Diastolic Learning: Making the Tacit, Explicit
Introduction: Surgery is a motor skill that has to be learnt through practice. The acquisition of motor skills and the principles are well documented especially in sport. Deliberate practice is the engagement in structured activities created specifically to improve performance in a domain and requires feedback. The experience needed to become an expert can be helped in the early stages of training with deliberate practice and observation by a skilled trainer. The aim of this project is to establish whether a combination of low fidelity simulation models and deliberate practice can reliably predict achievement of basic surgical skills competency. Video based scoring was used to quantify progress.</p> <p>Methods: We recruited thirty junior doctors and medical students with minimal exposure to surgery. They were provided with appropriate instruments and materials. They were given a demonstration of low fidelity simulation models, principles of needle handling and feedback on their first attempts. An initial video was taken. Subsequently they were given specific exercises to practice at home. They were reassessed after a period of one week and a second video was taken. <p>Results: The participants were scored on four parameters: Time/pace, flow/rhythm, precision, rotation. There was significant improvement on all four parameters in twenty-eight out of thirty participants. This ranged from 18.9% (time) to 40% (flow).</p> <p>Conclusion: This project has enhanced our knowledge and practice in surgical education and training.Our work provides evidence on how low-fidelity simulation models can reliably be used to achieve significant progress through early stages of the learning curve. Furthermore it demonstrates the principles that need to be observed in order for deliberate practice to be effective and efficient in acquisition of surgical skills.
Background
Surgery is a motor skill that has to be learnt through practice. The acquisition of motor skills and the principles are well documented especially in sport. The theory and practice of coaching all athletes at every level involves an understanding of the fundamentals of movement and ergonomics. In the current era, surgical training has evolved in order to conform with certain conditions: The European Working Time Directive (shorter workweek for residents), increasing complexity of cases and emphasis on operating room efficiency as well as mitigating medical error constitute limitations in the preparation of trainees for the operating room experience. Simulation techniques are based on established theories on motor skill acquisition and development of expertise [1]. Fitts and Posner’s three-stage theory is widely accepted [2]. Many consultants of today learnt their skills by volume, by ‘practicing’ on patients. Basic Surgical Skills were acquired and rarely taught. Many a trainer, when asked how they executed a specific task will not be able to deconstruct the actions into set up, posture, instrument handling, angles etc. They will when it is explained i.e. the tacit is made explicit. The handling of instruments and the passage of the needle through the tissue can be explained in a similar way – this theory has been published and the success of this teaching is realised over sixteen years delivering critically acclaimed courses – PAR Excellence and PAR Aorta courses. The feedback from trainees includes “I wish I was taught this earlier!” and “why hasn’t anyone explained this to me before!” Most models suggest that the earlier stages should take place outside the operating room. Fidelity may be less important at relatively junior levels of training. Initial acquisition of skills require block practice i.e. repetition. This can be done at home on low fidelity models that offer visible and tactile feedback [3]. Deliberate practice is the engagement in structured activities created specifically to improve performance in a domain and requires feedback. Are experts ‘born’ or ‘made’? This is a highly controversial issue. The 10 000 hours needed to become an expert can be helped in the early stages of training with deliberate practice and observation by a skilled trainer. The aim of this project is to establish whether a combination of low fidelity simulation models and deliberate practice can reliably predict achievement of basic surgical skills competency. The tasks were recorded and videos were reviewed and scored by the assessors.
The Concept of ‘Diastolic Learning’
The cardiac cycle consists of two distinct time periods: Systole (contraction of myocardium) and diastole (relaxation of myocardium). Systole is a fixed and relatively short time period whereas diastole is longer and varies in length of time depending on haemodynamic conditions. We propose that the surgical skill of suturing any structure (ie. vein, artery, skin, subcutaneous tissue) can also be divided in two distinct time periods: The passing of the needle through the structure (systole) and the setting up of the needle on the needle holder in preparation for the next pass (diastole). The above parallelism is elaborated below: The time it takes an expert surgeon and a trainee to deliver a needle through the tissue is the same for a single pass “systole”– but the difference between the expert and the trainees becomes obvious when examining the time it takes to set up to take the second stitch “diastole”. The diastolic time is reliant on the ergonomics of the setup, posture, positioning and handling of the instruments – these skills are tacit for the expert surgeon and have been honed by volume and time. For the trainee, this aspect can be explained and taught. Have you ever wondered why a good operation appears as smooth; it is because the diastolic period is minimized and the surgeon makes it look easy because they have attended to the setup, their posture, address to the table and angles i.e. all the negative-passive behaviours. These are sometimes poorly explained, taught or realised by the trainee or trainer alike but can be understood and more importantly practiced and rehearsed on low fidelity systems at home.
