Investigating the Integration of Telemedicine into Clinicians Workflow: A Review of Methods
Telemedicine has received recent attention as a means to improve care access for chronically ill patients and underserved communities. However, new health information technologies like telemedicine change health providers’ practices, management, and environment. These changes, if not well addressed, can cause dissatisfaction and disruption, negatively impacting time efficiency, quality of care, and patient safety. This scoping literature review seeks to identify the methods used to study integration of telemedicine into clinicians’ workflow. Scoping reviews identify gaps and provide direction for future research and areas of improvement. Peer-reviewed, original empirical studies related to workflow in the context of telemedicine integration were identified through a comprehensive search of MEDLINE (Ovid). The search identified 147 articles, which were screened based on title and abstract. The remaining articles were thoroughly reviewed and assessed for eligibility. Fifteen articles were included. Three approaches to study telemedicine integration in clinical workflow predominate the academic literature: First, quantitative data analysis techniques applied to time studies, time-motion studies, and surveys and interviews; second, qualitative data analysis techniques applied to interviews, surveys, and observational studies; and third, mixed methods to assess telehealth integration. Literature identifies time-saving as a significant benefit of telemedicine. However, physicians, nurses and other relevant stakeholders have concerns that cannot necessarily be measured in terms of time. Additional research is needed to address other dimensions of clinical workflow, collect holistic perspectives of integration issues from stakeholders, and connect those issues to the specific components of the telemedicine system to prioritize in process improvement.
Introduction
Integration of health information technologies (HIT) has provided valuable benefits in healthcare management and access. For example, HIT has allowed physicians to track patients’ health information on demand via electronic health records (EHRs) [1] and patients’ health status remotely (e.g. telemedicine) [2], providing quality, efficiency, and cost-reduction benefits [3]. Telemedicine which involves providing patient care remotely has received special attention in recent years for improving healthcare access [4], as well as for supporting integrated care for chronic diseases by providing patient education and information transfer between patients and providers, and by improving EHRs [5]. Telemedicine has been formally defined in various ways based on medical, technological, spatial, and beneficial aspects [6], but the Health Resources and Services Administration (HRSA) defines telemedicine as “the use of electronic information and telecommunications technologies to support and promote long-distance clinical health care, patient, and professional health-related education, public health and health administration [7].” Despite the benefits of telemedicine, development and implementation of telemedicine technologies has shown challenges in terms of cost, acceptance, usability, and effectiveness.
One of the most important challenges for implementation of new telemedicine technologies, is the change in health providers’ workflow. For the purposes of this research, ‘workflow’ refers to the sequence of tasks (mental or physical) performed by people in their work environment. Understanding the impact of telemedicine integration on clinician workflow is vital for long-term success and adoption of these technologies. Such impacts, if not well understood and addressed, may lead to provider dissatisfaction and workflow disruptions, impacting efficiency, quality of care, and patient safety [8, 9]. It is known that increased workload as a result of telemedicine integration could result in low to no adoption of the technology by clinicians [10]. Despite the recent growth of telemedicine platforms, no review exists to document and synthesize the learning from recent integration of telemedicine focusing on methods for investigating the effects on clinicians’ workflow. To address this gap, we conducted a review of literature to identify the scope of work done as well as methods and approaches that have been applied to study integration of telemedicine into clinicians’ workflow, with the ultimate goal of developing methods to improve telemedicine integration into healthcare clinical environments.
Method
Published literature about the study of the integration of telemedicine into clinician’s workflow was identified through a comprehensive double search of the MEDLINE (Ovid) database (Table 1) conducted in February of 2018, and reviewed in January of 2019. Search terms such as “telemedicine”, “mobile applications”, “patient portals”, “remote consultation”, “remote monitoring”, “remote sensing technologies”, “physicians”, “doctors”, “nurses”, and “workflow” were used to capture articles that mainly apply qualitative and quantitative methods to study the impact of telemedicine integration in clinicians’ workload or to develop models for telemedicine integration into healthcare settings from the clinicians’ perspective. Only English-language, peer-reviewed journal publications with original empirical evidence were included with no date restriction; review articles and non-empirical essays were excluded.
