Epithelioid Granuloma; 3cases with Different Clinical Features
Author presents three cases of epithelioid cell granuloma with different pathogenic backgrounds. Two cases were noninfectious and were diagnosed as lupus miliaris disseminatus faciei (LMDF) and sarcoidosis, respectively. The remaining case was infectious and diagnosed as borderline tuberculoid (BT) leprosy. In the histopathology of LMDF, granulomas were observed to be continuous with facial hair follicles. Although various etiologies have been proposed for sarcoidosis, the involvement of Propionibacterium acnes (P. acnes) has been reported. Hair follicles are preferential site for P. acnes colonization. LMDF has been considered to represent a variant of sarcoidosis. The finding that granulomas in LMDF were localized to hair follicles in the present case suggests a possible association between LMDF and sarcoidosis. The histopathological features of BT leprosy showed more intense inflammatory changes than those observed in the two non-infectious granulomatous diseases, reflecting a strong host immune response against Mycobacterium leprae. The histopathological features of these 3 epithelioid cell granulomas with different pathogenic backgrounds are intriguing, as they appear to reflect the individual immune environments responding to different etiologic factors.
Abbreviations
LMDF: Lupus Miliaris Disseminatus Faciei; BT: Borderline Tuberculoid; WHO: World Health Organization.
Introduction
Epithelioid granuloma is an inflammatory reaction against insoluble pathogens. The key cells of granuloma are monocytes/macrophages, originate from hematopoietic stem cells in the bone mallow. They transform to histiocytes, epithelioid cells, and epithelial giant cells, which store the phagocytosed residual materials (pathogens). The proliferated epithelioid cells enclosing the core pathogens and tightly aggregate to form epithelioid granuloma, accompanied with various inflammatory cells. Here, 2 cases of non-infectious granuloma and one case of infectious granuloma are presented, focusing on the pathological findings.
Case Studies
Case 1: Lupus Miliaris Disseminatus Faciei (LMDF)
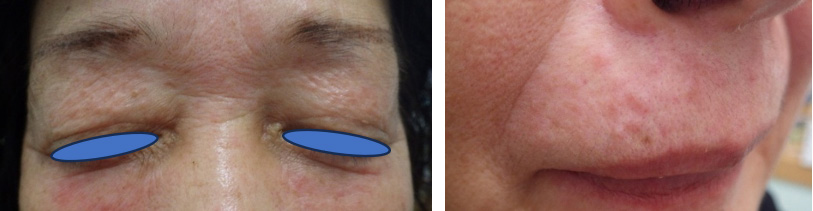
A 66-year-old Japanese woman noticed indolent papular eruptions symmetrically spread on her face 2 weeks prior to presentation. Each lesion was 2 to 4 mm in diameter, and most lesions were located around eyes and perioral (Figure 1).
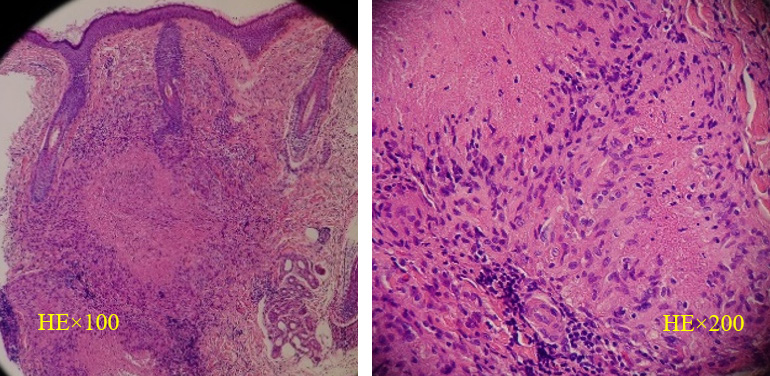
Pathology Eosinophilic amorphous substances containing nuclear dust are surrounded by epithelioid cells, mononuclear lymphocytes, and multinucleated giant cells (Figure 2). These findings are compatible with those of epithelioid granuloma with caseous necrosis. Most of these are connected with hair follicles. The patient was diagnosed with LMDF.
Case 2: Sarcoidosis
A 73-year-old Japanese woman noticed several intradermal nodules on the lateral part of both upper arms. Each nodule was less than 10 mm in diameter and well circumscribed. One nodule was excised for pathological examination.
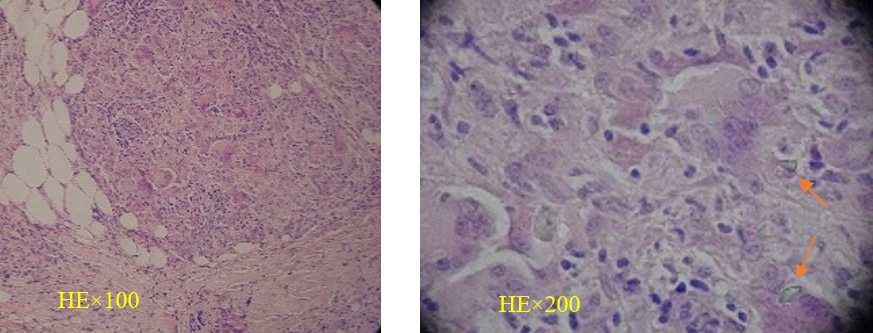
Pathology Globular masses of various sizes are found in the subcutaneous tissue, composed of epithelial cells and lymphocytes at the periphery, forming epithelioid granulomas. Multinucleated giant cells are also found, some of which contained shiny foreign substances, resembling silica (Figure 3). There is no caseation inside the granuloma. These findings are compatible with intradermal sarcoidosis.
