The Conundrum of Mixed Pilomatrixoma and Basal Cell Carcinoma: A Case Report and Literature Review
Pilomatrixoma is a common tumour found most often in cutaneous or subcutaneous location on the upper half of the body of children and young adults. Basal cell carcinoma (BCC) is a very common malignant cutaneous neoplasm found most often on the face of middle age and old people. A collision of BCC and pilomatrixoma is a very rare occurrence and only two cases have been reported in the English literature [1,2]. We present a case of pilomatrixoma and basal cell carcinoma occurring on the face of an 83-year-old white female patient. We considered the possibilities of a collision tumour of BCC and pilomatrixoma, BCC originating from long standing pilomatrixoma, BCC with matrical differentiation, and pilomatrix carcinoma and favoured the former two scenarios. Pilomatrix carcinoma was excluded in view of the histological and immunohistochemical findings and the clinical presentation.
Case Report
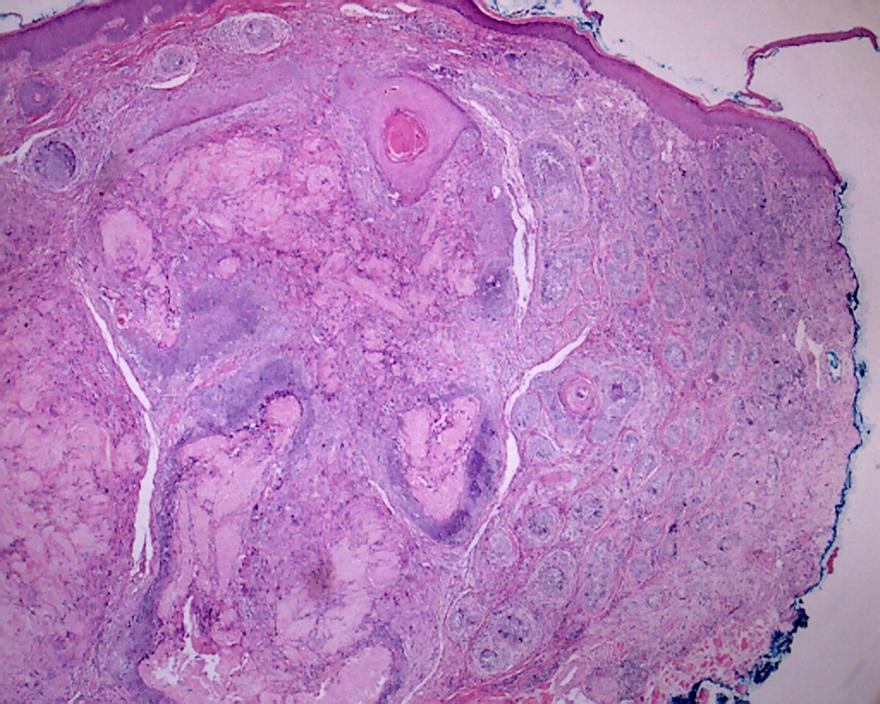
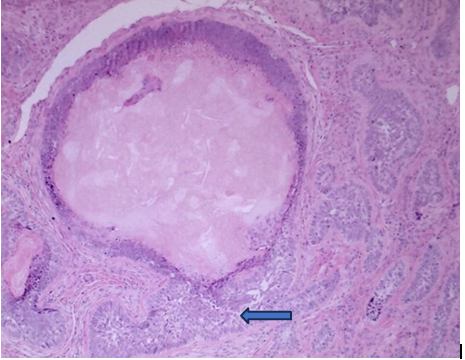
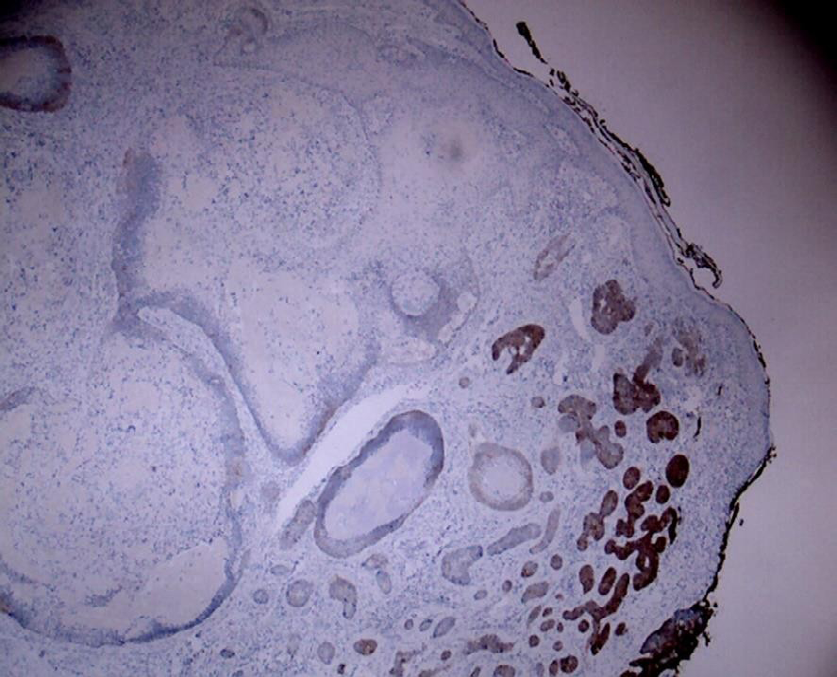
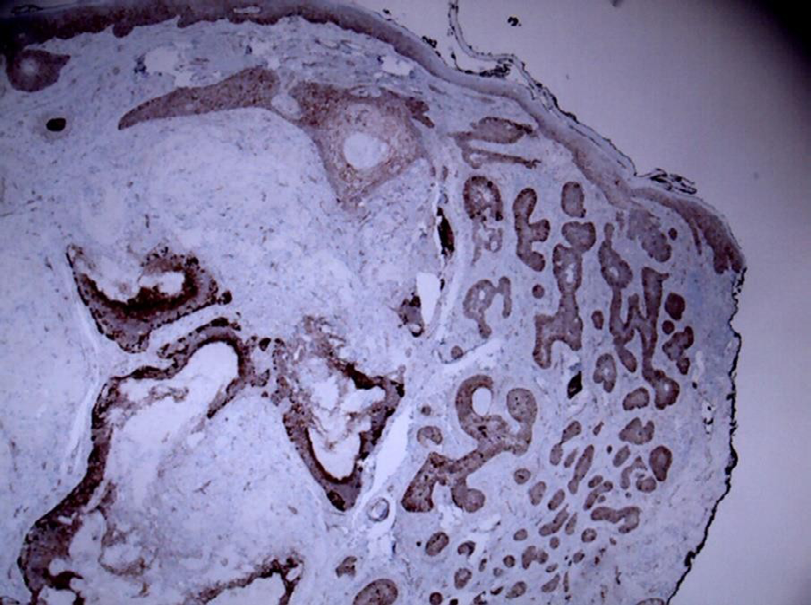
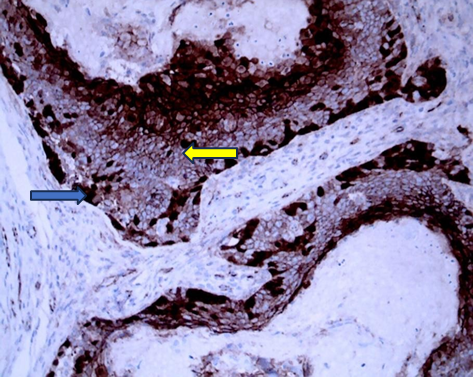
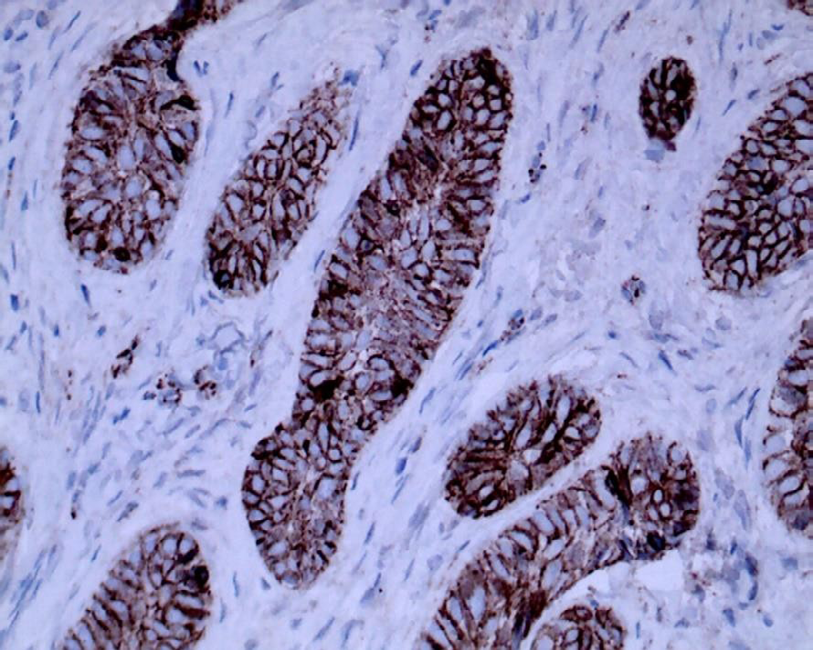
