Distinguishing Superficial Actinic Porokeratosis from Actinic Keratosis with UVF Dermoscopy: A Case Report
UVF dermoscopy (UVFD) is a new visualization method that is increasingly used for many different superficial dermatological conditions. In patients with widespread actinic changes in the face, actinic keratosis and solar lentigo may develop, and the risk of superficial actinic keratosis may also increase. We aimed to emphasize the use of UVF dermoscopy as a practical method for distinguishing superficial actinic porokeratosis from actinic keratosis as reporting this case.
Abbreviations
UVF: Ulster Volunteer Force; VFD: Variable Frequency Drive.
Case Report
A 65-year-old male patient was admitted to our clinic with itchy actinic keratosis on his face. He had no complaints of the skin other than the facial area. There was no history of skin cancer in either the patient or family.
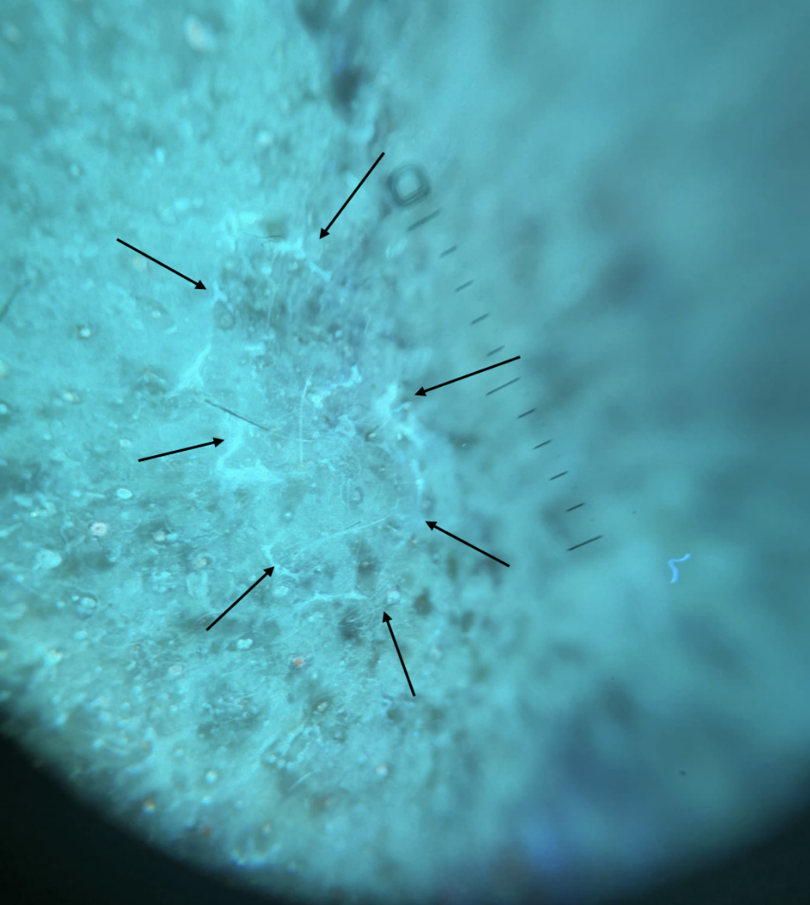
Dermatological examination revealed hyperkeratotic plaques with erythematous bases in frontal and nasal regions. Dermoscopy revealed a strawberry-like pattern. In addition, a 7 × 11 mm oval-shaped keratotic papule with a well-defined border and a slightly atrophic center on the nose was observed (Figure 1). UVF dermoscopy (DermLite DL5) revealed a white-blue peripheral keratotic tract with double free edges (Figure 2). No mucosal or nail findings were noted. Histopathology was not performed for the unusual lesion on the nose, because superficial actinic porokeratosis was considered based on the findings of this lesion on UVF dermoscopy, as previously described in the literature.
Cryotherapy was performed to diagnose the porokeratosis.

Discussion
Porokeratosis is a rare disorder characterized by anulary-atrophic plaques surrounded by well-defined ridge-like hyperkeratotic borders called cornoid lamellae. Delfino et al. defined dermoscopy of porokeratotic lesions as a whitish-yellowish, annular structure, appearing as ‘the outlines of a vulcanic crater as observed from a high point,’ sharply demarkating a central flat pink-white scar-like area [1].
