Socioeconomic Attributes and Barriers to Healthcare Access: A Perspective of Dependency
It is well documented that people in a low socioeconomic hierarchy have lesser healthcare access than those higher on the hierarchy. However, cases of non-access to healthcare are also observed among those who are at the top of the socioeconomic hierarchy. The main reason is their dependency on others and therefore, healthcare access also needs to be studied from the perspective of dependency on others. The study discusses healthcare access from the perspective of dependency in the context of socioeconomic attributes and barriers. The discussion is mainly based on the existing literature. The attributes such as ‘age’, ‘gender’ and ‘disability’ and the related four kinds of individuals such as children, disabled men, old age men, and women with threshold levels of best socioeconomic attributes at which the dependency still prevents them from healthcare access. Therefore, two corrective measures are necessary here. First, the family and social support and second, the government intervention. Hence, the sociological and behavioural approaches are necessary to incorporate into health policy along with institutional supports like quality health infrastructure and financial protection provisions for equitable healthcare for all.
Abbreviations
UBI: Universal Basic Income; WHO: World Health Organization.
Introduction
A lot of studies are available on the association between socioeconomic attributes and healthcare access. An uneven distribution of healthcare access is largely observed across socioeconomic determinants. For example, the poor have lesser access to healthcare than the rich [1, 2]; men have better healthcare access than women [3, 4, 5]; and people from the upper caste are better off than the lower caste in healthcare access [6, 7]. Studies also confirm high inequality in healthcare access due to the intersection of two or more socioeconomic axes [8]. A large part of the population actually stands at the intersection of several socioeconomic attributes and hence, affiliation with a number of low hierarchical socioeconomic attributes (such as low income, women, low caste, and poor education) actually decides how much a person would be disadvantageous than others in healthcare access. For example, an illiterate black woman from the poor income class would have lower healthcare access than a literate white woman from the same income class. There are other examples too.
Socioeconomic attributes may be either positive or negative. Positive attributes are like men, the rich class, higher education, upper caste and others. Negative attributes are such as women, the poor, illiterate, and lower caste. Second, an individual usually has a large number of positive and negative attributes, but the number of people with only negative attributes is found to be only a fraction of the population such as illiterate, old, poor women from low caste and race. Third, the positive and negative socioeconomic attributes cancel the effect of each other on healthcare access and it is the net effect (either positive or negative) that actually drives access to healthcare. For example, a literate woman from a poor income class would have better healthcare access than a literate woman from the same income class. It is because ‘literacy’ diminishes the negative effect of attributes such as ‘being a woman’ and ‘poor income class’ and thus, improves healthcare access. Similarly, an old- rich man from a low caste may have better healthcare access than an old man from a poor income class. The attribute of ‘richness’ suppresses the negative impact of attributes like ‘old age’ and ‘low caste’.
Among all socioeconomic attributes, rich and poor income classes are perhaps the most decisive and dominant attributes of healthcare access. Despite the majority of negative socioeconomic attributes, if a person is rich, he would have better healthcare access than others; therefore, the higher income is considered the most dominant factor for healthcare access. Perhaps that is why financial protection schemes such as health insurance are considered the most effective way of equal distribution of health resources. Most government policies on health are structured around financial support. In India, government-sponsored health insurance schemes such as ‘RSBY’ and ‘Ayushman Bharat’ are acclaimed as the best way to improve healthcare access [9]. Public and private organisations also run similar schemes. Other countries have also recognised income as a major determinant of better healthcare access and health status and therefore, they promoted the idea of universal healthcare either by providing the universal basic income (UBI), health insurance, or improving the health infrastructure to reduce the income barrier. For the rich, income/health expenditure is not a barrier, but there are other supply-side barriers to healthcare access such as poor health infrastructure, the distance of healthcare facilities from home, waiting time, and others. However, even those supply-side barriers are not absolute for the rich and they can still have healthcare access as they are capable of buying. Does this mean, the rich (more precisely, super rich) have always access to healthcare? The answer is perhaps no. The reason is discussed later.