The patient was an 83-year-old white female who presented with a long-standing nodule on the right side of the face (Figure 1) with a provisional clinical diagnosis of dermatofibroma. A wide excision of the lesion was performed and the specimen comprised an ellipse of skin 9x6x4mm with a slightly raised 5mm pink nodule. Microscopic examination revealed a predominantly dermal tumour with focal connection to the dermo-epidermal junction and composed of lobules of ghost cells surrounded by basaloid epithelium typical of pilomatrixoma, immediately adjacent to collection of malignant basal cells with characteristic peripheral palisading of nuclei infiltrating to the deep dermis confirming invasive basal cell carcinoma (Figures 1 & 2). Ber-EP4 stain was positive in the BCC and negative in the pilomatrixoma component (Figure 3). β catenin stain was characteristically seen in the nuclei of the basaloid cells of pilomatrixoma, cell membrane and cytoplasm of BCC and negative in the transitional cells and ghost cells (Figures 4-6).
A combined basal cell carcinoma and pilomatrixoma was diagnosed in view of the presence of two separate components with characteristic histological and immunohistochemical profiles. We were unable to distinguish between a collision tumour and BCC arising in a pilomatrixoma. We considered BCC with matrical differentiation unlikely in view of the long history of the lesion and we were able to exclude pilomatrix carcinoma based on the histology.
Discussion