| MEDLINE (Ovid) | |
|---|---|
| 1. exp TELEMEDICINE/ | 1. exp TELEMEDICINE/ or exp Remote Consultation/ or exp Monitoring, Physiologic/ or exp Remote Sensing Technology/ or exp Mobile Applications/ |
| 2. exp Mobile Applications/ | 2. (remote adj2 (monitor* or consult* or sensing)).ti,ab. |
| 3. exp Patient Portals/ | 3. exp Patient Portals/ |
| 4. (telemedicine or (mobile adj2 app*) or (patient adj1 portal*)).ti,ab. | 4. (telemedicine or (mobile adj2 app*) or (patient adj1 portal*)).ti,ab. |
| 5. or/1-4 | 5. or/1-4 |
| 6. exp PHYSICIANS/ | 6. exp PHYSICIANS/ or exp NURSES/ |
| 7. (physician* or doctor*).ti,ab. | 7. (physician* or doctor* or nurses or nurse or clinician*).ti,ab. |
| 8. 6 or 7 | 8. 6 or 7 |
| 9. exp WORKFLOW/ | 9. exp WORKFLOW/ |
| 10. workflow.ti,ab. | 10. workflow.ti,ab. |
| 11. 9 or 10 | 11. 9 or 10 |
| 12. 5 and 8 and 11 | 12. 5 and 8 and 11 |
Table 1: Search Criteria.
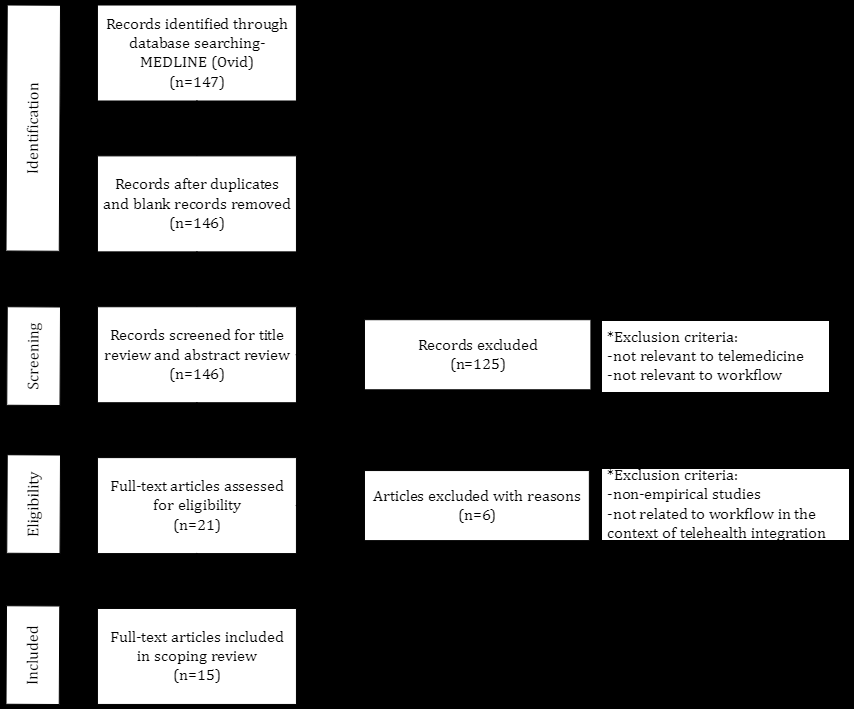
The initial search identified 147 articles, from which only 146 were considered for the inclusion process after deleting one duplicate publication. The included articles were selected using a 2-step inclusion process. In the first step, the articles were screened based on their title and abstract. There were 125 articles excluded in this step because they were not relevant to telemedicine or workflow analysis. The remaining 21 articles were thoroughly reviewed and assessed for eligibility. Eligibility criteria included: (1) articles with original empirical studies and (2) related to workflow in the context of telemedicine integration. The second step excluded six articles. Finally, 15 peer-reviewed journal articles were included in the scoping literature review. See Figure 1, modified from the PRISMA-ScR [11] guidelines for reporting scoping reviews, for a process summary.
