Pilomatricoma of the Neck in a Young Boy: An Overlooked Entity
Pilomatricoma is known as one of the benign tumors of the skin appendages. This tumor originates from the matrix cells of the hair follicle. It usually presents as a superficial, firm mass, commonly found in the head and neck region which may pose a diagnostic challenge as it may resemble other common benign lesions such as, sebaceous and epidermoid cysts. Pilomatricoma is best diagnosed by excisional biopsy and histopathological examination. Pathologically, these skin lesions show the presence of basaloid cell islands, eosinophilic cytoplasmic cells without nuclei, as well as haemorrhage and calcification. They typically present as a superficial, firm, solitary, slow-growing mass of the dermis. The overlying skin may exhibit a bluish discoloration or tethering. Treatment consists of surgical excision. Recurrence is rare after complete resection. Malignant pilomatricomas have rarely been reported. We report a case of a young boy with pilomatrixoma of neck, surgical management and histopathological findings.
Introduction
Pilomatricoma is known as one of the benign tumors of the skin appendages. This tumor originates from the matrix cells of the hair follicle and often affects the neck area in young adults and children [1]. The clinical appearance of the lesion is a firm and single subcutaneous nodule, which is usually asymptomatic [2, 3]. The prognosis for this tumoral lesion is good, and it is recommended to completely excise the lesion as the treatment [4].
Pilomatricomas often present as a solitary, hard, slow- growing, subcutaneous mass, and the overlying skin may occasionally have a bluish discolouration. They can occur at any age, although most affect children and young adults. They can present in most hair-bearing parts of the body including the upper and lower extremities and trunk, but they have a predilection for the skin of the head and neck [5, 6, 7]. They are often misdiagnosed, which can result in inappropriate management [8].
In this case report, we present the case of a 13-years- old boy with a large and unusual nodular lesion at the nape of neck noticed 2 years ago. The lesion had been gradually growing over the last one year prior to her visit. We discuss cases of these atypical manifestations of Pilomatricoma.
13-year old boy presented with painful swelling at the nape of neck noticed 2 years ago. The swelling was initially a size of pea, has been gradually increasing in size for the past one year to the current size of nearly a small lemon. It was also associated with pain intensity of which has been increased over the last 2-3 months. There was no accompanying constitutional symptom, history of trauma or any similar complaints in the family. Clinically, he is comfortable and afebrile. Local examination revealed subcutaneous swelling of size measuring 4 × 3 cms, tender, firm, mobile, non- pulsatile, no fixity to the underlying muscles but tethering of the overlying skin was present. The overlying skin was otherwise normal with no change in colour or discharge. There was no other swelling in the head or neck or any other parts of body. Oral cavity examination revealed no pathology. Systemic examination was normal.
The preliminary diagnosis made was sebaceous cyst. FNAC of the swelling was also done that revealed areas of epithelial cell clusters, some showing prominent nucleoli, findings suspicious of cutaneous adnexal tumour. Excision biopsy of mass was done under general anaesthesia.
A yellow-brownish firm mass measuring 4 × 3 cms in subcutaneous plane without any fixity to underlying muscles, was removed taking sufficient margins of healthy surrounding tissues approximately 0.5cm along with an overlying skin and sent for histopathological examination [Figure 1 A-C]. No complication was encountered during or post procedure. Histopathologic findings revealed sheets of basaloid cells undergoing abrupt keratinization, lacking granular cell layer, abundant ghost keratinocytes with foci calcification and foreign body histiocytic giant cell reaction which is consistent with Pilomatricoma [Figure 1D]. He had no evidence of recurrence during his follow-up.
