Comparison between the Efficacy of Platelet Rich Plasma Combined with Fractional CO2 Laser vs. Laser alone in the Treatment of Facial Atrophic Acne Scar Split-Face Study
Introduction: Acne scar is a common distressing complication of acne vulgaris. Many treatments are available for treating post acne scars but optimized treatment still does not exist. Aim of the work: To compare the efficacy and safety of combining autologous PRP with FCL in the treatment of atrophic acne scars with that of FCL alone. Patients and Method: This study included 30 patients suffering from post-acne scars. CO2 laser treatment was applied to both sides of the face followed by PRP injection for the right side, each participant received 3 treatments with four weeks interval between the sessions and were followed up for a period of 3 months. Results: The outcome among the study were assessed using Goodman and Baron Scale at different time intervals. Significant reduction in acne scars was observed in both treated sides but better reduction of acne scars was noted at the PRP site, the incidence of adverse effects such as erythema during the procedure was significantly disappeared faster in PRP injected side compared to the other side. Conclusion: Combination of fractional CO2 laser resurfacing and intradermal PRP was superior to CO2 laser alone for acne scar treatment.
Hamid B Suleiman* and Rama M Okdeh
Introduction
Acne vulgaris is a common chronic inflammatory disorder of pilosebaceous unit affecting adolescents and young adults psychologically. Untreated acne especially the inflammatory type results in often distressing and difficult to treat scars. Acne scar formation results either due to increased tissue formation or damage of local tissue [1]. The severity of scarring depends upon the degree of tissue damage, inflammatory reaction and time lapsed from the onset of tissue inflammation [2, 3]. It can be classified into three different types: atrophic, hypertrophic, or keloidal. Atrophic scars are by far the most common type, which can also be classified based on the width, depth, and three- dimensional architecture into icepick, rolling, and boxcar scars [4].
Acne scarring cause cosmetic and psychological problems. There has been no standard treatment option for the treatment of acne scars. Various therapeutic options have been described, with variable clinical outcomes and complications, such as surgical techniques (punch graft, punch excision, subcision), resurfacing techniques (dermabrasion, ablative laser treatment, chemical peels), nonablative laser treatment, autologous fat transfer, and injection of dermal fillers [5]. Fractional ablative carbon dioxide (CO2) laser (FCL) therapy is based on the theory of fractional photothermolysis. Fractionated ablative laser treatment creates microscopic channels of thermal injury in the skin, causing skin tightening and smoothening through ablation and re-epithelialization and elevation of the floor of depressed scars through collagen remodelling [6]. Despite the documented efficacy of FCL in the treatment of acne scars, It has drawbacks, such as long periods of erythema and edema, which may cause discomfort and hinder patient’s daily lives, limiting its use [7].
Platelet-rich plasma (PRP) is an autologous concentration of human platelets in a small volume of plasma. It contains growth factors especially: epidermal growth factor, platelet- derived growth factor, transforming growth factor beta, and vascular endothelial growth factor [8]. These factors are known to regulate various processes including cell migration, attachment, proliferation, and differentiation, and to promote extracellular matrix production by binding to specific cell surface receptors [9]. PRP has been used in many fields of medicine and surgery to promote wound healing and accelerate the formation of newly formed tissue in addition to the cosmetic applications in the rejuvenation and treatment of hair disorders [10].
Aim of the Work To compare the efficacy and safety of combining autologous PRP with FCL in the treatment of atrophic acne scars with that of FCL alone.
Patients and Methods
This study was designed as a single-blinded, comparative split-face applying fractional CO2 laser alone for the left side and using a combination of CO2 laser with PRP for the treatment of acne scars on the right side. Thirty patients with facial acne scars presenting to Dermatology OPD of Tishreen Hospital, Lattakia, syria between 2018 -2019 were enrolled in the study. Clinical examinations of post-acne scars were performed with a magnifying lens, under good illumination, while the patient was sitting in an upright position, to detect the type of each lesion. Grading of post-acne scars’ severity was performed using the qualitative and quantitative scarring grading system by Goodman and Baron [11, 12].