Methods
Recruitment and Demonstration
Over a period of nine months (Oct 2016 – June 2017) we recruited thirty junior doctors (rotating through cardiothoracic surgery at the Royal Infirmary Edinburgh) and medical students (University of Edinburgh Medical School) with minimal or no previous exposure to surgery. We purchased an ironing board (operating table), Castro-Viejo needle holders, 5-0 and 6-0 prolene sutures, aortic punches and bananas. On a one-to-one basis we explained to each participant the concept of diastolic learning. We demonstrated the basic principles of needle- mounting on needle holder, needle-handling, delivering (clean rotation) through tissue with minimal injury, pick- up of needle at specific angles to facilitate next pass. We encouraged them to use dominant hand only (ie. non- dominant hand was kept behind back during execution of task so it did not play any role). Needle rotation through the tissue is evident by how cleanly the needle enters and exits the tissue (banana skin) without tearing. The banana skin tears and blackens giving visible feedback of needle holes - 'skids' are clearly seen as linear tears.
The Task and Deliberate Practice
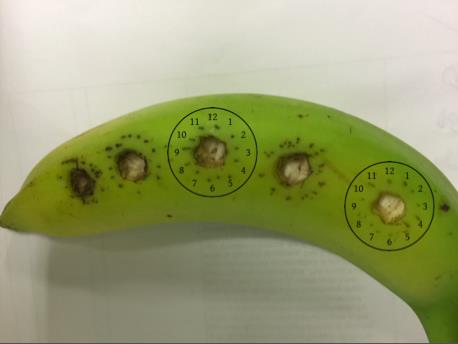
We made five 0.5 -1cm diameter holes on the banana skin. We advised participants to visualise the hole in the banana as a 12hour clock (pictures). We instructed them to try and hit every hour, on the hour, (1 through 12) with their needle rotating cleanly through the hole. Each participant had 4 attempts to complete the task with the supervisor providing feedback and correcting/adjusting hand motions, instrument handling, posture, table height etc. The fifth attempt was performed independently by the participant (ie. no feedback was provided by supervisor) and was video recorded. The participant was given a set of instruments and materials to practice the learned task on the banana at home, in their own time, for the next six days. They were advised to spend 30mins per day. A second video was taken of their post six-days-of- deliberate-practice attempt. The two videos were compared.
Parameters Measured
Time / pace: The average time taken to complete the task. Flow / rhythm of motion: Number of times that participant had to use non-dominant hand to re-adjust the needle on needle-holder after first pass through banana skin. Precision: How many of the 12 hours were hit accurately: Needle holes equidistant from each other and from the edge of banana hole. (1-12 points). Rotation: How cleanly was the needle delivered through banana skin (distinct holes vs slits) (1-12 points).

Results
Twenty eight out of thirty participants demonstrated improvement in all four variables. On average the time needed to complete the task on first attempt was 4:46 mins (range 3:41 – 5:30mins) and on second attempt 3:24 mins (range 2:00 – 4:00mins). The improvement in task completion time was 28.6%. The flow / rhythm parameter was improved 40% and this is obvious on watching attempts 1 and 2 of each participant. There is a clear difference in the needle handling, pick-up and delivery. This improvement can be described as more deliberate and planned movements with significant reduction of hesitation, deviation, interruption and repetition.
- Precision showed an improvement of two points (on average) on the twelve point scale. Participants were scored 8/12 for their first attempt (range 7/12 – 10/12) and 10/12 for their second attempt (range 9/12 – 11/12). st nd
- N=30
- 1
- Attempt
- Improvement
- Time mean, (range)
- 4:46 (3:41 – 5:30)
- 3:24 (2:03 – 4:18)
- 1mn22sec (28.6%)
- Attempt
- 2
- Flow median (range)
- 5
- (1 – 8)
- 3 (1 – 5)
- 2 (40%)
- Precision median, (range)
- 8/12
- (7/12 – 10/12)
- Rotation median, (range)
- 7/12
- (6/12 – 9/12)
Table 1: Improvement of two points (on average) on the twelve point scale.