| Variable | Description & Assumptions |
|---|---|
| Year | Year the research study was published. |
| Healthcare Setting | Type of clinical environment where the study was held. The data was collected inductively and then classified in three major categories: |
| (1) PCP/Clinic | |
| (2) Hospital/ER | |
| (3) Telemonitoring Research Program | |
| Type of Health Provider | Qualified healthcare professional that served as subjects for the studies. |
| Medical Condition | Diseases or medical disorder of the patient population for which telemedicine was being used or tested to provide healthcare services in the study. |
| Telemedicine Modality* | Particular type of telemedicine system being used in the study. Classified based on the four major types of telemedicine modalities: |
| (1) RPM | |
| (2) Store-and-forward | |
| (3) Real time live video | |
| (4) mHealth | |
| Abbreviations: ER (Emergency Room); PCP (Primary Care Physician); RPM (Remote Patient Monitoring); mHealth (mobile Health) | |
| *While telehealth is now more commonly used to describe the wide range of health services provided using technology, telemedicine is often used to make reference to the delivery of clinical diagnosis and monitoring using technology [12]. |
Table 2: Description of the variables for which data were sought.
The scoping literature review was conducted by a single reviewer. The reviewer extracted five aspects of the studies, established a priori. For each article included, the reviewer identified the following variables (established and defined in Table 2): (1) year, (2) healthcare setting, (3) type of healthcare provider, (4) medical condition, and (5) telemedicine modality. Additionally, the reviewer documented the methods used and the major findings from each of the articles.
Results
Findings have been divided into two sections. The first section presents the results from a descriptive analysis that was conducted for the variables of interest for the included articles (Table 3). The second section summarizes the methods and approaches that have been applied in the included articles to study the integration of telemedicine technologies into clinicians’ workflow.
| Author | Year | Healthcare Setting | Type of Healthcare Provider | Medical Condition | Telemedicine Modality |
|---|---|---|---|---|---|
| Tang, et al. [13] | 2007 | Hospital/ER | Physician Nurse | ICU Patients | RPM |
| Kaufman, et al. [14] | 2009 | Hospital/ER | Nurse | Diabetes | Real-time live video |
| Cady, et al. [15] | 2010 | Telemonitoring Research Program | Nurse | Lung Problems | RPM |
| Fish, et al. [16] | 2011 | PCP/Clinic | Physician | Diabetes Ophthalmology | Store-and-forward |
| Cronin, et al. [17] | 2012 | PCP/Clinic | Nurse | Heart Conditions | RPM |
| Armstrong, et al. [18] | 2012 | PCP/Clinic | Physician | Dermatology | Store-and-forward |
| Cady & Finkelstein [19] | 2012 | PCP/Clinic | Nurse | Complex Pediatric Conditions | Real-time live video |
| Koopman, et al. [20] | 2013 | PCP/Clinic | Physician Nurse | Diabetes | RPM |
| Shaw, et al. [21] | 2013 | PCP/Clinic | Physician Nurse | Blood Pressure | Real-time live video |
| Cady & Finkelstein [22] | 2013 | PCP Clinic | Nurse | Complex Pediatric Conditions | Real-time live video |
| Uscher-Pines & Kahn [23] | 2014 | Hospital/ER | Physician | Complex Pediatric Conditions | Real-time live video |
| Cady & Finkelstein [24] | 2014 | PCP/Clinic | Nurse | Complex Pediatric Conditions | Real-time live video |
| Ricci, et al. [25] | 2014 | PCP/Clinic | Physician Nurse | Heart Conditions | RPM |
| Facchin, et al. [26] | 2016 | PCP/Clinic | Physician Nurse | Heart Conditions | RPM |
| Yen, et al. [27] | 2016 | PCP/Clinic | Physician Nurse | Arthritis | mHealth |
| Abbreviations: ER (Emergency Room); ICU (Intensive Care Unit); PCP (Primary Care Physician); RPM (Remote Patient Monitoring); mHealth (mobile Health). |
Table 3: Peer-reviewed articles included in the scoping review.