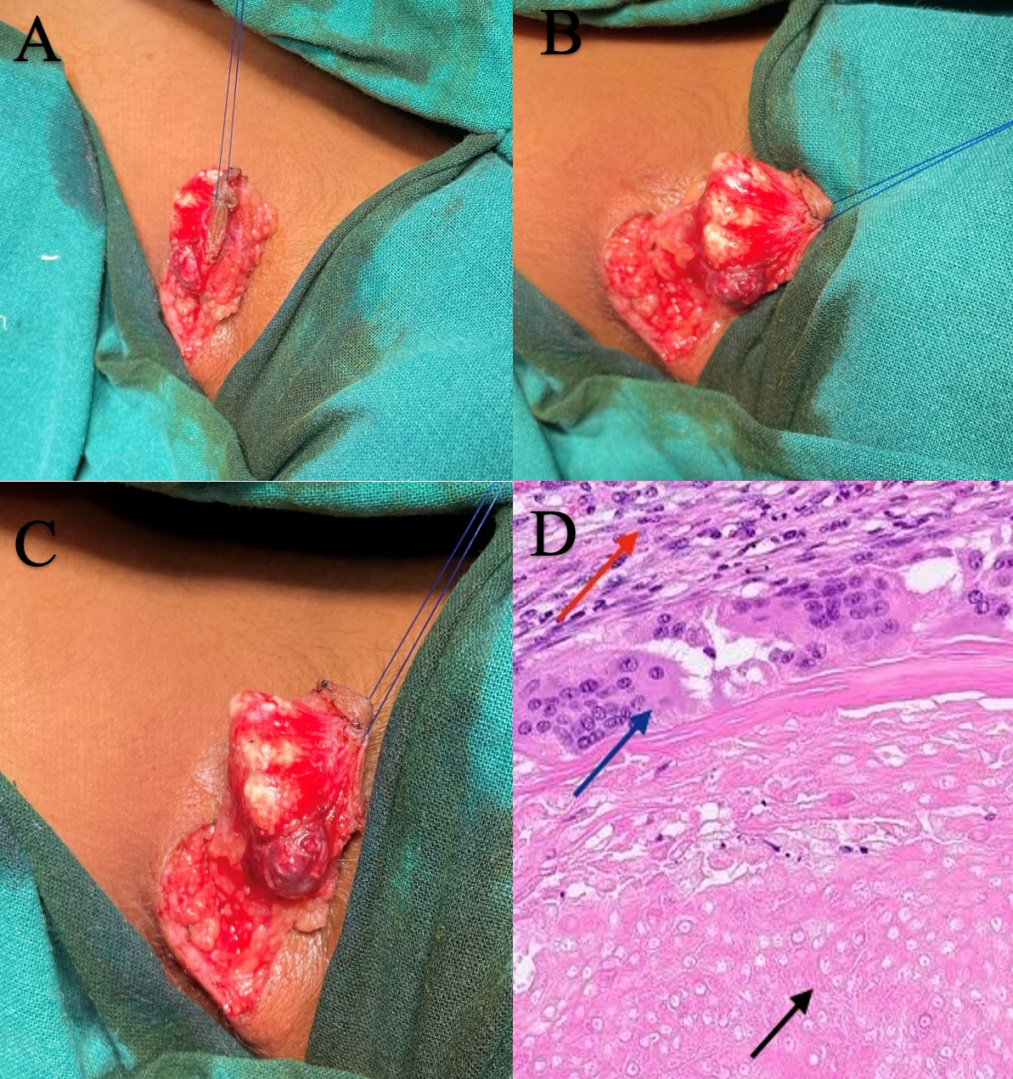
Figure1 A-C: showing firm to hard yellow-brown nodular swelling with calcifications in subcutaneous plane without any fixity to underlying muscle. Skin tethering was also present so it was taken and removed along with the swelling. Figure1D: Histopathological view showing pilomatricoma lesion reveals basaloid cells (blue arrow) and eosinophilic cell structures without nuclei (also known as ghost cells) (black arrow). Red arrow represents stroma of underling tissue.
Discussion
Pilomatricomas often present as a gradually enlarging, asymptomatic, mobile, hard subcutaneous mass [5, 6, 7].
Pilomatrixoma is a rare tumour, accounts for 1.04% of all benign skin lesions [9]. The etiology remains debatable. Dubreuilh and Cazenave proposed two alternative hypothesis [10]. The first hypothesis suggest that the tumour arises from branchial cleft and the second hypothesis proposes the tumour is of ectodermal origin. The fact that pilomatrixoma arises from hair matrix may support the second hypothesis and this may be the etiologic factor of our patient.
Pilomatricomas are frequently misdiagnosed with two common entities viz. sebaceous (35%) and epidermoid (19%) cysts, which can be explained by the fact that these lesions are much more common and can have a similar appearance. Epidermoid (sebaceous) cysts are often spherical and firm, are attached to the overlying skin, and have a punctum, whereas pilomatricomas often present as a subcutaneous mass with a hard nodular surface, and are freely mobile from the underlying tissues, although the skin attachment can occasionally be mistaken for a punctum as similar finding in our case report. The “tent sign”, where stretching the skin over the mass to allow the nodular surface to become apparent, can help narrow the diagnosis [11]. Although pilomatricomas occur over a wide age range they often present in children, whereas epidermoid cysts are not common in this prepubertal age group.
Less than 30% of cases were reported to be diagnosed preoperatively [5]. Pilomatricoma is best diagnosed by excisional biopsy and histopathological examination, as fine needle aspirate may be misleading if ghost cells are not aspirated [12]. Findings including sheets of basaloid cells undergoing abrupt keratinization, lacking granular cell layer, abundant ghost keratinocytes with foci calcification and foreign body histiocytic giant cell reaction are consistent with pilomatricoma but presence of ghost cells are highly characteristic in diagnosing this entity. As for radiologic imaging, it carries little diagnostic value as to differentiate pilomatrixoma from other subcutaneous tumour. Malignant transformation (pilomatrix carcinoma) is very rare, and fewer than 100 cases reported worldwide. It is most common in the head and neck and has a male predominance and a predilection for the elderly [13].
