Keratoacanthoma: A Diagnostic and Therapeutic Conundrum
Keratoacanthoma is a squamoproliferative disorder with varying presentations and subtypes. However, debates persist regarding its classification as a benign and spontaneously resolving tumor, while other authors consider it a rare variant of cutaneous squamous cell carcinoma with metastatic potential. Consequently, there is a lack of standard practice guidelines regarding the workup and management of such lesions. Therefore, invariably, some lesions of keratoacanthoma may be missed due to a low index of suspicion, inadequate workup, or spontaneous resolution without histological evidence. Herein, we present the case of a 46-year-old housewife with a mass over the lower lip who was diagnosed with keratoacanthoma following histopathological examination, which is in contrast with the usual site and exposure history in keratoacanthoma. Additionally, we present a review of the literature on the topic and the controversies associated with the diagnosis and management of keratoacanthoma to aid physicians in suspecting and diagnosing this entity accurately.
Introduction
Keratoacanthoma (KA) is a cutaneous squamoproliferative tumor. It is divided into different subtypes with varying presentations, such as solitary keratoacanthoma, subungual KA, mucosal KA, giant KA, KA centrifugum marginatum, generalized eruptive KA of Grzybowski, and Ferguson– Smith syndrome with multiple KAs [1]. Definitive guidelines regarding its treatment are lacking because of debates over its classification as a benign, spontaneously resolving tumor versus a variant of cutaneous squamous cell carcinoma with rare potential for metastasis. In clinical practice, KA can be missed as it is either confused for squamous cell carcinoma or it resolves spontaneously without being reported [2]. However, it is critical to diagnose KA accurately to rule out squamous cell carcinoma and metastases. Herein, we present the case of a 46-year-old woman who was diagnosed with KA to highlight the clinical difficulties encountered with KA.
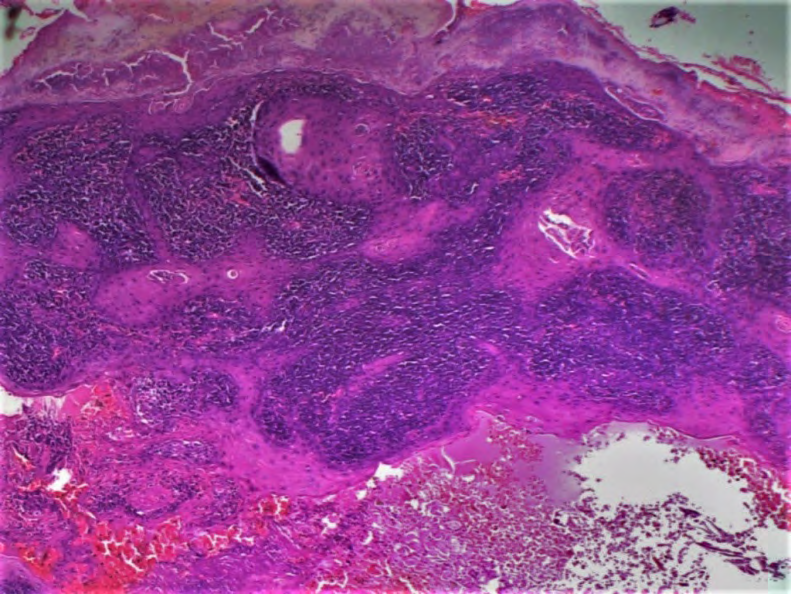
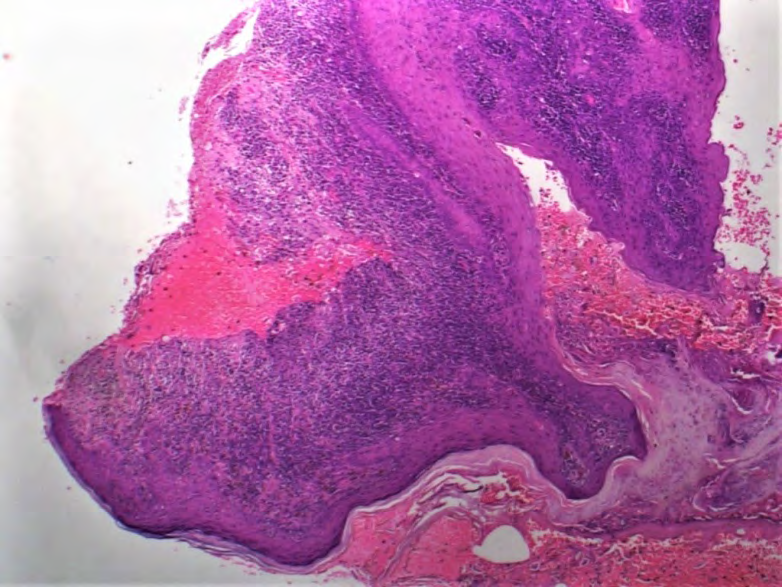
A 46-year-old housewife presented to the outpatient department of dermatology at Belagavi Institute of Medical Sciences, India with a growing mass over the right lower lip for 4 months (Figure 1). The mass began as a small, painless papule and progressively increased in size. No history of trauma, infections, or pain over the area were noted. There was no history of similar lesions at other sites. None of the family members had similar lesions. On examination, a 2 x 3-cm vegetative mass was noted on the right lower lip. Excision biopsy followed by histopathological examination was advised to rule out squamous cell carcinoma. The histopathological examination revealed hyperplasia of contiguous follicular infundibula with pseudocarcinomatous hyperplasia, peripheral hyperplastic overhanging lips, and lamellated parakeratotic and dyskeratotic plugs (Figure 2). The surface revealed papillomatosis, hypergranulosis, and orthokeratosis with foci of parakeratosis and encroachment of the dermo-epidermal junction with lymphocytes and necrotic keratinocytes/colloid bodies. The margins were

clear. Post-procedurally, the lip was sutured using 3-0 non- absorbable sutures with no adverse events or recurrence till 6 months.

