A Case of Tinea pseudoimbricata Caused by Microsporum Audouinii
Tinea pseudoimbricata has morphological similarity to Tinea imbricata which is characterized by multiple concentric rings, but it is caused by dermatophytes other than Trichophyton concentricum. We report a case of tinea pseudoimbricata caused by Microsporum audounii that presented with multiple concentric scaly annular erythema. The most common clinical presentation of pseudoimbricata was tinea corporis followed by Tinea cruris. However, tinea imbricate-like lesions are very rare. Tinea pseudoimbricata is considered a unique sub-type of Tinea incognito which caused by inappropriate use of topical steroid. Both Fungal culture and microscopic findings confirmed Microsporum audouinii infection in this case. The patient was treated with oral terbinafine according to culture and antifungal sensitivity testing at a dose of 250 mg/day for 8 weeks.
Introduction
Dermatophytosis has been increasing in the past few years at a frightening rate. Patients have presented with extensive, recurrent, and recalcitrant disease often with atypical morphology of superficial dermatophytosis. Widespread availability of over‑the‑counter potent and super‑potent topical steroids (alone or in combination with antifungals and antibiotics) and self‑medication have led to the evolution of an atypical presentation of dermatophytosis, Tinea incognito [1].
Tinea imbricata is a unique dermatophytosis caused by Trichophyton concentricum. It is commonly found in Southeast Asia, South Pacific and Central and South America [2]. It commonly presents as concentric erythematous scaly rings on the trunk or limbs. Other Dermatophytes as Tinea pseudoimbricata can mimic this presentation. Tinea pseudoimbricata is caused by T_. mentagrophytes, T. rubrum, _T. tonsurans, Microsporum audouinii and Microsporum gypseum [1, 3, 4].
It is often seen in immune-compromised individuals or in patients with a history of steroid abuse. This condition has been postulated to occur as a result of local immunosuppression induced by topical steroids [3]. Another alarming fact is the positive family history in some patients which might be responsible for the reinfection in these patients [1].
Case Report
A female Indian patient aged 22 years came to Egypt in the last 9 months. The condition started one year ago. Initially the patient had repeated 2-week course of kenacomb. She eventually sought medical advice from a dermatologist and was treated with fluconazole (fungican 150 mg cap once/week for 2weeks) and antihistamines with mild improvement. The condition worsened 5 months later using the same treatment. No history of contact with animals or birds. No history of hypertension, the patient is proved to be prediabetic. No other apparent internal diseases.
The patient reported that her husband had a similar

Figure 1a Figure 1b
condition. After Mycological culture it was the same isolated strain of fungi.
On clinical examination the patient presented with multiple concentric scaly erythematous, annular plaques giving the pattern of “ring within ring” appearance. The number of concentric rings ranged from 2-3. The condition is associated with severe pruritus and runs a chronic course. The lesions are disseminated in different body sites as; trunk (over the breast), back, buttock, abdomen, groin, thigh, leg, and dorsum of the foot (near lateral malleoli) (Figures 1 a-e) respectively. According to the multiple site involvement, the patient thus has extensive tinea corporis and cruris.
Figure 1c Figure 1d Figure 1e Figure 1a-e: Various clinical presentations of the patient with Tinea pseudoimbricata multiple concentric scaly erythematous patches. (a) on abdomen (b) on trunk (c) on back (d) on thigh (e) on foot Scrapings from the skin at the edges of the lesions were taken for KOH wet mount for direct microscopic examination and fungal culture. Fungal culture was done on Mycobiotic agar (Conda lab-Spain) and DTM (HI Media-India). Antifungal sensitivity test for the isolate using disc diffusion method was done on Brain heart infusion agar (HI Media) with discs of Terbinafine, Voriconazole, Itraconazole, Fluconazole supplied from Conda lab.
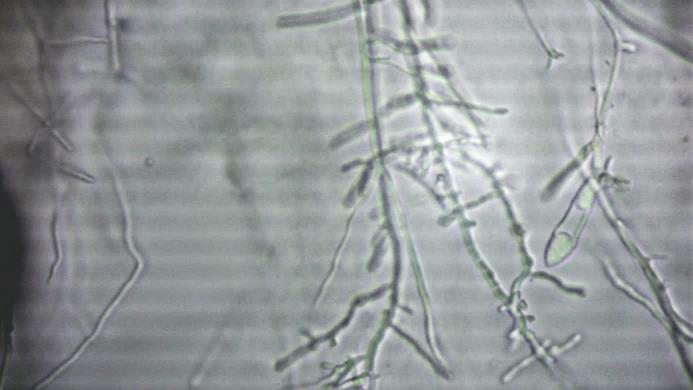
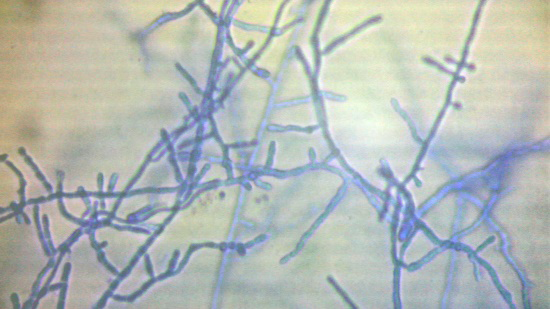
Direct microscopic Examination revealed branched

Figure 5: M. audouinii Showed pectinate hyphae. Microconidia (red arrow) and macroconidia cells (black arrows). Antifungal sensitivity test with disc method showed high sensitivity to Terbinafine Itraconazole and Voriconazole while moderate sensitivity to Fluconazole and Miconazole. The patient was treated with oral Terbinafine as dose of 250 mg/day for 8 weeks which showed marked improvement from fourth week.