Descriptive Analysis
The included literature was published after 2007. Thus, although telemedicine has been a topic in the last 20-30 years, specific study of workflow integration is relatively new and sparse. The few empirical studies published have mostly used primary care clinics and specialty care centers as their main research setting. Both physicians and nurses have been the main subjects of study. Workflow involving telemedicine has three distinctive aspects: (1) technology-mediated intervention, (2) centrality of the tele-mediated encounter with the patient, and (3) novelty of the paradigm, with a less prescribed workflow leading to variation in practice [14].
Technology-mediated intervention depends on the type of telemedicine modality being used. Real-time live video implies the use of audiovisual telecommunications technology to allow two-way interaction between the health provider and the patient, caregiver, or another provider [12]. Store-and-forward uses secure electronic communications systems to transmit recorded health history between practitioners who then evaluate the case or provide service outside the real-time modality [12]. In remote patient monitoring (RPM), patient health and medical data are transmitted to the provider using electronic communication technologies [12]. Mobile health (mHealth), on the other hand, refers to the use of mobile communication devices to provide health care and public health practice and education [12]. Out of the four modalities, real-time live video and RPM have received significant emphasis in this literature. However, some work has been published regarding the mHealth and store-and-forward (Table 3). Applications of telemedicine can be found for multiple diseases and medical conditions. In the context of the impact in clinicians’ workflow, studies have involved telemedicine technologies for the consultation and monitoring of patients with arthritis, dermatology conditions, ophthalmology conditions, lung conditions, but more commonly for diabetes, hypertension, cardiac problems, and specific pediatric conditions. Finally, the most common setting in which the impact of telemedicine on workflows were studied was primary care physician offices and clinics.
Methods and Approaches to Study Integration of Telemedicine into Clinicians’ Workflow
There are variations in the data analysis methods used to study the impact of technology integration. Some studies use quantitative data analysis, such as descriptive statistics, to analyze the data obtained from time studies, time-motion studies, and surveys and interviews. Others use qualitative data analysis techniques to analyze interviews, surveys, and observational data. Several studies used mixed methods including both quantitative and qualitative methods.
Quantitative Methods and Approaches: Quantitative approaches to data collection have focused on time as their primary measure, by various means. The time study methods emerged as part of the “scientific management” field and consider the time required to accomplish specific tasks [28]. For telemedicine workflow integration, time studies have been conducted mostly to analyze the impact on time it takes the physicians to monitor RPM patients with cardiac implantable electronic devices compared to non- telemedicine workflows. Descriptive statistics have been used to report measures of interest regarding the impact on physician’s workflow, such as: (1) number and frequency of scheduled and unscheduled transmissions [17, 26], (2) number and frequency of actionable events requiring physician notification [17], and (3) average processing time for evaluation and review by physicians or nurses [17, 25]. Results from these studies revealed that processing remote transmissions were faster when compared with in-person evaluations [17]. Additionally, it was identified that an RPM approach (specifically for remote follow-up of cardiac implantable devices) requires less workforce, representing a gain in time and resources in comparison with in-hospital follow-ups [25]. However, these studies only consider impacts in one dimension of the workflow-time.
Time motion studies not only consider time but also analyze the set of tasks within the activities the clinicians have to perform [28]. This approach identifies and categorizes relevant tasks to establish: (1) the frequency and time spent on each task [13, 14, 15, 22, 24, 27], (2) frequency and duration of interruptions during the telemonitoring encounters [13], (3) frequency of information resource use during the telemonitoring encounters [13, 15, 22, 24], (4) comparison between the total time spent on a patient visit before and after telemonitoring system implementation [27], (5) impact of activities added to the workflow by telemonitoring system integration [24], and (6) comparison between different telemonitoring encounters, such as initial, routine, and complex encounters [14]. Descriptive statistics quantify each of the measures mentioned above. Even with this more activity-based depth, however, time motion studies still do not encompass relevant qualitative factors at the people, environmental, technological, and organizational levels [29].