Education is another dominant attribute of healthcare access. An educated person from a lower social hierarchy may have better healthcare access than those who are from a higher social hierarchy but are not educated. Rest other socioeconomic attributes are weak and by improving the income and education of a person, his healthcare access can be significantly improved. However, income and education resolve only the supply-side barriers and one can still have poor healthcare access due to demand-side barriers. For example, a rich and educated woman may not find the time to visit a healthcare centre due to being busy with household work. Similarly, a rich and educated old man is unable to access healthcare services due to the unavailability of any companion to take him to a doctor or hospital. Cognitive barriers like ignorance of illness and poor perception of the disease/illness also prevent people of any social hierarchy from healthcare access despite the availability of all kinds of health facilities nearby.
In this paper, some of the fundamentally strong socioeconomic attributes are explored regarding healthcare access. Since, even at the top of the socioeconomic hierarchical level, the cases are non-access to healthcare are significantly found, it is important to explore those factors to address the barrier to healthcare access in a more comprehensive and holistic way.
Dependency on Others: Pivot to Healthcare Access
The role of socioeconomic attributes in healthcare access has widely been studied. However, in all those studies, the dependency of individuals on others to access healthcare has largely been ignored. There might be a situation when an individual is at the top of the social hierarchy, but can’t access to healthcare because of his high dependence on others. For example, an old age person is rich, well-educated, and belongs to the upper caste group but still, he is unable to access healthcare because he is dependent on his family members to take him to a doctor or medical facilities. Similarly, a disabled person may face the same kind of situation for healthcare access. In almost all developed and developing societies, women have primary responsibility for their children, family members and household work. They also have lesser autonomy than men in the decision-making process. A large number of studies have confirmed the poor healthcare access and health status of women due to their poor autonomy and high involvement in household work (see, for example, [10, 11]). In a few Asian and Middle-east countries such as India, Bangladesh, Pakistan, Afghanistan, Saudi Arabia, Qatar and others, the situation is even worsening. Therefore, women are partially dependent upon men and other family members to access healthcare. At last, children below the age of 14 years are assumed to be fully dependent on family members for healthcare access.
Basically, attributes such as ‘age’, ‘gender’ and ‘disability’ are the most persistent and fundamental attributes that prevent healthcare access despite an individual’s high social status in terms of income, education, caste, ethnicity, and region. These three attributes can also interact with each other. An example of such interaction is given in Figure 1.
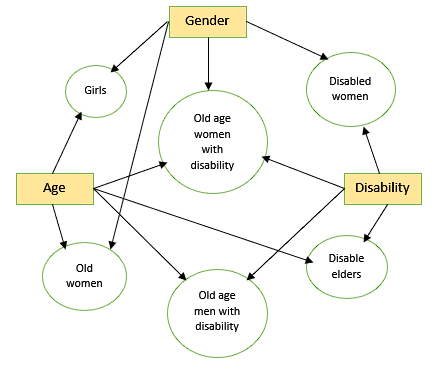
Figure 1: Interaction of attributes: Age, Gender, and Disability. With these three attributes, there are four kinds of individuals who are either partially or fully dependent on others irrespective of their status on the ladder of social hierarchy. They are (i) old-age men, (ii) women, (iii) disabled men, and (iv) children. The suggested individuals represent the threshold level of maximum positive socioeconomic attributes at which the dependency factor dominates all for healthcare access. If we alter the interaction of attributes – ‘age’, ‘gender’, and ‘disability’, the dependency on others would increase. For example, elder women would be more dependent on others than elder men for healthcare access. Similarly, old-age disabled women would be more dependent on others than disabled men. Dependency on others is one of the major barriers to healthcare access. Despite any socioeconomic improvement and supply-side healthcare development, few individuals would always be left with inadequate healthcare access and thus, the vision of ‘healthcare for all’ can never be achieved.