Figure 4: Microscopic feature of M. audouinii with characterestic pectinate bodies septate hyphae while on culture media dermatophyte isolate was obtained which identified according to its macro- morphological and micro-morphological characters as M. audouinii. Colonies of M. audouinii isolate showed white surface color on mycobiotic with radiating edges turns red on DTM. the isolate turned the medium to red. Microscopic examination of the colonies showed the characteristic of M. audouinii as pectinate hyphae, microconidia and rudimentary macroconidia.
$$ \mathrm {E} = \frac {1}{2} \mathrm {A} ^ {2} + \mathrm {B} ^ {2} $$
$$ \mathrm {E} = \frac {1}{2} \mathrm {A} ^ {2} + \frac {1}{2} \mathrm {B} ^ {2} $$ $$ \downarrow $$
Discussion
Tinea pseudoimbricate or tinea indecisiva are used to describe a clinical presentation that is similar to that of tinea imbricate. However, it is caused by different dermatophytes than the ones caused tinea imbricata T. concentricum. The
first reported case of tinea pseudoimbricata dates back to 1987 which was caused by Microsporum ferrugenum [5]. Tinea pseudoumbricata is encountered more often nowadays due to the misuse of topical steroids. The diagnosis of tinea pseudoimbricata mandates a positive culture [7]. The literature showed that Tinea pseudoumbricata is common in India [1, 6, 7].
Our patient presented with multiple, concentric, annular, erythematous scales with multiple sites involvement on abdomen and groin with extensive tinea corporis and tinea cruris, a picture, which agrees Sun and Ho who described similar presentation [8, 7]. KOH preparation and fungal culture for our case revealed Microsporum audouinii which is coincide with the fact that the disease caused by different dermatophytes as T. tonsurans, T. mentagrophytes, T. rubrum, M. audouinii and M. ggypseum [1, 3, 4]. In Egypt M. audouinii is rare as a cause of tinea capitis, corporis and cruris. The present case is the first of pseudoimbricata - to our knowledge – reported in spite of common occurrence of Tinea incognito. The exact etiopathogenesis is not known, but it can occur in our patient due to some degree of immunosuppression, as a result of application of topical steroids with a confounding effect of associated prediabetes.
A hypothesis that can explain the concentric rings presentation of Tinea pseudoimbricata is that Fungal invasions trigger the host immune response result in suppression of the fungal cell growth [1, 8]. Topical application of potent steroid causes local immunosuppression which may diminish the host responses, specifically the cellular immune responses, against the fungus which would lead to flare up of the infection. Intermittent therapy with topical steroids without antifungals leads to repeat of this cycle many a times forming the ring in ring appearance. In addition, we can postulate depending on the cases published and our case that Indian people may be more affected by tinea pseudoimbricata may be due to some of genetic factors [6].
Tinea pseudoimbricata is encountered more often nowadays due to the misuse of topical steroids, and to diagnose tinea pseudoimbricata culture is mandatory. The morphology of concentric rings is not restricted to Trichophyton concentricum but can occur with other species depending on the clinical scenario.
According to culture and antifungal sensitivity testing, the patient was prescribed oral terbinafine at a dose of 250 mg/day for 8 weeks. The patient showed marked improvement on terbinafine at 4 weeks.
Besides, general measures are important to treat the family members to avoid spread of the infection to household members. In our case to decrease the chances of reinfection we advised separate washing of infected clothes and avoidance of sharing of towels, clothes, bed linen, and soaps [1].
References
-
Singal A, Jakhar D, Kaur I, Pandhi D, Das S (2019) _Tinea_ _pseudoimbricata_ as a unique manifestation of steroid abuse: A clinico-mycological and dermoscopic study from a tertiary care hospital. Indian Dermatolo Online J 10(4): 422-425.
-
Baiofaz A, Conzalez V (2011) Tinea imbricate in the Americans. Curr opin infect Dis 24(2): 106-111.
-
Lee JS, Choi YW, Park JS (2021) A Case of _Tinea_ _pseudoimbricata_ by Trichophyton tonsurans. J Mycol Infect 26(1):13-16.
-
Rao AG, Datta N (2013) Tinea corporis due to Trichophyton mentagrophytes and Trichophyton tonsurans mimicking tinea imbricata. Indian J Dermatol Venereol Leprol 79(4): 554.
-
Lee KH, Lee ES, Kang WH, Lee S (1987) An unusual clinical manifestation of tinea corporis caused by Microsporum ferrugenium. Korean J Dermatol 25: 383-388.
-
Jartarkar SR, Patil A, Goldust Y, Cockerell CJ, Schwartz RA, et al. (2022) Pathogenesis, Immunology and Management of Dermatophytosis. Journal of Fungi 8(1): 39.
-
Bhagyashree M, Shilpashree PA (2022) A Clinico Mycological Study of _Tinea pseudoimbricata_. Indian Dermatol Online J 13(1): 73-77.
-
Sun PL, Ho HT (2006) Concentric rings: An unusual presentation of tinea corporis caused by Microsporun gypseum. Mycoses 49(2): 150‑151.
- Epithelioid Granuloma; 3cases with Different Clinical Features
- Advancing Representation in Dermatology Clinical Trials: Ethical, Scientific, and Regulatory Imperatives for Inclusion Across all Fitzpatrick Skin Types
- A Case of Atopic Dermatitis with Concurrent Psoriasis Vulgaris: Successful Treatment with Upadacitinib
- Innovation Lifting Eyeshadow: A Synthesis of Makeup and Optical Illusion
- Distinguishing Superficial Actinic Porokeratosis from Actinic Keratosis with UVF Dermoscopy: A Case Report
- High Mobility Group Box 1 (HMGB1) in Cutaneous Inflammation: An Immune Modulator Bridging Cellular Stress, Ferroptosis and Danger Signaling