Exclusion Criteria
Patients with active acne, predisposition to keloid formation, patients with active herpes infection, pregnant and lactating mothers, patients who have taken isotretinoin within previous 6 months, bleeding diathesis, HIV, HBV infection.
Treatment Protocol
All Patients received three sessions of laser treatment with four weeks interval between the sessions. Patients were followed up after 3 months of the final session. Laser treatment Each participant’s lesions on both sides of the face were treated with an ablative CO2 fractional laser (10600 nm) (Smartxide DOT, advanced CO2 fractional technology, Deka, Florence, Italy), and then only the right side received autologous PRP injection after each laser session Table 1.
| Parameters | Values |
|---|---|
| Power | 15 W |
| Dwell time | 600 μs |
| Spacing | 700 μm |
| Smart Stack | level 2 |
Table 1: Fractional CO2 laser settings.
Local anesthetic cream (5% lidocaine) was applied to the treated area, Then the whole face was cleansed using a mild cleanser.
Preparation of PRP
Under aseptic precautions, 10 ml of patient’s blood sample was collected from antecubital vein in a vacutainer containing anticoagulant sodium citrate in 1:9 ratio. Collected blood was subjected to centrifugation using SCILOGEX. spin was done at the speed of 4000 revolutions per minute (RPM) for 4 minutes. Portion of plasma containing platelets (platelet rich plasma) was taken in a tuberculin syringe containing calcium chloride (CaCl2). Ration was maintained at 1-part CaCl2 and 9-part PRP. Calcium chloride was the activator for platelets. A specific amount of PRP was injected at each site of post acne scar. Patients were asked to report the day when the erythema disappeared in both sides after each session, and if there any adverse reactions that may experience after the treatment. All patients were asked to avoid direct sun exposure, heat and friction on the treated areas. They were advised to apply sunscreen of sun protection factor (SPF) 30. One month after the initial treatment session, all participants received the second treatment session with the same protocol.
Patient Assessment
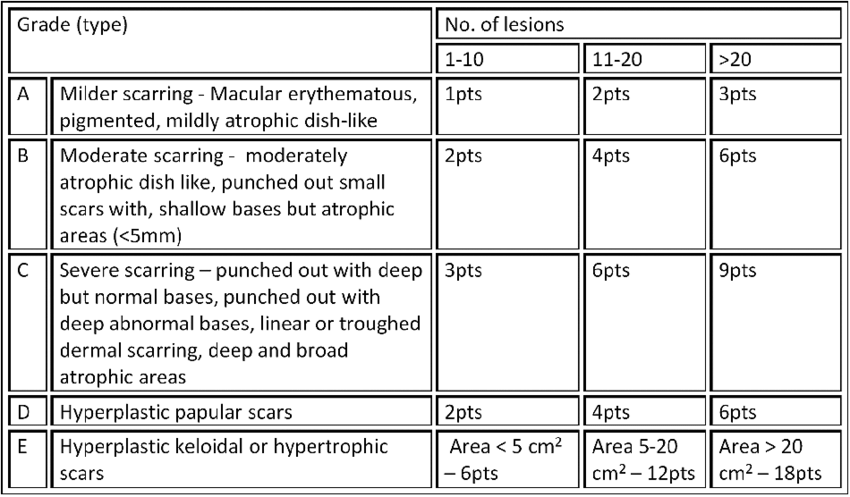
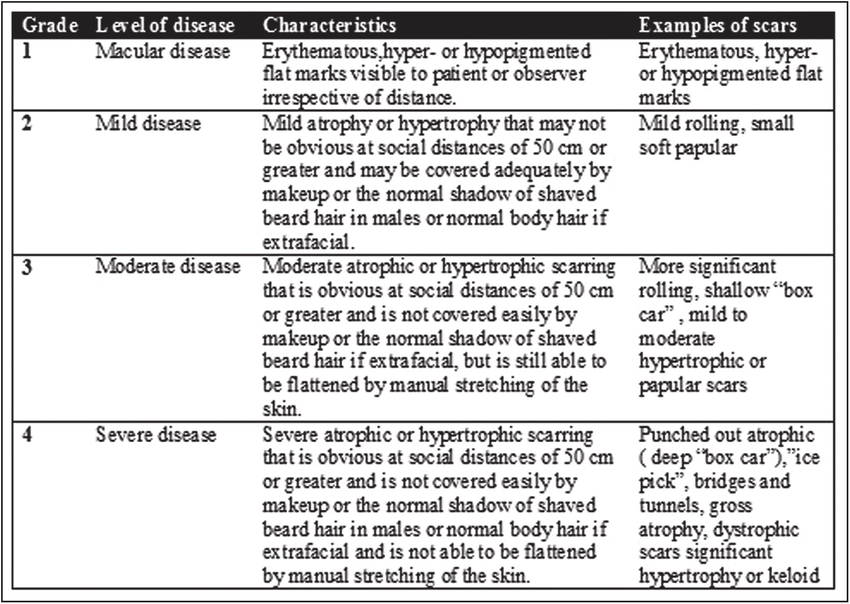
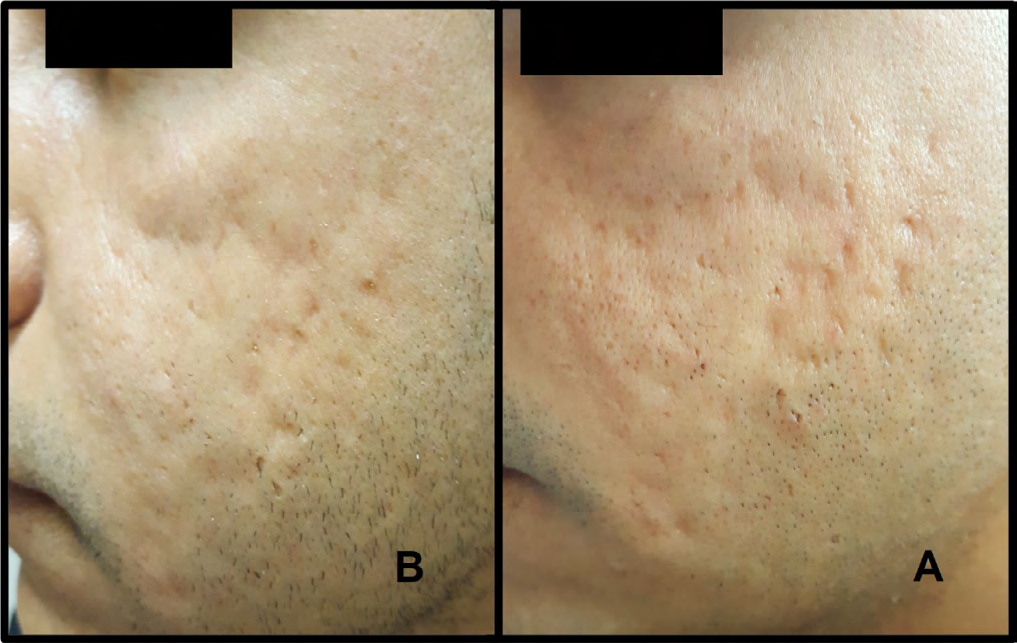
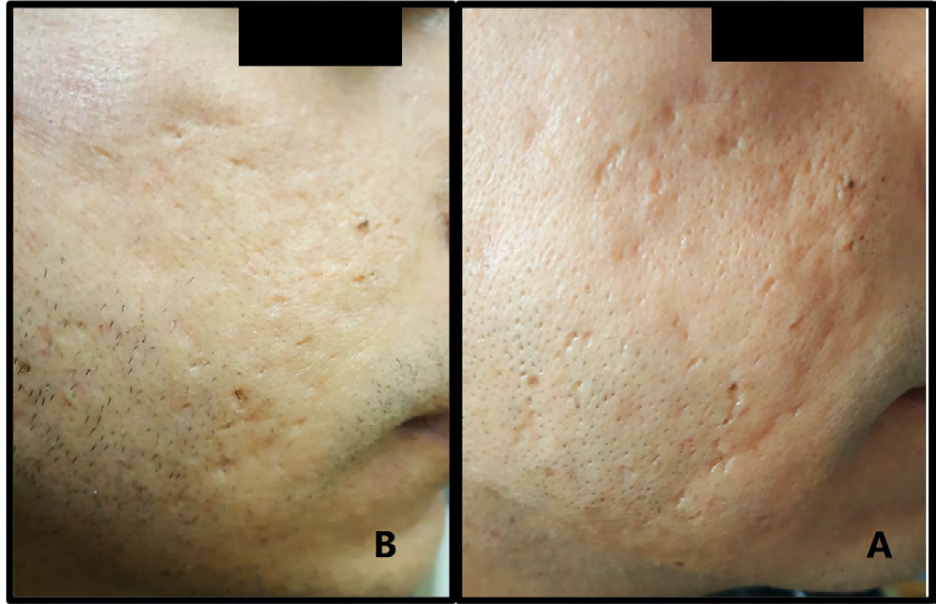
Participants were required to undergo serial photography of the lesions at baseline and after each treatment session (one month apart), using a digital camera. Camera setting, lighting and positioning were kept identical for all serial photographs. Scoring of acne scars was done using Goodman and Baron’s quantitative and qualitative global acne scarring grading system as shown in Figures 1 & 2.