Less frequently, descriptive statistics have also been used to analyze results from physicians’ interviews. Armstrong, et al. [18] used this approach to identify and quantify: (1) the factors that influence PCPs to refer patients to tele-dermatology programs, (2) the challenging aspects of participating in a tele-dermatology referral program (workflow disruption was mentioned by the interviewees), and (3) opportunities for operational improvement in the referral program.
Qualitative Methods and Approaches
Qualitative data collection methods include observational studies, sometimes complemented by audio- visual recording [14], to: (1) capture activities performed by the subjects before, during, and after a telemedicine encounter [14], (2) identify issues encountered when interacting with the telemedicine system [14, 16, 22, 25], and (3) identify the communication and interaction that the subjects have with other resources [14, 22, 24]. The think- aloud verbal protocol has also been used to understand the subject’s thought process while performing activities related to the telemedicine system [27]. Semi-structured interviews and surveys have been highly used to collect information about: (1) workflow patterns [14, 20, 22, 24], (2) interaction with the resources and artifacts used [14, 22, 24], (3) problems and challenges encountered [14, 16, 18, 20, 23], and (4) barriers and facilitators for organizational readiness [21]. In the case of mHealth, usability evaluations have been performed to identify issues when physicians interact with mobile applications [27].
Researchers have used grounded theory [30] and qualitative data analysis (QDA) methods with the purpose of identifying relevant patterns and themes in data obtained from observation, interviews, and surveys. Uscher-Pines & Kahn [23] incorporated both themes from the literature as well as new themes that emerged from the analysis, to interpret results from a physician survey regarding the use of pediatric telemedicine in underserved areas of the United States [23]. The authors developed a hierarchical organized codebook [31] and identified significant barriers to the successful use and implementation of telemonitoring systems in pediatric emergency settings, including: (1) integration of the technology into established workflows, (2) usability of the technology, (3) lack of physician buy-in, (4) misaligned incentives, and (5) lack of reimbursement. Similarly, Koopman, et al. [20] used grounded theory to analyze interviews of nurses and physicians regarding the implementation of a home blood glucose and blood pressure telemonitoring system in primary care practices. Results from their QDA overlap with the findings of Uscher-Pines & Kahn [23]. The physicians and nurses presented concerns regarding (1) the impact on workflow, (2) extra work required due to non-integration between the telemedicine system and the EHR, (3) usability of the system and the display design, (4) effectiveness and return on investment, and (4) misaligned incentives for providers. Fish, et al. [16] used open coding to analyze the results of semi-structured interviews of ophthalmologists regarding their experiences using store-and-forward telemedicine. Themes included (1) the need to develop efficient workflow protocols to avoid unbalanced workload, (2) change in the relationship between physicians when managing a patient, and (3) the perceived possibility of malpractice and potential impact on physician’s adoption of telemedicine.
Shaw, et al. [21] used conventional content analysis to analyze qualitative interview and survey data from nurses, physicians, administrators, and information technology professionals regarding organizational factors associated with readiness to implement a primary care- based telemedicine behavioral program for blood pressure control. The authors used the Weiner Organizational Theory of Implementation Effectiveness [32] to categorize their findings. Results from the analysis revealed that the stakeholders expressed concerns related to (1) the length of implementation time (which affects their buy-in of the telemedicine system), (2) the availability of staffing time to dedicate to the telemedicine intervention, and (3) the possibility that the telemedicine intervention could compete with other existing telemedicine and home service programs.
Mixed Methods and Approaches: Other researchers have integrated both qualitative and quantitative data collection approaches. Primarily, those researchers have complemented time-on-task and time-motion studies with the integration of observation and interviews with relevant stakeholders involved in the process [14, 19, 22, 24]. Work related to real-time video-conference telemedicine can be analyzed in three dimensions: (1) system resources, (2) flow of communication, and (3) time on task [14]. This three- dimensional workflow analysis involved complementing the time on task statistical analysis with a qualitative analysis of system resources and a communication flow analysis to represent coordination over time across the different agents involved in the process, including the communication modalities (e.g., email, phone, and video) involved. Work by Cady and Finkelstein also addressed at least two out of these three dimensions of workflow [19, 22, 24]. The authors developed mixed methods to analyze the workflow of clinicians (focusing on nurses) after the implementation of a real-time live video telemedicine platform. The authors combined qualitative analysis of cognitive ethnography data and quantitative analysis of time-motion studies data to understand the differences in the resources and time (time on task) requirements, before and after the integration of a telemedicine system.