Based on the pathological findings, some physical examination was conducted. There were no abnormal findings on chest radiology, electric cardiograph, and ophthalmological examination. Angiotensin converting enzyme level was normal.
Case 3: Leprosy (Borderline Tuberculoid: BT)
A 31-year-old Brazilian man visited our clinic with numerous well-defined red plaques that measured 1-4 cm in diameter and another larger annular lesions (Figure 4). These were asymmetrically disseminated on the face, trunk, and extremities. Loss of sensation, rough skin texture, and hair loss were apparent inside these lesions. Biopsy specimen was obtained from a red macule on his left forearm.

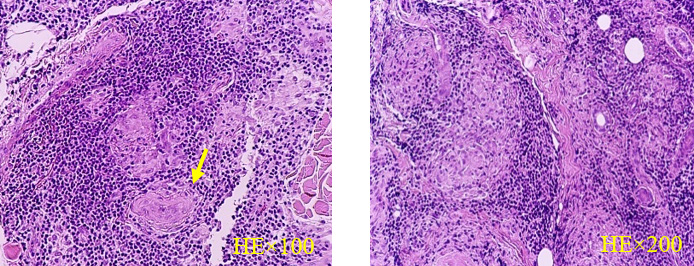
Pathology Degenerated nerve bundles, skin appendages, and clumped epithelioid cells are surrounded by densely infiltrated lymphocytes, forming well defined epithelioid cell granulomas (Figure 5). Acid fast bacilli are not found on Fite stain. BT leprosy was diagnosed and the patient completely cured with WHO-MDT/MB [1] regimen for 1 year.
Discussion
In Case 1, epithelioid cell granulomas were observed predominantly around hair follicles. Although the pathogenesis of lupus miliaris disseminatus faciei (LMDF) remains unclear, it has been suggested that some cases represent a micropapular variant of sarcoidosis or a sarcoidal form of rosacea [2].
Previous studies have also suggested an etiologic link between Propionibacterium acnes (P. acnes, currently classified as Cutibacterium acnes) and sarcoidosis [3]. Given that sebaceous glands within hair follicles represent a preferential site for P. acnes colonization, the folliculocentric distribution of granulomas in this case may provide supportive evidence for an immunopathological association between LMDF and sarcoidosis. This observation reinforces the hypothesis that a localized immune response to follicular antigens may contribute to granuloma formation in selected cases.
The histopathological findings in Case 2 are consistent with a sarcoid-type granulomatous reaction induced by silica, a traumatic foreign material. Sarcoidosis is thought to arise from an exaggerated cell-mediated immune response to a wide range of antigens, including microorganisms, environmental agents, and autoantigens [4]. In this case, the granulomatous response appears to have been triggered by an exogenous inorganic material, highlighting the heterogeneous antigenic stimuli capable of inducing sarcoid- type granulomas. Although no extracutaneous involvement has been identified to date, careful long-term follow-up is warranted, given the potential for systemic manifestations to emerge over time.
In contrast, Case 3 represents an infectious granuloma of borderline tuberculoid (BT) leprosy. Histologically, the lymphocytic infiltrate was more prominent than that observed in the non-infectious granulomas of Cases 1 and 2. BT leprosy is characterized by strong cell-mediated immunity against Mycobacterium leprae, and the histopathological findings in this case reflect a robust host immune response aimed at pathogen elimination [5]. This contrasts with sarcoid-type granulomas, in which the inciting antigen may be poorly defined or persist intracellularly without effective clearance.
Taken together, these 3 cases illustrate that epithelioid cell granulomas represent a pathological phenotype reflecting the functional status of cell-mediated immunity in the host. Variations in histological architecture and inflammatory composition among the cases suggest differences in individual immune environments and underlying different etiologies.
Conflict of Interest
The author declares no conflicts of interest.
References
-
(2018) WHO guidelines for the diagnosis, treatment and prevention of leprosy. World Health Organization.
-
El Darouti M, Zaher H (1993) Lupus miliaris disseminatus faciei: pathologic study of early, fully developed, and late lesions. Int J Dermatol 32: 508-511.
-
Eishi Y (2013) Etiologic link between sarcoidosis and Propionibacterium acnes. Respir Investig 51: 56-68.
-
Asai J (2017) What is new in the histogenesis of granulomatous skin diseases? J Dermatol 44: 297-303.
-
Ridley DS, Jopling WH (1966) Classification of leprosy according to immunity. Int J Lepr 34(3): 255-273.
- Advancing Representation in Dermatology Clinical Trials: Ethical, Scientific, and Regulatory Imperatives for Inclusion Across all Fitzpatrick Skin Types
- A Case of Atopic Dermatitis with Concurrent Psoriasis Vulgaris: Successful Treatment with Upadacitinib
- Innovation Lifting Eyeshadow: A Synthesis of Makeup and Optical Illusion
- Distinguishing Superficial Actinic Porokeratosis from Actinic Keratosis with UVF Dermoscopy: A Case Report
- High Mobility Group Box 1 (HMGB1) in Cutaneous Inflammation: An Immune Modulator Bridging Cellular Stress, Ferroptosis and Danger Signaling
- Knowledge, Attitude, and Practices towards Leprosy among Nurses around Semarang, Indonesia