Management for pilomatrixoma is complete excision including an excision of overlying skin if adherence is observed. As for the malignant variant, wide excision is proposed to prevent recurrence. Post-operative recurrence has been reported between 2 and 6% [14]. As for our patient, no recurrence is noted during her 6 months follow-up.
Conclusion
Pilomatricoma is one of the benign tumors of the skin appendages and frequently confused with other common entities viz. sebaceous (35%) and epidermoid (19%) cysts. So, clinicians should be aware of this entity as to avoid unnecessary radiologic imaging and procedure. Fine needle aspiration is often considered as part of the diagnostic investigation of a mass in the head and neck. The presence of ghost cells and basaloid cells on fine needle aspiration from a subcutaneous mass is considered enough to diagnose pilomatricoma but many times ghost cells are not aspirated and it may be misleading. Pilomatricoma is best diagnosed by excisional biopsy and histopathological examination. Malignant transformation to a pilomatrix carcinoma should be suspected in cases with repeated local recurrences.
Author Contribution Details
N Jain was involved in the diagnosis and management of the patient as well as responsible for reviewing, editing, and finalising the manuscript.
Conflict of Interest
The Authors declare that there is no conflict of interest.
Funding/Financial Disclosure
No financial support was received for the research, authorship and/or publication of this article.
References
-
Inagaki A, Yamashita Y, Mori Y, Takeuchi E, Asaoka K, et al. (2019) An unusual tumor of the ear pilomatricoma in a middle-aged woman. Case Rep Otolaryngol 18(4): 34-40.
-
Shetty AS, Kishan P, Asnani R (2022) Giant sternal Pilomatricoma an unusual tumor at an uncommon site. J Health Allied Sci NU 13: 440-442.
-
Bouabdella S, Khouna A, Dikhaye S, Zizi N (2022) Isolated pilomatricoma of the arm: a case and a review of the literature. Our Dermatology Online/Nasza Dermatologia Online 13(1): 86-88.
-
Sun J, Fu LB, Xu JS, Han XF, Wei L (2023) Confused subcutaneous nodules in children: differential diagnosis of pilomatricoma in children. J Cosmet Dermatol 22(12): 3413-3417.
-
Julian CG, Bowers PW (1998) A clinical review of 209 pilomatricomas. J Am Acad Dermatol 39: 191-195.
-
Pirouzmanesh A, Reinisch JF, Gomez I, Smith EM, Meara JG (2003)Pilomatrixoma: a review of 346 cases. Plast Reconstr Surg 112(7): 1784-1789.
-
Danielson A, Lin SJ, Hughes CA, An YH, Maddalozzo J (2001)Head and neck pilomatrixoma in children. Arch Otolaryngol Head Neck Surg 127(12): 1481-1483.
-
Kumaran N, Azmy A, Carachi R, Raine PA, Macfarlane JH, et al. (2006) Pilomatrixoma accuracy of clinical diagnosis. J Pediatr Surg 41(10): 1755-1758.
-
Guinot MR, Valmaseda CE, Berini AL, Gay EC (2010) Pilomatrixoma review of 205 cases. Medicina Oral Patologia Oral y Cirugia Bucal 16(4): 552-555.
-
Dubreuilh W, Cazenave E (1922) De l’epithelioma calcifie etude histologique. Ann Dermatol Syphilol 3: 257-268.
-
Graham JL, Merwin CF (1978) The tent sign of pilomatricoma. Cutis 22(5): 577-580.
-
Pant I, Joshi SC, Kaur G, Kumar G (2010) Pilomatricoma as a diagnostic pitfall in clinical practice: report of two cases and review of literature. Indian J Dermatol 55(4): 390-392.
-
Hardisson D, Linares MD, Cuevas SJ, Contreras F (2001) Pilomatrix carcinoma a clinicopathologic study of six cases and review of the literature. Am J Dermatopathol 23: 394-401.
-
Guinot MR, Valmaseda CE, Berini AL, Gay EC (2010) Pilomatrixoma review of 205 cases. Med Oral Patol Oral Cir Bucal 16(4): 552-555.
- Epithelioid Granuloma; 3cases with Different Clinical Features
- Advancing Representation in Dermatology Clinical Trials: Ethical, Scientific, and Regulatory Imperatives for Inclusion Across all Fitzpatrick Skin Types
- A Case of Atopic Dermatitis with Concurrent Psoriasis Vulgaris: Successful Treatment with Upadacitinib
- Innovation Lifting Eyeshadow: A Synthesis of Makeup and Optical Illusion
- Distinguishing Superficial Actinic Porokeratosis from Actinic Keratosis with UVF Dermoscopy: A Case Report
- High Mobility Group Box 1 (HMGB1) in Cutaneous Inflammation: An Immune Modulator Bridging Cellular Stress, Ferroptosis and Danger Signaling