A Suggested Framework for Healthcare Access
To address the divergence in healthcare access at the intersection of three socioeconomic attributes – ‘age’, ‘gender’, and ‘disability’, a common framework with possible corrective measures can be adopted. It is given in Figure 2 below.
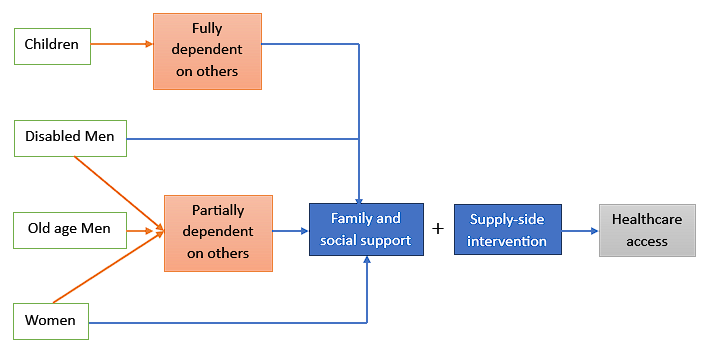
For four basic kinds of individuals- children, disabled men, old age men, and women, two corrective measures are suggested- (i) Family support, and (ii) Supply-side intervention. A single or combination of these measures can effectively improve healthcare access irrespective of their social status.
Children below the age of 14 years are unable to take care of their health and therefore, they are fully dependent on others for quality healthcare. Therefore, good family support, love, and affection may significantly improve their healthcare access and health status. In almost all societies, the health of children is a top priority of the family and irrespective of household income, region, caste, religion, or educational status, the family does best of its effort to consult with doctors and medical practitioners for the good health of children. In some cases, children are left of healthcare access because of institutional and non-institutional barriers, although few barriers are also successfully overcome because of the family’s emotional attachment to children. For example, the income barrier is often addressed by taking financial support from relatives/friends, NGOs, and by selling assets. Non-availability of quality healthcare nearby is also addressed by travelling long distances irrespective of the cost and time involved. Hence, every family puts their best effort into accessing healthcare for children. The outcome of such efforts might be good, satisfactory or unsatisfactory, but full family support is largely observed and it is the most decisive factor in healthcare access.
Disabled men also need family support for healthcare access. Here, family support is usually needed in the form of either nursing care or support at home or a companion to go along with the disabled to healthcare facilities. The other barriers such as low income and poor education may also come across healthcare access, but they can effectively be reduced by the families, if they wish. Therefore, the most pertinent and common requirement of manpower support for the disabled can effectively be met through family support.
For old age people, the ‘availability of quality healthcare nearby’ and ‘family support’ are two basic requirements for healthcare access. In old age, people usually turn to be physically weak and emotionally vulnerable and thus, they need family support to address motor control and cognitive impairments. Further, despite family support, elders might not be able to travel a long distance to seek healthcare due to their poor mobility and hence, quality healthcare nearby is equally important for them for better healthcare access.
Women are perhaps in the most disadvantageous position to healthcare access. A long history of women’s subjugation and exploitation is perhaps a major reason for their low position in family and society and therefore, women need more social and emotional support for the equitable allocation of resources including healthcare. They usually need family support for greater autonomy in the decision-making process on several issues including health. In countries like India, Pakistan, Bangladesh, and other Islamic countries, women are either restricted to go alone anywhere or prefer to go along with some family member. Thus, family support in terms of both physical and emotional support is necessary for better healthcare access. In addition, the high involvement of women in household work is common to observe in all families which not only restricts their self-care but also increases the trade-off between health priority and other household responsibilities. Hence, sharing household work with other family members would significantly improve their chances of healthcare services. The ‘availability of healthcare centres nearby’ is another major determinant of their healthcare access, especially for those women who live in a few Asian and Islamic countries. If quality healthcare is available near their home, it would serve two purposes. First, near-home healthcare facilities would reduce the requirement of a companion to go along with them and second, it would reduce the opportunity cost of forgoing the household chores for consulting a doctor.
