Direct Inguinal Hernia in Pediatrics: Two case reports
Pediatric inguinal hernia occurs due to failure of closure of processus vaginalis. Aim of the procedure of indirect type in pediatrics is complete ligation of the sac. Direct and femoral hernias are extremely rare in pediatrics which could be easily detected from inside the abdomen especially during laparoscopic management. We present two rare cases of direct inguinal hernia.
Introduction
Inguinal hernia in Pediatrics is classified as indirect type as it is the most common variant in this age group [1, 2]. We had two rare cases; an infant had bilateral direct inguinal hernia and a two-year -old patient had both direct and indirect hernia at the right side.
Case 1
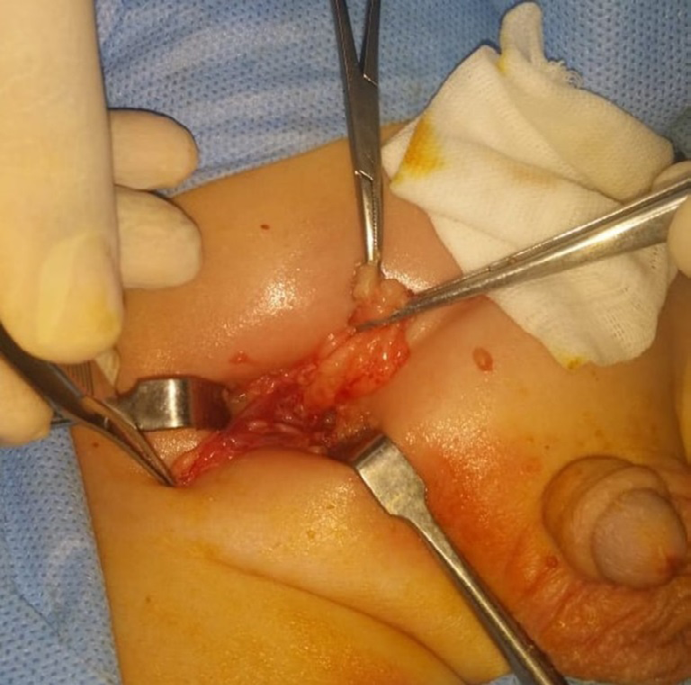
A one-year-old boy attended at our department as a case of bilateral inguinal hernia. He underwent open bilateral inguinal incisions which revealed bilateral direct inguinal hernia containing fat medial to inferior epigastric vessels and away from the cord Figures 1 and 2.
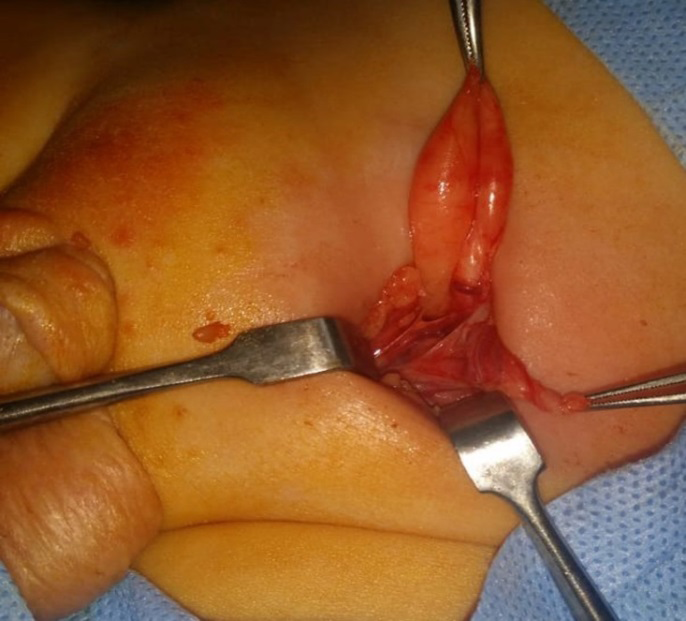
Our aim was changed into inversion of the sac inward, repairing and reinforcing the posterior inguinal wall. After inverting the sac, the transversalis fascia was plicated beside repairing both conjoint tendon and reflected part of the inguinal ligament.
Case 2
A two-year-old boy had right inguinal hernia. He underwent open right inguinal incision which showed both hernia sac within the cord contents and direct hernia in form of fatty bulge of the medial fossa of posterior inguinal wall medial to inferior epigastric vessels and away from the cord but with narrow neck Figure 3.

