Pseudoxanthoma Elasticum and its Rare Co-Existence with Comedones and Neurofibroma
<p>A 68 year old male patient, presented with multiple asymptomatic elevated skin lesions over the face, V area of neck since last 40 years. Physical examination revealed numerous open comedones all over the face, forehead and V area of neck. Numerous firm, skin colored to yellowish, non-follicular papules coalescing into plaques were seen around the neck, suprascapular region, both axillae, cubital and popliteal region with redundant lax skin folds. A single pedunculated nontender firm swelling of 1X1 cm size is seen over the left side of the chest. Histopathological examination of punch biopsy from lesional skin showed irregularly clumped faintly basophilic elastic fibres admixed with mucoid material in the mid and lower dermis. Excisional biopsy from the lesion over the chest showed skin with underlying dermal circumscribed, non encapsulated tumour composed of spindle cells arranged in fascicles. Patient improved with topical and systemic retinoids. We are reporting this case as it’s a rare association with pseudoxanthoma elasticum.</p>
Introduction
Pseudoxanthoma elasticum (PXE) is an inherited disorder of the connective tissue mainly involving the elastic fibers of the skin, eyes and cardiovascular system [1]. Skin lesions consist of yellowish papules or plaques with an associated increase in skin laxity. Histopathology of skin lesion shows calcification, alteration and fragmentation of elastic fibres in the mid and lower dermis. The diagnosis is most often made late in the second or third decade of life [1, 2]. With a prevalence of 1 in 25,000 to 70,000, it results from mutations in a gene located at chromosome 16p13.1, which encodes for the transmembrane transporter protein adenosine triphosphate binding cassette C6 (ABC- C6) with an autosomal recessive inheritance pattern [2]. We hereby report an unusual case of Pseudoxathoma elasticum and its co-existence with cutaneous neurofibroma and numerous open comedones which is an extremely rare association.
A 68 year old male patient, presented with multiple asymptomatic elevated skin lesions over the face, V area of neck since last 40 years. There was no history of similar complaints in the family nor was there any consanguinous marriage. The patient was not on any drugs.
Physical examination revealed numerous open comedones all over the face, forehead and V area of neck, with relative sparing of forehead and nose (Figure 1). Numerous firm, skin colored to yellowish, non-follicular papules coalescing into plaques were seen around the neck, suprascapular region, both axillae, cubital and popliteal region (Figures 4-7). These areas also showed lax, redundant, sagging folds of skin mainly around the neck (Figures 1-3). A single pedunculated nontender firm swelling of 1X1 cm size is seen over the left side of the chest at the level of left coastal margin along the mid clavicular line (Figure 8). The ophthalmologic examination was normal. The results of routine laboratory tests were within normal limits. Electrocardiography (ECG) and radiography of the chest, both were within normal limits.







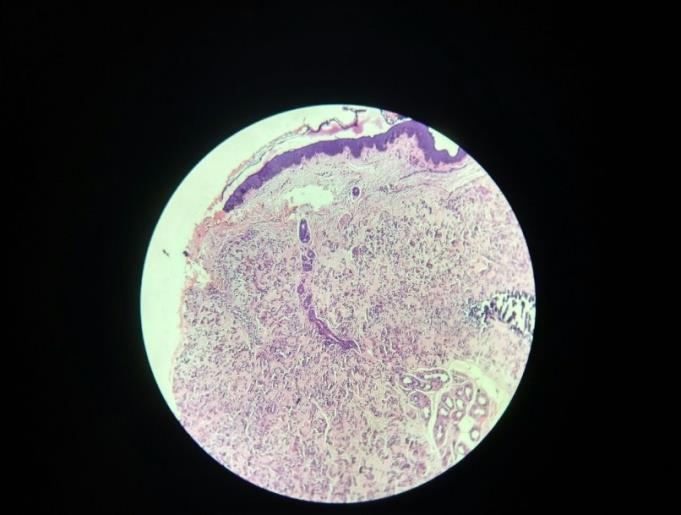
Figure 7: Skin colored smooth pedunculated swelling of 1X1 cm size over left chest. Skin from neck and left forearm was biopsied and subjected to staining with hematoxyllin - eosin and Von Kossa stains. It showed irregularly clumped faintly basophilic elastic fibres admixed with mucoid material in the mid and lower dermis (Figure 8). At one focus, basophilic dense calcified deposits were seen. No evidence of inflammatory cell infiltration. Hematoxylin and eosin stained section from the excisional biopsy specimen of swelling over left chest showed skin with underlying dermal circumscribed, nonencapsulated tumour composed of spindle cells arranged in fascicles. Spindle cells showed thin wavy
Discussion
Pseudoxanthoma elasticum can be associated with considerable morbidity and mortality. The clinical variability is evident by observations that the involvement of all three major organ systems, i.e., skin, eyes and the cardiovascular system, is encountered in some patients. Flexures and periumbilical skin are commonly affected. Ocular involvement is characterised by angioid streaks, breaks in the Bruch’s membrane, choriocapillaris etc. Lastly, patients may develop systemic manifestaions like increased risks of acclerated peripheral vascular disease, ischemic heart disease, hypertension and cerebrovascular disease [3, 4].