Discussion
Keratoacanthoma was first described by Sir Jonathan Hutchinson in 1888 [3, 4]. However, the epidemiological characteristics, histopathological diagnostic criteria, prognosis, and treatment guidelines of KA are confusing and non-standardized. Therefore, the diagnosis of KA requires a high index of suspicion and prompt treatment in view of risk of metastatic changes. In some cases, the clinical course of KA can result in spontaneous involution as well.
KA is generally encountered in elderly patients and especially over the sun-exposed parts of the body. In contrast, our patient was a middle-aged housewife without signs of photodamage over the lips. Additionally, KA is commonly encountered in the sixth and seventh decades; in contrast, our patient was a middle-aged person. The familial type of multiple eruptive KA of Ferguson–Smith has its onset in adolescence or earlier. In temperate regions, 70% of KAs are localized to the face, while in the subtropics they involve the arms, dorsa of hands, and lower extremities [5]. Even though our patient is from the tropical region, the lesion was noted on the lower lip.
KAs are squamoproliferative tumors primarily of the hair-bearing skin. They are characterized by a triphasic pattern of evolution. The initial stage is a proliferative (early) stage characterized by rapid growth. The subsequent stage of stabilization (well-developed) is characterized by a fixed size of the the lesion, while the late stage of regression is characterized by spontaneous involution. Interestingly, this clinical course mimics the hair cycle to some extent [3, 6, 7, 8]. In our case, the patient was in the early proliferative phase.
The diagnosis and treatment of KA requires an interdisciplinary approach. Conventional surgical excision is the treatment of choice for solitary KA since it allows for both the histopathologic assessment as well as the removal of the tumor. Consequently, surgical excision was performed, and the excised tissue was sent for histopathological excision. Additionally, there was no recurrence for 6 months. However, other therapies include electrodesiccation and curettage; ionizing radiation; intralesional pharmacologic therapy, such as methotrexate, 5-fluoruracil, and bleomycin; photodynamic therapy; and topical treatment with 5-fluoruracil and imiquimod [8]. However, topical treatment is often time- consuming and may be associated with skin discoloration and pain [1].
The prognosis of KA is excellent following surgical excision. Generally, patients with KA will require long-term follow-up to screen for new primary skin cancers. Metastasis of KA is rare but is a possibility. The treating physician must advice the patient regarding sun-protective measures using protective clothing and sunscreen and must advise the patient about further reducing the sun exposure.
References
-
Zito PM, Scharf R (2022) Keratoacanthoma. Treasure Island (FL): StatPearls Publishing.
-
Kwiek B, Schwartz RA (2016) Keratoacanthoma (KA): An update and review. J Am Acad Dermatol 74(6): 1220- 1233.
-
Hutchinson J (1889) The crateriform ulcer of the face: A form of epithelial cancer. Trans Pathol Soc London 40: 275-281.
-
Hutchinson JA (1888) A peculiar form of cancer of the skin. _In:_ Smaller Atlas of Illustrations of Clinical Surgery. 2nd (Vol.), Philadelphia: Blakiston, pp: 921.
-
Khandpur S, Ramam M (2022) Skin Tumors. In: Sacchidanand S, Oberai C, et al. (Eds.), IADVL Textbook of Dermatology. Mumbai: Bhalani Book Depot, pp: 2075- 154.
-
Nagarajan P (2020) Differentiating keratoacanthoma from squamous cell carcinoma—In quest of the holy grail. J Cutan Pathol 47(4): 418-420.
-
Schwartz RA (2004) Keratoacanthoma: a clinico- pathologic enigma. Dermatol Surg 30(2): 326-333.
-
Tisack A, Fotouhi A, Fidai C, Friedman BJ, Ozog D, et al. (2021) A clinical and biological review of keratoacanthoma. Br J Dermatol 185(3): 487-498.
- Epithelioid Granuloma; 3cases with Different Clinical Features
- Advancing Representation in Dermatology Clinical Trials: Ethical, Scientific, and Regulatory Imperatives for Inclusion Across all Fitzpatrick Skin Types
- A Case of Atopic Dermatitis with Concurrent Psoriasis Vulgaris: Successful Treatment with Upadacitinib
- Innovation Lifting Eyeshadow: A Synthesis of Makeup and Optical Illusion
- Distinguishing Superficial Actinic Porokeratosis from Actinic Keratosis with UVF Dermoscopy: A Case Report
- High Mobility Group Box 1 (HMGB1) in Cutaneous Inflammation: An Immune Modulator Bridging Cellular Stress, Ferroptosis and Danger Signaling