Consequently, herniotomy of both sacs was done followed by plication of the transversalis fascia beside repairing both conjoint tendon and reflected part of inguinal ligament. Both patients had a smooth postoperative course and follow up without recurrence.
Discussion
In Pediatrics, direct inguinal hernia is rare. Its incidence is about 0.2–1.2% of all inguinal hernias [3, 4]. It commonly occurs in males, and the right side [4]. Fonkalsrud or others illustrated the causes of direct inguinal hernia: (1) attenuation of transversalis fascia, (2) increased abdominal pressure, and (3) weakness of the internal inguinal ring due to the previous surgery for indirect inguinal hernia. Wright divides the direct hernia into five based on the findings from the inguinal region [5, 6]. Preoperatively, the correct diagnosis rate of indirect hernia constitutes 38%, and it is usually missed even intraoperatively [5]. The laparoscopic management is supposed to be a better intervention for proper visualization of direct inguinal and femoral hernia defects. In our cases, preoperative diagnosis is an indirect hernia; however, direct hernia was detected intraoperatively. The treatment of direct hernia is different in each facility. Some authors recommend Bassini repair [4, 5] and some recommend McVay repair for femoral hernia [6]. We misunderstood our cases as an indirect inguinal hernia prior to the operation.
Most pediatric surgeons prefer the open approach. Recently, laparoscopic management technique reported in children which has the advantage of defects visualization [7, 8]. We consider direct hernia repair in form of the closure of the hernia defect without tension, following the resection of lipoma with the hernia sac if possible or the inversion of the sac followed by reinforce of the posterior wall then Bassini repair if possible.
Conclusion
Pediatric inguinal swelling could be a rare type as direct or femoral hernia rather than the indirect type. These types are rarely detected preoperatively. Laparoscopy could be a possible option foe better visualization and repair of these rare types.
References
-
Endo M, Ukiyama E (2004) Laparoscopic Closure of Patent Processus Vaginalis in Girls with Inguinal Hernia Using a Specially Devised Suture Needle. Pediatric Endosurgery & Innovative Techniques 5(2): 187-191.
-
Takehara H, Yakabe H, Kameoka K (2006) Laparoscopic Percutaneous Extra corponeal Closure For Inguinal Hernia in Children Clinical Outcome of 972 Repairs Done in 3 Pediatric Surgical Institutions. J Pediatr Surg 41(12): 1999-2003.
-
Schier F (2000) Direct Inguinal Hernias in Children Laparoscopic Aspects. Pediatr Surg Int 16(8): 562-564.
-
Wright J (2004) Direct Inguinal Hernia in Infancy and Childhood. Pediatric Surgery International 9: 161-163.
-
Fonkalsrud EW, Delorimier AA, Clatworthy HW Jr (1965) Femoral and Direct Inguinal Hernias in Infants and Children. JAMA 192: 597-599.
-
Viidik T, Marshall DG (1980) Direct Inguinal Hernias in Infancy and Early Childhood. J Pediatr Surg 15(5): 646- 647.
-
De Caluwe D, Chertin B, Puri P (2003) Childhood Femoral Hernia a Commonly Misdiagnosed Condition. Pediatr Surg Int 19(8): 608-609.
-
Tainaka T, Uchida H, Ono Y, Tanano A, Shirota C, et al. (2015) A New Modification of Laparoscopic Percutaneous Extraperitoneal Closure Procedure for Repairing Pediatric Femoral Hernias Involving a Special Needle and a Wire Loop. Nagoya J Med Sci 77(3): 531- 535.
- Understanding Pediatric Multiple Sclerosis: Clinical Presentation, Diagnostic Criteria, Therapeutic Advances, and Supportive Care Approaches
- Hemophilia in Children
- Xia-Gibbs Syndrome- A Case Report
- A Study to Assess Effectiveness of Play Therapy in Reducing Post-Operative Pain among Children Age 2 To 5 Year who have Undergone General Surgeries in Selected Pediatric Hospitals of Vadodara
- Preterm Birth: Scope of the Problem, Cost of Care, Potential Complications and Current Guidelines for Management
- Noradrenaline: Can we Use it to Manage Hemodynamic Instability among Neonatal Septic Shock at the NICU?