![Figure 9: Resolution of comedones following treatment. In the present case the lesions over the neck, limbs, suprascapular, supraclavicular, popliteal and cubital area were clinically suggestive of pseudoxanthoma elasticum which was consistent with histopathological findings. Pseudoxanthoma elasticum and its association with reticulate papules and plaques as seen in our case along with multiple open comedones and neurofibroma is an extremely rare association. A study of Pseudoxanthoma elasticum cases in the Indian subcontinent showed that skin lesions and eye involvement are common but systemic involvement is relatively rare [5]. Eye](/fulltextimages/2122/fig_9.jpeg)
Figure 9: Resolution of comedones following treatment. In the present case the lesions over the neck, limbs, suprascapular, supraclavicular, popliteal and cubital area were clinically suggestive of pseudoxanthoma elasticum which was consistent with histopathological findings. Pseudoxanthoma elasticum and its association with reticulate papules and plaques as seen in our case along with multiple open comedones and neurofibroma is an extremely rare association. A study of Pseudoxanthoma elasticum cases in the Indian subcontinent showed that skin lesions and eye involvement are common but systemic involvement is relatively rare [5]. Eye
6. Hartman A, Hartman-Visser SR (1977) Pseudoxanthoma elasticum with extensive comedone formation. Dermatologica 154(5): 318-319.
involvement and systemic symptoms were not seen in our case. There is no specific treatment for Pseudoxanthoma elasticum. This patient was treated with topical tretinoin 0.025%, systemic isotretinoin 10mg per day and sunscreen. After 8 weeks of therapy his lesions started showing improvement with resolution of most of comedones (Figure 9). Cutaneous neurofibroma was excised under local anaesthesia.
Conclusion
We are reporting this case as the association of Pseudoxanthoma Elasticum with comedones and cutaneous neurofibroma is an extremely rare. As per extensive literature search there was one case report which showed an association of PXE with multiple comedones [6].
References
-
Kumar GN, Ragi KV, Nair PS (2007) Pseudoxanthoma elasticum with cerebrovascular accident. Indian J Dermatol Venereol Leprol 73(3): 191-193.
-
Baglieri F, Scuderi G (2010) Pseudoxanthoma elasticum: Description of a late onset case. Indian J Dermatol Venereol Leprol 76(4): 448.
-
Kocatürk E, Kavala M, Zindanci I, Koç M (2009) Periumbilical perforating pseudoxanthoma elasticum. Indian J Dermatol Venereol Leprol 75(3): 329.
-
Rath N, Bhardwaj A, Kar HK, Sharma PK, Bharadwaj M, et al. (2005) Penicillamine induced pseudoxanthoma elasticum with elastosis perforans serpiginosa: A case report. Indian J Dermatol Venereol Leprol 71(3): 182-185.
-
Leblebici C, Falay T, Zırtıloğlu S, Demirkesen C (2017) Cutis laxa-like pseudoxanthoma elasticum with osteoma cutis. Indian J Dermatol Venereol Leprol 83(4): 464-467.
- Epithelioid Granuloma; 3cases with Different Clinical Features
- Advancing Representation in Dermatology Clinical Trials: Ethical, Scientific, and Regulatory Imperatives for Inclusion Across all Fitzpatrick Skin Types
- A Case of Atopic Dermatitis with Concurrent Psoriasis Vulgaris: Successful Treatment with Upadacitinib
- Innovation Lifting Eyeshadow: A Synthesis of Makeup and Optical Illusion
- Distinguishing Superficial Actinic Porokeratosis from Actinic Keratosis with UVF Dermoscopy: A Case Report
- High Mobility Group Box 1 (HMGB1) in Cutaneous Inflammation: An Immune Modulator Bridging Cellular Stress, Ferroptosis and Danger Signaling