Statistical Analysis
Data were analyzed using the IBM SPSS statistics (Version20).
Results
This study included 30 patients suffering from post-acne scars. Their age was between 22–45 years with a mean of (28.1± 6.4), 18 patients were females (60%) and 12 patients were males (40%). According to the Fitzpatrick classification of skin photo types, 4 patients (13.3%) were type II, 18 patients (60%) were type III, and 8 patients (26.7%) were of skin type IV as shown in Table 2.
| Characteristics | No. of patients | Percentage |
|---|---|---|
| Gender | ||
| Male | 12 | 40% |
| Female | 18 | 60% |
| Fitzpatrick skin photo type | ||
| II | 4 | 13.30% |
| III | 18 | 60% |
| IV | 8 | 26.70% |
Table 2: Patient characteristics
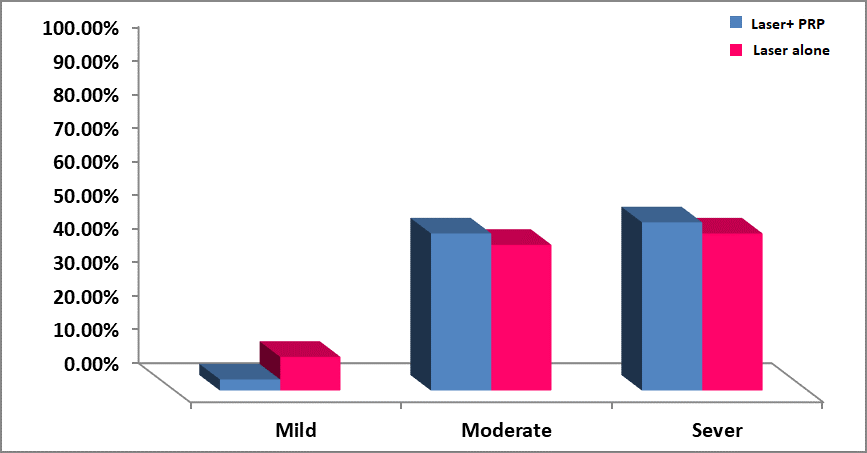
The severity of acne scars before treatment was graded according to the Qualitative Global Grading System and it was mild in 1 patient (3.3%) in the right side and in 3 patients (10%) in the left side, moderate in 14 patients (46.7%) in the right side and 13 patients (43.3%) in the left, and severe in 15 patients (50%) in the right and in 14 patients (46.7%) in the left as shown in Figure 3.