Social Support and Healthcare Access
Social support is characterised by the help and assistance from friends, family members, neighbours and other people from society. Pierce GR, et al. [12] defines social support as assistance provided to individuals to cope with difficulties in everyday life, especially, from the critical situation. Hall A, et al. [13] explains the importance of social exchange in situations of need to improve health outcomes. Social support not only reduces the risk of physical illness but also helps the seeker to speedy recovery from the mental illness [14, 15]. Usually, social support is considered tangible health [16], although it may also be in the form of perceived support which is usually subjective in nature and proves to be very helpful in the situation of mental stress [17].
Social supports depend upon socioeconomic, demographic and geographical factors. Persons with higher socioeconomic status along with younger and married men usually receive higher social support than others [18]. Children and younger get more family support because of the natural love and affection they get from family members, although cases of neglected children are also largely observed among families of low socioeconomic status [19, 20, 21]. Social networking significantly supports the healthcare demand of men [22, 23]. However, in the case of disabled men, the need for social support becomes more urgent. A disabled man not only faces the problem due to physical and mental disability but also due to the lacklustre attitude of society [24]. Thus, Social support would help them cope with difficulties and lead a respectable life [25].
Social support is particularly important to women due to their specific roles in the family and society [26]. Women care for their family members with heart and soul without giving due attention to their healthcare needs [27]. The discriminatory and exploitative nature of men in a patriarchal society leaves women more vulnerable to physical and mental stress. The low socioeconomic status of women further aggravates the problem. Hence, women are usually the second recipient of all public facilities and support including healthcare [28, 29]. The poor utilization of healthcare and ignorance of illness leads to several health- related complexities among women including premature deaths [30]. Therefore, women need greater attention for their better health and well-being and here, family and social support for women can prove to be decisive. Women are found to be the recipients of informal perceived support [31], but still, a lot is required to do at both institutional and societal levels.
Elders are also more vulnerable to illness and disease [32]. In older age, many health issues arise along with poor mobility and high cognitive impairments and therefore, social supports become more critical and amplified [33]. At very old age, social networking and support also get reduced and social isolation becomes deeper among elders from low socioeconomic status [34]. Therefore, the lack of social support significantly contributes to the high mortality among elders [35]. Several studies have confirmed a positive association between social support and the good health status of elders. The emotional support of family members including spouses and children immensely supports the health and well-being of elders [36].
Supply-Side Intervention
The supply-side intervention includes adequate health infrastructure along with financial protection schemes such as health insurance, contractual indemnities, universal basic income, and others. Quality of healthcare is nonetheless the most important factor for access to healthcare, although in the case of disabled men, the elderly, and women, the ‘availability of healthcare services nearby’ is equally important. It is due to the reason that all these three kinds of individuals have specific barriers to either physical mobility or social mobility. The restricted physical mobility of disabled men and the elderly are well understood, but women are primarily restricted to social mobility. In addition, women are burdened with household work and therefore, there opportunity cost of consulting a doctor is comparatively high. In India, around 8.9% of women didn’t access healthcare either due to either ‘non-availability of medical facility nearby’ or ‘non-affordability of long waiting time due to domestic engagement’ (NSS 75th round survey, 2017- 18). It is the second most prominent reason for non-access to healthcare after the reason of ‘non-seriousness of illness.’ Therefore, appropriate distribution of quality healthcare services must be ensured in clusters of population.