Discussion
Telemedicine is a broad concept involving the use of novel technologies to provide remote health care to a patient population. Its implementation may vary according to several factors, such as the telemedicine modality used, the medical condition of the patient population, the intended functionality, the agents involved in the process, and the readiness of the clinical environment to adopt new technology. As a consequence, the intrinsic variability in the study of integrating telemedicine into clinical workflow- in addition to the lack of a coherent understanding of the definition of workflow within the research community [33], leads to results that are limited in their generalizability. For example, the findings from a study of the integration of RPM in an outpatient clinic environment may not be generalizable for the integration in other healthcare settings or even for other telemedicine modalities. Even with these limitations, the studies published in this area provide valuable insight into the complexities that understanding telemedicine integration implies.
Unertl, et al. [33] developed a conceptual framework of the elements to include when studying workflow in any field. According to the authors, the study of workflow has two levels, pervasive and specific [33]. The pervasive level includes three factors: context, temporal factors (e.g., scheduling and coordination of events), and aggregate factors (relationship and interaction between the different tasks and actors). The specific level is composed of the actors, artifacts, actions, characteristics, and outcomes involved in the workflow. This conceptual framework overlaps with Kaufman, et al. [14] three-dimensional vision of workflow noted above. Published literature on telemedicine integration tends to focus on the third dimension, measuring the impact on time as a metric to assess the success of the technology implementation. Even when savings in time are a definite benefit of adopting a telemedicine system, the study of telemedicine integration requires the assessment of the other two dimensions in the workflow analysis, which has not been well addressed in the published literature. A limitation in the majority of the quantitative studies published in this area is the focus on analyzing the telemedicine activities in isolation, ignoring other direct or indirect effects on other task and organizational non-telemedicine related aspects of the clinical workflow.
Qualitative studies in this research area have provided a more holistic understanding of telemedicine integration, providing insights about the barriers and facilitators to telemedicine integration in clinical workflow. However, most of the studies focus only on understanding the integration from the perspective of physicians, nurses, or both. It is essential to recognize that physicians and nurses are not the only entities impacted by the integration of telemedicine technologies. The workflow of other personnel, such as medical assistants and medical staff, could be impacted too. However, few research efforts involve these parties, who in some settings perform enrollment, scheduling, and other administrative activities relevant to the telemonitoring system.
Qualitative and mixed methods research findings about benefits and challenges, such as disruption and inefficiencies in the integration of telemedicine, are descriptive and informative. However, once the critical actual or potential challenges and contributors to disruption and inefficiencies are identified, there is a need to assess how to lead the process improvement efforts. This may require the connection of those identified challenges and contributors to the components of the work system and the telemedicine system architecture to identify where the process improvement efforts should be directed. Contributions in any of the identified gaps will be a step forward towards improving the acceptability, trust, and integration of a technology that seems to continue shifting healthcare delivery from hospital or clinics into the patients’ home, becoming a vital component of the future of healthcare delivery.
Conclusion
Telemedicine is a health technology area that will continue developing over the years. This scoping review was limited to research articles that included empirical studies for assessing the impact of the integration of telemedicine in general. Even when distinctions are made between the four modalities of telemedicine, not further efforts were made to analyze each modality individually and establish the similarities and differences among them. This limitation is expected to be addressed in future research efforts. Despite this limitation, the conducted scoping review provided valuable insights regarding the methods that have been used in the literature to understand the impact of telemedicine integration into clinical workflow, and the gaps and potential areas of opportunity for future research in this area. In particular three approaches to study telemedicine integration in clinical workflow predominate the academic literature: First, quantitative data analysis techniques applied to time studies, time-motion studies, and surveys and interviews; second, qualitative data analysis techniques applied to interviews, surveys, and observational studies; and third, mixed methods to assess telehealth integration. Literature identifies time-saving as a significant benefit of telemedicine. However, physicians, nurses and other relevant stakeholders have concerns that cannot necessarily be measured in terms of time. Additional research is needed to address other dimensions of clinical workflow, collect holistic perspectives of integration issues from stakeholders, and connect those issues to the specific components of the telemedicine system to prioritize in process improvement.