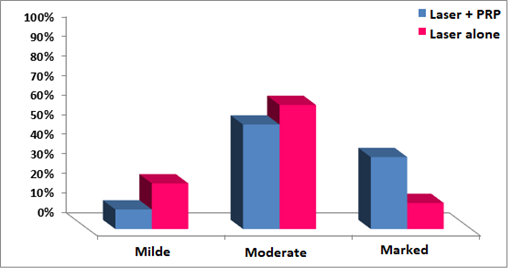
Physician’s assessment was done by blinded dermatologist using digital photographs. Improvement was noted on quartile scale where 0-25% was considered as mild improvement, 25-50% as moderate improvement, 50–75% as marked improvement and 75-100% as excellent improvement. Regarding clinical improvement, the right side of the face showed marked improvement in 11 patients (36.7%), 16 patients (53.3%) had moderate improvement, and 3 patients (10%) had mild improvement. On the other hand, the left side showed marked improvement among 4 patients (13.3%), moderate improvement in 19 patients (63.3%), and mild improvement in 7 patients (23.3%) (Figure 4).
The mean baseline Goodman and Baron’s quantitative score on the right side was 12.6 ± 3.8 and mean final score at the end of the study was 7± 3.4. On the left side, the mean baseline score was 11.3 ± 4.1 and mean final score was 8 ± 4.1. There was statistically significant difference in the quality of scars when the baseline scores were compared with the final scores of each side individually. Before and after scores were statistically significant (P = 0.0001) on the right side and similar results were seen on the left side (P = 0.0001) (Table 3).
| FCL+PRP | FCL alone | |
|---|---|---|
| Base line | 12.6±3.8 | 11.3±4.1 |
| After the 1st session | 12.1±3.9 | 11.2±4.1 |
| After 2nd session | 10.2±3.7 | 9.5±4.1 |
| After 3rd session | 7.7±3.4 | 8.1±3.9 |
| In the end of the treatment | 7±3.4 | 8±4.1 |
| P-value | 0.0001 | 0.0001 |
Table 3: Comparison of reduction of acne scar according to Goodman and Baron quantitative scale at baseline and in each session a
According to the previous table a noticeable decrease in the degree of acne scarring when starting treatment was noticed compared with the degree of it after treatment in each of the two sides, a marked decrease of 44.4% in the plasma with laser side while in the laser side only it reached 29.2%.
Adverse Effects
Figure 7 presents the adverse effects of the treatment reported by the patients in both the groups. The patients asked to report the day when the erythema disappeared in both sides after each session. In the current study, all patients developed post laser transient erythema and edema.
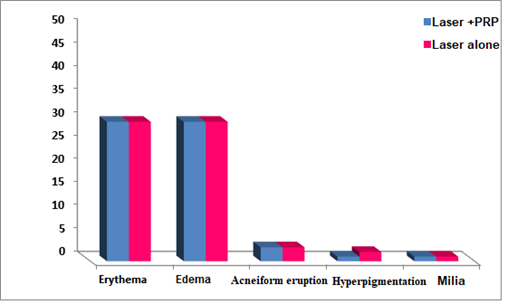
Two Patients presenting with post-inflammatory pigmentation after the third session one of them in the side of the laser alone, and the two of them were from IV skin photo type. Acneiform eruption was observed after treatment in three patients in the both sides and only one patient developed milia in both sides.
| Type of Treatment | ||||
|---|---|---|---|---|
| Laser + PRP | Laser | |||
| sessions | Mean ± SD | Range | Mean ± SD | Range |
| First | 4.26±1.1 | [3-5] | 6.1±1.06 | [4-7] |
| Second | 3.4±1.3 | [1-5] | 4.9±0.9 | [3-7] |
| third | 2.6±1.2 | [1-5] | 4.1±0.9 | [3-5] |
Table 4: Differences in the mean days of erythema in each of the two types of treatment We observe from the previous table the de
Table 4: Differences in the mean days of erythema in each of the two types of treatment We observe from the previous table the decrease in the average number of days of erythema with increased treatment sessions in both treatment patterns, especially in the laser + plasma group, where the percentage of decline was 38.9% compared to 32.8% in the laser group with a difference of statistical significance in the two groups.