Pilomatrixoma (pilomatricoma, calcifying epithelioma of Malherbe) is a relatively common benign skin appendage tumour with follicular differentiation, accounts for almost 20% of pilar tumours and is frequently found on the head, neck and upper extremities mostly in the first two decades of life [3]. Pilomatrixoma is a slow growing pink or tan papule or nodule which is usually asymptomatic but may be associated with local irritation, discharge or even ulceration [4, 5]. Imaging in particular ultrasonography is usually helpful in distinguishing hypoechoic and calcified pilomatrixoma from other skin tumours [6]. Histologically, a mixture of basaloid, transitional and shadow cells is characteristic of pilomatrixoma [7]. Immunohistochemically, the nucleus and cell membrane of basaloid cells show strong β catenin staining whereas BerEP4 stain is typically negative [8].
BCC is the most common malignant tumour of skin and usually occurs in the elderly mostly in the head and neck [9]. BCC presents mostly as a pink or flesh colored papule or nodule [10]. The diagnostic histologic features of BCC include, basaloid cells with thin pale cytoplasm and round or oval nuclei. Peripheral border of cells with palisaded nuclei is a characteristic feature and artifactual separation of cell nests forming retraction artifacts can also be identified in BCC.9 BCC is typically positive with BerEP4.8 Most BCC are slow growing, non-metastasizing tumours and are cured by local excision [11].