Conclusion
Socioeconomic attributes play a significant role in healthcare access and perhaps due to the same reason, the government’s health policy and programs are specifically designed to address the socioeconomic barriers for healthcare seekers. For example, the universal health insurance program is a novel step of eliminate the financial barrier for the poor. In India, the ‘Indira Gandhi National Disability Pension Scheme’ supports the poor-disabled and the ‘Maternal Health Scheme’ supports women. However, at the top of the socioeconomic hierarchical level, the cases of non-access to healthcare are also significantly found because of either cognitive barriers like ‘non-seriousness of illnesses’ or ‘dependency on others.’ The barrier of dependency can be effectively reduced by family and social support. Making people sensitised and aware of their family and social obligation is a difficult task because of its underpinning to socio-cultural and psychological setups. Therefore, a multi- facet approach including sociological and behavioural approaches is needed to achieve equitable healthcare access for all.
References
-
Xu Ke, Saksena P, Carrin G, Jowett M, Kutzin J (2009) WHO report.
-
Asada Y, Kephart G (2007) Equity in Health Services use and Intensity of use in Canada. BMC Health Serv Res 7(41): 1-12.
-
Markids CP (1992) Women and Access to Healthcare. Social Science and Medicine 35(4): 619-626.
-
Davidson PM, McGrath SJ, Meleis AI, Stern P, Digiacomo M, et al. (2011) The Health of Women and Girls Determines the Health and Well-Being of our Modern World: A White Paper from the International Council on Women’s Health Issues. Health Care Women Int 32(10): 870-886.
-
Dasgupta A (2020) Indian Women may be Missing Tertiary Healthcare.
-
Agarwal G, Arokiasamy P (2010) Morbidity Prevalence and Healthcare utilization among older Adults in India. Journal of Applied Gerontology 29(2): 155-179.
-
Patel P, Das M, Das U (2018) The Perceptions, Health Seeking Behaviors and Access of Schedule Caste Women to Maternal Health Services in Bihar, India. Reprod Health Matters 26(54): 114-125.
-
Sen G, Iyer A, Mukherjee C (2009) A Methodology to Analyse the Intersections of Social Inequalities in Health. Journal of Human Development and Capabilities 10(3): 397-415.
-
Mahapatro SR, James KS, Mishra US (2021) Intersection of Class, Caste, Gender and unmet Healthcare needs in India: Implications for Health Policy. Health Policy Open 2: 100040.
-
Anand I, Thampi A (2021) The Crisis of Extreme Inequality in India. Indian J Labour Econ 64(3): 663-683.
-
Stamarski CS, Hing LSS (2015) Gender Inequalities in the Workplace: the Effects of Organizational Structures, Processes, Practices, and Decision makers’ Sexism. Front Psychol 6: 1400.
-
Pierce GR, Sarason BR, Sarason IG (1990) Integrating Social Support Perspectives: Working Models, Personal Relationships and Situational Factors. In: Duck S (Eds.), Personal Relationships and Social Support. Sage Publications, London, pp: 173-215.
-
Hall A, Wellman B (1985) Social Networks and Social Support. In: Cohen S, et al. (Eds.), Social Support and Health. Academic Press pp: 23-41.
-
Seeman TE (2000) Health Promoting Effects of Friends and Family on Health Outcomes in Older Adults. Am J Health Promot 14(6): 362-370.
-
Stroebe W (2000) Moderators of the Stress-Health Relationship. In: Stroebe W (Eds.), Social Psychology and Health. Open University Press, Philadelphia, pp: 236-273.
-
Krause N (2001) Social Support. In: Binstok RH & George LK (Eds.), Handbook of Aging and the Social Sciences. Academic Press, San Diego, pp: 272-294.
-
Gadalla TM (2010) The Role of Mastery and Social Support in the Association Between Life Stressors and Psychological Distress in Older Canadians. J Gerontol Soc Work 53(6): 512-530.
-
Gallie D, Paugam S (2000) Welfare Regimes and the Experience of Unemployment in Europe. Oxford University Press.
-
Boer KD, Rothwell DW, Lee C (2013) Child and Family Poverty in Canada: Implications for Child Welfare Research. Canadian Child Welfare Research Portal Information Sheet pp: 1-123.