Discussion
Acne scars cause cosmetic and psychological problems and still lack standardized treatment option. Various therapeutic options have been described with variable outcomes as well as complications. Fractional CO2 laser therapy is based on the theory of fractional photothermolysis, which creates microscopic zones of thermal injury and sparing normal healthy zones in between, which helps in rapid re-epithelization, tissue tightening, and new collagen formation, which in turn improves the appearance of wrinkles and atrophic acne scars [13]. Despite the documented efficacy of fractional CO2 laser resurfacing in the treatment of acne scars, its drawbacks such as long periods of erythema and edema may cause discomfort and hinder patients’ daily lives, limiting its use [14].
PRP contains multiple autologous growth factors, especially epidermal growth factor, platelet-derived growth factor, transforming growth factor β, vascular endothelial growth factor, and other cytokines and chemokines [10]. The right side of the face (combined PRP- and fractional CO2-treated side) showed significant clinical improvement compared with the left side, with much more favorable outcome. There was also a statistically significant reduction in the severity of acne scars on both sides of the face after treatment. These results were in agreement with those of Lee, et al. [15], who compared the effect of fractional CO2 laser plus PRP on one side versus fractional CO2 laser alone on the other side, and concluded that the overall degree of clinical improvement was significantly better on the PRP- treated side.
Our results also agree with those of Gawdat, et al. [9], who randomized the patients into four groups. They compared intradermal PRP plus fractional CO2 resurfacing versus fractional CO2 alone. They also compared intradermal PRP with fractional CO2 versus topical PRP plus fractional CO2. The clinical improvement was excellent in 66.7% of the patients who received fractional CO2 and intradermal PRP, 60% of the patients who received fractional CO2 and topical PRP, and 26.7% of the patients who were only treated by fractional CO2 laser, and there was a statistically significant improvement of the PRP-treated sides over the non-PRP- treated side.
The present study shows that patients rated a significantly lower scar severity score on the PRP side (7 ± 3.4) as compared to the laser alone treated side (8 ± 4.1). The results of the study show that adverse effects such as persistent erythema was disappeared faster in PRP side as compared to laser alone group.
These results verify that adjuvant PRP treatment may help promote the recovery of laser-damaged skin and decrease downtime. One of the earlier proposed mechanism of action for these observed effects may be the numerous growth factors present in PRP. Specifically, platelet-derived growth factor may help to stimulate the production of other growth factors important in tissue remodelling, promoting connective tissue healing by upregulating collagen and protein synthesis. Higher levels of transforming growth factor beta may also expedite tissue recovery through the up regulation of cellular migration and proliferation, as well as by directly stimulating cell replication and fibronectin binding interactions. Insulin-like growth factor may also assist in the proliferation and migration of fibroblasts and increase collagen production. Although the effects of epithelial growth factor are limited to the basal layer of the epidermis, it also promotes cell differentiation and re- epithelialization [16]. These growth factors may enhance the recovery of laser-damaged skin and shorten the duration and degree of postoperative erythema, and edema [17, 18, 19].
Conclusion
In conclusion, our results show that PRP treatment after ablative CO2 fractional resurfacing provides better overall clinical improvement and expedites the recovery of laser- damaged skin. We suggest that PRP should be considered as an adjuvant therapeutic option for dermatologic procedures such as fractional CO2 laser resurfacing as it might have additional benefit of reducing the adverse effects such as persistent erythema.
References
-
Rivera AE (2008) Acne scarring: a review and current treatment modalities. J Am Acad Dermatol 59(4): 659- 676.
-
Kadunc BV, de Almeida ART (2003) Surgical treatment of facial acne scars based on morphologic classification: a brazilian experience. Dermatol Surg 29(12): 1200-1209.
-
Dreno B, Khammari A, Orain N, Noray C, Merial-Kieny C, et al. (2006) Ecca grading scale: an original validated acne scar grading scale for clinical practice in dermatology. Dermatol 214(1): 46-51.
-
Sobanko JF, Alster TS (2012) Management of acne scarring, part I: acomparative review of laser surgical approaches. Am J Clin Dermatol 13(5): 319-330.