Funding
This research was partly funded by the National Science Foundation Engineering Research Center Precise Advanced Technologies and Health Systems for Underserved Populations (PATHS-UP).
Conflict of Interest
The authors declare that there is no conflict of interest.
References
-
Thakkar M, Davis DC (2006) Risks, barriers, and benefits of EHR systems: A comparative study based on size of hospital. Perspectives in Health Information Management 3: 5.
-
Hailey D, Roine R, Ohinmaa A (2002) Systematic review of evidence for the benefits of telemedicine. Journal of Telemedicine and Telecare 8(S1): 1-30.
-
Chaudhry B, Wang J, Wu S, Maglione M, Mojica W, et al. (2006) Systematic review: Impact of health information technology on quality, efficiency, and costs of medical care. Annals of Internal Medicine 144(10): 742-752.
-
Hjelm NM (2005) Benefits and drawbacks of telemedicine. Journal of Telemedicine and Telecare 11(2): 60-70.
-
Wootton R (2012) Twenty years of telemedicine in chronic disease management-an evidence synthesis. Journal of Telemedicine and Telecare 18(4): 211-220.
-
Sood S, Mbarika V, Jugoo S, Dookhy R, Doarn C, et al. (2007) What is telemedicine? A collection of 104 peer- reviewed perspectives and theoretical underpinnings. Telemed J E Health 13(5): 573-590.
-
Health Resources and Services Administration (2019) Telemedicine and Telehealth. HealthIT.gov.
-
Jarvis-Selinger S, Chan E, Payne R, Plohman K, Ho K (2008) Clinical telehealth across the disciplines: Lessons learned. Telemedicine Journal and E-Health 14(7): 720- 725.
-
Zheng K, Haftel HM, Hirschl RB, O’Reilly M, Hanauer DA (2010) Quantifying the impact of health IT implementations on clinical workflow: A new methodological perspective. Journal of the American Medical Informatics Association 17(4): 454-461.
-
Brooks E, Turvey C, Augusterfer EF (2013) Provider barriers to telemental health: Obstacles overcome, obstacles remaining. Telemedicine Journal and E-Health 19(6): 433-437.
-
Tricco AC, Lillie E, Zarin W, O’Brien KK, Colquhoun H, et al. (2018) PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Annals of Internal Medicine 169(7): 467-473.
-
CCHP (2019) About Telehealth. Center for Connected Health Policy.
-
Tang Z, Weavind L, Mazabob J, Thomas EJ, Chu-Weininger MYL, et al. (2007) Workflow in intensive care unit remote monitoring: A time-and-motion study. Critical Care Medicine 35(9): 2057-2063.
-
Kaufman DR, Pevzner J, Rodriguez M, Cimino JJ, Ebner S, et al. (2009) Understanding workflow in telehealth video visits: Observations from the ideatel project. Journal of Biomedical Informatics 42(4): 581-592.
-
Cady R, Finkelstein S, Lindgren B, Robiner W, Lindquist R, et al. (2010) Exploring the translational impact of a home telemonitoring intervention using time-motion study. Telemedicine Journal and E-Health 16(5): 576- 584.
-
Fish A, George S, Terrien E, Eccles A, Baker R, et al. (2011) Workflow concerns and workarounds of readers in an urban safety net teleretinal screening study. AMIA Annual Symposium Proceedings 2011: 417-426.
-
Cronin EM, Ching EA, Varma N, Martin DO, Wilkoff BL, et al. (2012) Remote monitoring of cardiovascular devices: A time and activity analysis. Heart Rhythm 9(12): 1947- 1951.
