raeve L, Bonduelle M, Deconinck H, Roseeuw D, Stene JJ (2008) Trichothiodystrophy like hair abnormalities in a child with keratitis ichthyosis deafness syndrome. Pediatr Dermatol 5(4): 466-469.
-
Lamprecht A, Goecke T, Anton Lamprecht I, Kuster W (1988) Progressive erythrokeratodermia and cochlear hearing impairment. A case report and review of the literature. Int J Pediatr Otorhinolaryngol 15(3): 279-289.
-
Giuntini G, Forli F, Nicastro R, Ciabotti A, Bruschini L, et al. (2016) Early care in children with permanent hearing impairment. Acta Otorhinolaryngol Ital 36(1): 51-59.
-
Fulcher A, Purcell AA, Baker E, Munro N (2012) Listen up: Children with early identified hearing loss achieve age-appropriate speech/language outcomes by 3years- of-age. Int J Pediatr Otorhinolaryngol 76(12): 1785- 1794.
-
Yoshinaga Itano C, Sedey AL, Coulter DK, Mehl AL (1998) Language of early- and later-identified children with hearing loss. Pediatrics 102(5): 1161-1171.
-
Moeller MP (2000) Early intervention and language development in children who are deaf and hard of hearing. Pediatrics 106(3): e43.
-
Messmer EM, Kenyon KR, Rittinger O, Janecke AR, Kampik A (2005) Ocular manifestations of keratitis- ichthyosis-deafness (KID) syndrome. Ophthalmology 112(2): 1-6.
- Understanding Pediatric Multiple Sclerosis: Clinical Presentation, Diagnostic Criteria, Therapeutic Advances, and Supportive Care Approaches
- Hemophilia in Children
- Xia-Gibbs Syndrome- A Case Report
- A Study to Assess Effectiveness of Play Therapy in Reducing Post-Operative Pain among Children Age 2 To 5 Year who have Undergone General Surgeries in Selected Pediatric Hospitals of Vadodara
- Preterm Birth: Scope of the Problem, Cost of Care, Potential Complications and Current Guidelines for Management
- Noradrenaline: Can we Use it to Manage Hemodynamic Instability among Neonatal Septic Shock at the NICU?