Discussion
The practice of surgery like all sports requires the application of the same principles. It is important to deconstruct the movements and explain ergonomics required to achieve the action. It is this understanding and rehearsal of these movements that will cultivate and reinforce a motor memory resulting in a reduction in the diastolic time of an operation and a smooth transition between actions. These simple principles have been employed in the instruction of the martial arts for thousands of years. The power and flow is achieved with an attention to the practice of the deconstructed movements; the first skill is to master correctness. Most skills workshops have trainees seated (picture here) on fixed chairs operating at tables – this is not optimising the functional anatomy of the upper limb and cannot be further from the movements and understanding of the ergonomics required to effect a smooth action at the operating table where we are standing. Those disciplines that do sit to operate undoubtedly have a stool that is on wheels and goes up and down. The stool can move through three dimensions. It is not fixed. We are training our surgeons incorrectly. Moreover, we do not offer a framework of understanding or provide models for deliberate practice. There is a very attractive meritocratic and egalitarian attribute to Ericsson’s view that everyone can attain expert level of performance with enough hard work, coaching and feedback. Antagonists have commented that the deliberate practice theory requires ‘a blindness to ordinary experience’ and to the fact that most people who want to become experts – in music, sports or other domains- do not make it [4]. Furthermore, literature provides support for Ericson’s contention that many professionals probably never attain true expertise [1]. A recent meta-analysis concluded that the volume of deliberate practice – although unquestionably important as a predictor of individual differences in performance - is not as important as Ericsson and colleagues have argued. In fact it could only explain up to thirty percent of the variance [5]. Currently, two types of operative skills assessment are in use: Rating scales and motion analysis. In this work we used rating scales as despite our research we were not able to identify the software required for reliable video interpretation and scoring. However, there are no defined relevant, robust measures of outcome that can be directly attributed to the effects of training. Therefore correlating assessment with future performance is difficult. Furthermore, as reliability and validity of assessment tools is increasing it is likely that competence-based advancement, rather than time served, will become standard in surgical training [1]. William Halsted, when he introduced the residency training system which remains the cornerstone of surgical training more than a century later, also supported competence-based advancement.
Limitations
In our opinion this project (supported by our experience with the PAR courses over last ten years) provides compelling evidence that basic surgical skills can reliably be taught and learned using low fidelity models and deliberate practice.
Three of the parameters measured (flow/rhythm, precision and rotation) are qualitative and subjective by definition. However, time/pace, which was the only objectively quantifiable parameter, showed an impressive 30% improvement. Furthermore participants reported their average practice times but they were not directly observed. In our experience character traits such as persistence and motivation play a role on how much time a trainee spends practicing and this has direct implications on their ability to perform the task.
Conclusion
This project has enhanced our knowledge and practice in surgical education and training both from trainee and trainer perspectives. Our work provides evidence on how low-fidelity simulation models can reliably be used to achieve significant progress through early stages of the learning curve. Furthermore it demonstrates the principles that need to be observed in order for deliberate practice to be effective and efficient in acquisition of surgical skills. Accurate assessment of an individual’s abilities at an early stage may be critical in their choice of career and whether they have a realistic chance of becoming an expert through deliberate practice. The usefulness of any particular assessment method is determined by its reliability, validity, impact on future learning and practice, acceptability to learners-faculty, and costs [6].
The next step in this project is to use video based motion analysis in order to objectively quantify the measured parameters. Our aim is to provide insight into how assessment methods can be optimized in terms of validity, reproducibility and cost-efficiency.
References
-
Reznick RK, MacRae H (2006) Teaching surgical skills-changes in the wind. N Engl J Med 355(25): 2664-2669.
-
Fitts PM, Posner MI (1967) Human performance. CA: Brooks/Cole, Belmont.
-
Papaspyros SC, Kar A, O’Regan D (2015) Surgical ergonomics. Analysis of technical skills, simulation models and assessment methods. Int J Surg 18: 83-87.
-
Hambrick DZ, Oswald FL, Altmann EM, Meinz EJ, Gobet F, et al. (2014) Deliberate practice: Is that all it takes to become an expert? Intelligence 45: 34-45.
-
Macnamara BN, Hambrick DZ, Oswald FL (2014) Deliberate practice and performance in music games sports education and professions: A meta analysis. Psychol Sci 25(8): 1608-1618.
-
Van der Vleuten CPM (1996) The assessment of professional competence: developments, research and practical implications. Adv Health Sci Educ 1(1): 41-67.
- The Expanding Landscape of Road Rage: A Systematic Review of Conflicts Involving Drivers, Pedestrians, and Micromobility
- Validating Cognitive Models of Royal Navy Performance on Control Systems
- Comparing Standard and State-of-the-art Firefighter Coats on Postural Balance and Gait in a Live Burn Environment
- Investigating the Integration of Telemedicine into Clinicians Workflow: A Review of Methods
- Risk Assessment of Ergonomic Factors in a Textile Firm by RULA, REBA and Fine Kinney Methods
- Impact of Self-Esteem Training on Individuals with Disabilities Aged 17-30