-
Knitzer J, Perry DF (2009) Poverty and Infant and Toddler Development: Facing the Complex Challenges. In: Zeanah C (Eds.), Handbook of Infant Mental Health. Guilford Press, USA, pp: 135-152.
-
Lefmann T, Combs OT (2014) Prenatal Stress, Poverty, and Child Outcomes. Child and Adolescent Social Work Journal 31(6): 577-590.
-
Antonucci TC, Akiyama H (1987) An Examination of Sex Differences in Social Support among Older Men and Women. Sex Roles 17: 737-749.
-
Thoits P (1995) Stress, Coping, and Social Support Processes: Where are we? What next? Journal of Health & Social Behavior 35: 53-79.
-
Akbarian MS (2007) Disability with Approach of Social Welfare. J Student Mohaghegh 1(2): 47-55.
-
Obst P, Stafurik J (2010) Online we are all able Bodied: Online Psychological Sense of Community and Social Support Found through Membership of Disability- Specific Websites Promotes well-being for People Living with a Physical Disability. Journal of Community & Applied Social Psychology 20(6): 525-531.
-
Hurdle DE (2001) Social Support: A Critical Factor in Women’s Health and Health Promotion. Health Soc Work 26(2): 72-79.
-
Arman M, Gebhardt A, Nordberg JH, Andermo S (2020) Women’s Lived Experiences of Chronic Pain: Faces of Gendered Suffering. Qual Health Res 30(5): 772-782.
-
Bagchi T, Das A, Dawad S, Dalal K (2022) Non-Utilization of Public Healthcare Facilities during Sickness: A National Study in India. Journal of Public Health 30(4): 943-951.
-
Wisdom JP, McGee MG, Horner JW, Michael YL, Adams E, et al. (2010) Health Disparities between Women with and without Disabilities: A Review of the Research. Soc Work Public Health 25(3): 368-386.
-
Filippi V, Ronsmans C, Campbell OMR, Graham WJ, Mills A, et al. (2006) Maternal Health in Poor Countries: the Broader Context and a Call for Action. Lancet 368(9546): 1535-1541.
-
Ross CE, Mirowsky J (1989) Explaining the Social Patterns of Depression: Control and Problem Solving or Support and Talking? J Health Soc Behav 30(2): 206-219.
-
Rundall TG (1992) Health Services for an Aging Society. Med Care Res Rev 49: 3-18.
-
Litwin H, Landau R (2000) Social Network Type and Social Support among the Old-Old. Journal of Aging Studies 14(2): 213-228.
-
Weyers S, Dragano N, Mobus S, Beck EM, Stang A, et al. (2008) Low Socio-Economic Position is Associated with Poor Social Networks and Social Support: Results from the Heinz Nixdorf Recall Study. Int J Equity Health 7: 13-
-
Andrew MK, Mitnitski AB, Rockwood K (2008) Social Vulnerability, Frailty and Mortality in Elderly People. PLoS ONE 3(5): e2232.
-
Okabayashi H, Liang J, Krause N, Akiyama H, Sugisawa H (2004) Mental Health among Older Adults in Japan: Do Sources of Social Support and Negative Interaction make a Difference? Soc Sci Med 59(11): 2259-2270.
- Origin, Evolution, and Functional Impact of Short Insertion- Deletion Variants in Human Genomes: A Review
- Harnessing Molecular Glues for Next-Generation Vaccine, Cancer and Cardiovascular Disease Drug Development: A Comprehensive Review
- Lateral Cervical Epidermal Inclusion Cyst in a Paediatric Patient: A Rare Case Report
- Malarial Plasmodium Falciparum with Hepatitis B and C Virus Infections among Blood Donors in Ife Central Local Government Area, Ile Ife, Osun State, Nigeria
- Withanolides and Withaferin A- What’s next in Ashwagandha Research
- Designing of Dual Pulse Photoacoustic Tomography for Imaging of Drug-Response and Tumor Growth