Very rarely, BCC and pilomatrixoma can occur together at one site [1, 2]. This occurrence could represent collision tumour or BCC originating from long standing pilomatrixoma. BCC with matrical differentiation and pilomatrix carcinoma need to be considered in the presence of a malignant tumour with matrical features. In our case, the long-standing nature of the tumour supported a component of pilomatrixoma. In the presence of malignant changes with basaloid differentiation, a basal cell carcinoma arising in or colliding with a pilomatrixoma and BCC with matrical differentiation would seem the most likely scenarios. Pilomatrix carcinoma arising from a long standing pilomatrixoma is also a possibility.
Pilomatrix carcinoma is a very rare aggressive tumour with close to 150 cases reported in the English literature [12, 13, 14, 15]. It commonly presents as a non tender, firm dermal swelling mostly in the head and neck region of the elderly arising de novo or resulting from malignant transformation of preexisting pilomatrixoma [12, 13, 14, 15]. Characteristically, it is composed of pleomorphic basaloid cells with anaplastic nuclei, prominent nucleoli and frequent mitotic figures. Keratotic matrix and shadow cells can be seen in the center of the malignant basaloid islands. Pilomatrix carcinoma shares the same CNNB1 gene mutation with pilomatrixoma and shows nuclear β catenin positivity [12] BerEP4 is positive in the basaloid cells and negative in the ghost cells [12]. It is of paramount importance to distinguish pilomatrix carcinoma, an aggressive tumour with increased risk of nodal or visceral metastases warranting wide local excision with possible lymph node dissection from mixed BCC and pilomatrixoma [12]. The absence of anaplasia combined with the typical features of BCC and pilomatrixoma excluded a pilomatrix carcinoma.
BCC with matrical differentiation is an extremely rare tumour with 30 cases reported in the English literature [16]. Histologically, these tumours exhibit shadow cells in addition to typical features of BCC [17]. BerEP4 is positive in the follicular germinative cells and markedly reduced or negative in the matrical areas and the reverse pattern is seen with β-catenin [17]. Although the immunohistochemical profile is identical to our case, BCC with matrical differentiation was excluded based on the presence of two distinct components and the long history of the lesion.
Furthermore, the two other more favorable diagnoses considered in this setting were collision tumour and BCC arising from long standing pilomatrixoma, both very rare occurrence with only two cases reported of the former and no reported cases of the latter despite thorough literature review [1, 2]. In our case, the occurrence of two distinct pilomatrixoma/BCC components supported a collision tumour. The possibility of BCC arising in pilomatrixoma could not be excluded as malignant basal cell clusters were juxtaposed to basaloid cells of pilomatrixoma (Figure 2) and because of the long-standing nature of the lesion. A collision tumour, BCC originating from pilomatrixoma and BCC with matrical differentiation require similar treatment and have identical prognosis as a BCC but it is essential to rule out a pilomatrix carcinoma requiring different treatment and imparting a worse prognosis [11, 12].
Conclusion
In conclusion, in the presence of a tumour with malignant basaloid and matrical components, one must consider a collision tumour of BCC and pilomatrixoma, BCC with matrical differentiation, BCC arising in pilomatrixoma and pilomatrix carcinoma. The presence of marked atypia, abundant mitoses with abnormal forms, tumour necrosis and lymphovascular invasion favour pilomatrix carcinoma. Distinguishing the other three scenarios is more challenging as they share similar histological and immunohistochemical features. Fortunately, treatment and prognosis are dependent on the extent of the BCC component.
References
-
Shapiro L (1968) Association of pilomatrixoma (calcifying epithelioma) and basal-cell carcinoma: a case report. J Pathol Bacteriol 95(2): 558-560.