-
Kim HJ, Kim TG, Kwon YS, Park JM, Lee JH (2009) Comparison of a 1,550 nm erbium: glass fractional laser and a chemical reconstruction of skin scars (CROSS) method in the treatment of acne scars: a simultaneous split-face trial. Lasers Surg Med 41(8): 545-549.
-
Hedelund L, Moreau KE, Beyer DM, Nymann P, et al. (2010) Fractional nonablative 1,540-nm laser resurfacing of atrophic acne scars. A randomized controlled trial with blinded response evaluation. Lasers Med Sci 25(5): 749- 754.
-
Chapas AM, Brightman L, Sukal S, Hale E, Daniel D, et al. (2008) Successful treatment of acneiform scarring with CO2 ablative fractional resurfacing. Lasers Surg Med 40: 381-386.
-
Kumaran MS, Arshdeep A (2014) Platelet-rich plasma in dermatology:boon or a bane? Indian J Dermatol Venereol Leprol 80(1): 5-14.
-
Gawdat HI, Hegazy RA, Fawzy MM, Fathy M (2014) Autologous platelet rich plasma: topical versus intradermal after fractional ablative carbon dioxide laser treatment of atrophic acne scars. Dermatol Surg 40(2): 152-161.
-
Kang BK, Lee JH, Shin MK, Kim NI (2013) Infraorbital rejuvenation using PRP (platelet-rich plasma): A prospective, randomized, split-face trial. J Am Acad Dermatol 68: SAB24.
-
Goodman GJ, Baron JA (2006) Postacne scarring: a qualitative global scarring grading system. Dermatol Surg 32: 1458-1466.
-
Goodman GJ, Baron JA (2006) Postacne scarring--a quantitative global scarring grading system. J Cosmet Dermatol 5(1): 48-52.
-
Majid I, Imran S (2014) Fractional CO2 laser resurfacing as monotherapy in the treatment of atrophic facial acne scars. J Cutan Aesthet Surg 7(2): 87.
-
Hwang YJ, Lee YN, Lee YW, Choe YB, Ahn KJ (2013) Treatment of acne scars and wrinkles in asian patients using carbon-dioxide fractional laser resurfacing: its effects on skin biophysical profiles. Ann Dermatol 25(4): 445-453.
-
Lee JW, Kim BJ, Kim MN, Mun SK (2011) The efficacy of autologous platelet rich plasma combined with ablative carbon dioxide fractional resurfacing for acne scars: a simultaneous split-face trial. Dermatol Surg 37(7): 931- 938.
-
Sampson S, Gerhardt M, Mandelbaum B (2008) Platelet rich plasma injection grafts for musculoskeletal injuries: a review. Curr Rev Musculoskeletal Med 1(3-4): 165-174.
-
Eppley BL, Pietrzak WS, Blanton M (2006) Platelet-rich plasma: a review of biology and applications in plastic surgery. Plastic Reconstructive Surg 118(6): 147-159.
-
Marx RE (2004) Platelet-rich plasma: Evidence to support its use. J Oral Maxillofac Surg 62: 489-496.
-
Robiony M, Polini F, Costa F, Politi M (2002) Osteogenesis distraction and platelet-rich plasma for bone restoration of the severely atrophic mandible: Preliminary results. J Oral Maxillofac Surg 60: 630-635.
- Epithelioid Granuloma; 3cases with Different Clinical Features
- Advancing Representation in Dermatology Clinical Trials: Ethical, Scientific, and Regulatory Imperatives for Inclusion Across all Fitzpatrick Skin Types
- A Case of Atopic Dermatitis with Concurrent Psoriasis Vulgaris: Successful Treatment with Upadacitinib
- Innovation Lifting Eyeshadow: A Synthesis of Makeup and Optical Illusion
- Distinguishing Superficial Actinic Porokeratosis from Actinic Keratosis with UVF Dermoscopy: A Case Report
- High Mobility Group Box 1 (HMGB1) in Cutaneous Inflammation: An Immune Modulator Bridging Cellular Stress, Ferroptosis and Danger Signaling