Because UVFD does not penetrate deeper into the skin layers, it is a better way to distinguish features confined to the superficial layers of the skin [2]. The application of ultraviolet-induced fluorescence (UVF) dermoscopy in the diagnosis of dermatological disorders originating from the superficial layer of the epidermis has recently enabled the more successful visualization of UV-induced fluorescence findings that are not visible/weakly visible in conventional dermoscopy. UV dermoscopy has been used to diagnose porokeratosis, and dermoscopic findings have been used to diagnose this condition. Sarvesh et al. dermoscopy with UV light revealed a diamond necklace–like appearance at the edge of each of these lesions [3]
Zalaudek’s clinical-dermatoscopic classification of AK is associated with different stages of its progression, defined as grade one, two and three [4]. Actinic keratosis can sometimes be clinically confused with disseminated superficial actinic porokeratosis, especially grade one and grade two. UVF dermoscopy can be a useful tool for distinguishing superficial actinic keratosis from actinic keratosis.
Long-standing cases of porokeratosis may undergo malignant transformation, which has been reported in 6.9%–11.6% of cases [5]. Nevertheless, the reported risk of the malignant progression of AK varies widely. A systematic review found that the estimated risk of a single AK lesion becoming malignant ranged between 0.075% and 0.096% per year, or approximately 1% over 10 years, with some estimates as high as 10% over 10 years [6]. It has been stated that UVFD may increase the efficiency of examination in patients treated for field cancer owing to widespread actinic keratosis and may emerge as a useful tool in the follow-up of treatments [7].
Although there are studies in the literature on the use of UVFD in superficial actinic porokeratosis, comparative studies addressing both entities in the differentiation from actinic keratosis are limited. The absence of histopathological confirmation in our case is one of the conditions that limit the claim of the case; however, we believe that this case will allow studies to be conducted in which two conditions with different malignant potentials are addressed. Overall, UVF dermoscopy can help differentiate actinic keratosis from porokeratosis quickly in daily practice, thus revealing differences in malignancy development and improving or expanding the treatment options.
Conflict of Interest
The authors declare that they have no conflicts of interest.
Statement of Appropriate Institutional Board Approval and Informed Consent
Ethics approval was not applicable. The patient has provided informed consent to publication of their case details and images.
Acknowledgment
We would like to thank our patient for giving us permission for this case report.
References
-
Delfino M, Argenziano G, Nino M (2004) Dermoscopy for the diagnosis of porokeratosis. J Eur Acad Dermatol Venereol 18: 194-195.
-
Bhat YJ, Islam MS, Errichetti E (2024) Ultraviolet-Induced Fluorescence Dermoscopy, a Novel Diagnostic Technique in Dermatological Practice: A Systematic Review. Indian Dermatol Online J 16(1): 25-39.
-
Sarvesh ST, Vidya DK, Uday SK (2014) “Diamond necklace” appearance in superficial porokeratosis, Journal of the American Academy of Dermatology, pp: e125-e126.
-
Zalaudek I, Piana S, Moscarella E, Longo C, Zendri E, et al. (2013) Lallas A., Argenziano G. Morphologic grading and treatment of facial actinic keratosis. Clin Dermatol 32: 80-87.
-
Novice T, Nakamura M, Helfrich Y (2021) The malignancy potential of porokeratosis: A single-center retrospective study. Cureus 13: e13083.
-
Dodds A, Chia A, Shumack S (2014) Actinic keratosis: rationale and management. Dermatol Ther 4: 11-31.
-
Korecka K, Polanska A, Pazdrowska A, Dechent C (2024) Assessing field cancerization and actinic keratosis using ultraviolet-induced fluorescence dermatoscopy after the application of 5-aminolevulinic acid - An observational study. Photodiagnosis Photodyn Ther 46: 104056.
- Epithelioid Granuloma; 3cases with Different Clinical Features
- Advancing Representation in Dermatology Clinical Trials: Ethical, Scientific, and Regulatory Imperatives for Inclusion Across all Fitzpatrick Skin Types
- A Case of Atopic Dermatitis with Concurrent Psoriasis Vulgaris: Successful Treatment with Upadacitinib
- Innovation Lifting Eyeshadow: A Synthesis of Makeup and Optical Illusion
- High Mobility Group Box 1 (HMGB1) in Cutaneous Inflammation: An Immune Modulator Bridging Cellular Stress, Ferroptosis and Danger Signaling
- Knowledge, Attitude, and Practices towards Leprosy among Nurses around Semarang, Indonesia