-
Khon B, John L, Chin M (2019) Collision Tumour: Basal Cell Carcinoma, Pilomatrixoma and Seborrhoeic Keratatosis. In: Abstact book of 24th world congress of Dermatology.
-
Hurt MA, Weedon D (2012) Weedon D.Weedon’s Skin Pathology.3rd ed.2010.Churchill,Living stone :Elseveir;2010. Dermatol Pract Concept 2(1): 79-82.
-
Laffargue JA, Stefano PC, Vivoda JL, Yarza ML, Bellelli AG, et al. (2019) Pilomatrixomas in children: Report of 149 cases. A retrospective study at two children’s hospitals. Arch Argent Pediatr 117(5): 340-343.
-
Pirouzmanesh A, Reinisch JF, Gonzalez-Gomez I, Smith EM, Meara JG (2003) Pilomatrixoma: a review of 346 cases. Plast Reconstr Surg 112(7): 1784-1789.
-
Hu JL, Yoo H, Kwon ST, Kim S, Chung JH, et al. (2020) Clinical analysis and review of literature on pilomatrixoma in pediatric patients. Arch Craniofac Surg 21(5): 288-293.
-
Le C, Bedocs PM (2023) Calcifying Epithelioma of Malherbe. In: StatPearls.
-
Alhumaidi A (2012) Practical immunohistochemistry of epithelial skin tumor. Indian J Dermatol Venereol Leprol 78(6): 698-708.
-
Rosai J (2011) Rosai and Ackerman’s Surgical Pathology, 10th (Edn.), Missouri: Mosby Elsevier: Ch.4.
-
Scrivener Y, Grosshans E, Cribier B (2002) Variations of basal cell carcinomas according to gender, age, location and histopathological subtype. Br J Dermatol 147(1): 41- 47.
-
Johnston R (2023) Weedon’s Skin Pathology 3rd edition. Churchill Livingstone: Elsevier; Ch 31.
-
Martin S, DeJesus J, Jacob A, Qvavadze T, Guerrieri C, et al. (2019) Pilomatrix carcinoma of the right postauricular region: A case report and literature review. Int J Surg Case Rep 65: 284-287.
-
Anand R, Kanuj M, Shirley S (2023) Pilomatrix Carcinoma-Rare Presentation of an Unusual Cutaneous Malignancy. Gulf J Oncolog 1(41): 107-110.
-
Jones C, Twoon M, Ho W, Portelli M, Robertson BF, et al. (2018) Pilomatrix carcinoma: 12- year experience and review of the literature. J Cutan Pathol 45(1): 33-38.
-
Aherne NJ, Fitzpatrick DA, Gibbons D, Armstrong JG (2008) Pilomatrix carcinoma presenting as an extra axial mass: clinicopathological features. Diagn Pathol 3, pp: 47.
-
Kyrpychova L, Carr RA, Martinek P, Vanecek T, Perret R, et al. (2017) Basal Cell Carcinoma With Matrical Differentiation: Clinicopathologic, Immunohistochemical, and Molecular Biological Study of 22 Cases. Am J Surg Pathol 41(6): 738-749.
-
Kim SH, Lee MG, Kwang GL (2003) Basal Cell Carcinoma with Matrical Differentiation. Yonsei Med J 44(3): 523- 525.
- Epithelioid Granuloma; 3cases with Different Clinical Features
- Advancing Representation in Dermatology Clinical Trials: Ethical, Scientific, and Regulatory Imperatives for Inclusion Across all Fitzpatrick Skin Types
- A Case of Atopic Dermatitis with Concurrent Psoriasis Vulgaris: Successful Treatment with Upadacitinib
- Innovation Lifting Eyeshadow: A Synthesis of Makeup and Optical Illusion
- Distinguishing Superficial Actinic Porokeratosis from Actinic Keratosis with UVF Dermoscopy: A Case Report
- High Mobility Group Box 1 (HMGB1) in Cutaneous Inflammation: An Immune Modulator Bridging Cellular Stress, Ferroptosis and Danger Signaling