-
Armstrong AW, Kwong MW, Chase EP, Ledo L, Nesbitt TS, et al. (2012) Teledermatology operational considerations, challenges, and benefits: The referring providers’ perspective. Telemedicine Journal and E-Health 18(8): 580-584.
-
Cady RG, Finkelstein SM (2012) A mixed methods approach for measuring the impact of delivery-centric interventions on clinician workflow. AMIA Annual Symposium Proceedings 2012: 1168-1175.
-
Koopman RJ, Wakefield BJ, Johanning JL, Keplinger LE, Kruse RL, et al. (2014) Implementing home blood glucose and blood pressure telemonitoring in primary care practices for patients with diabetes: Lessons learned. Telemedicine Journal and E-Health 20(3): 253-260.
-
Shaw RJ, Kaufman MA, Bosworth HB, Weiner BJ, Zullig LL, et al. (2013) Organizational factors associated with readiness to implement and translate a primary care based telemedicine behavioral program to improve blood pressure control: The HTN-IMPROVE study. Implementation Science 8: 106.
-
Cady RG, Finkelstein SM (2013) Mixed-methods approach for measuring the impact of video telehealth on outpatient clinic triage nurse workflow. Computers, Informatics, Nursing 31(9): 439-449.
-
Uscher-Pines L, Kahn JM (2014) Barriers and facilitators to pediatric emergency telemedicine in the united states. Telemedicine Journal and E-Health 20(11): 990-996.
-
Cady RG, Finkelstein SM (2014) Task-technology fit of video telehealth for nurses in an outpatient clinic setting. Telemedicine Journal and E-Health 20(7): 633-639.
-
Ricci RP, Morichelli L, D’Onofrio A, Calò L, Vaccari D, et al. (2014) Manpower and outpatient clinic workload for remote monitoring of patients with cardiac implantable electronic devices: Data from the HomeGuide Registry. Journal of Cardiovascular Electrophysiology 25(11): 1216-1223.
-
Facchin D, Baccillieri MS, Gasparini G, Zoppo F, Allocca G, et al. (2016) Findings of an observational investigation of pure remote follow-up of pacemaker patients: Is the in-clinic device check still needed? International Journal of Cardiology 220: 781-786.
-
Yen PY, Lara B, Lopetegui M, Bharat A, Ardoin S, et al. (2016) Usability and workflow evaluation of “RhEumAtic Disease activitY” (READY). A mobile application for rheumatology patients and providers. Applied Clinical Informatics 7(4): 1007-1024.
-
Lopetegui M, Yen PY, Lai A, Jeffries J, Embi P, et al. (2014) Time motion studies in healthcare: What are we talking about? Journal of Biomedical Informatics 49: 292-299.
-
Carayon P, Hundt AS, Karsh BT, Gurses AP, Alvarado CJ, et al. (2006) Work system design for patient safety: The SEIPS model. BMJ Quality & Safety 15(S1): i50–i58.
-
Miles MB, Huberman AM (1994) Qualitative Data Analysis: An Expanded Sourcebook. Sage Publications, Thousand Oaks.
-
MacQueen KM, McLellan E, Kay K, Milstein B (1998) Codebook development for team-based qualitative analysis. CAM Journal 10(2): 31-36.
-
Weiner BJ (2009) A theory of organizational readiness for change. Implementation Science 4(1): 67.
-
Unertl KM, Novak LL, Johnson KB, Lorenzi NM (2010) Traversing the many paths of workflow research: Developing a conceptual framework of workflow terminology through a systematic literature review. Journal of the American Medical Informatics Association 17(3): 265-273.
- The Expanding Landscape of Road Rage: A Systematic Review of Conflicts Involving Drivers, Pedestrians, and Micromobility
- Validating Cognitive Models of Royal Navy Performance on Control Systems
- Comparing Standard and State-of-the-art Firefighter Coats on Postural Balance and Gait in a Live Burn Environment
- Risk Assessment of Ergonomic Factors in a Textile Firm by RULA, REBA and Fine Kinney Methods
- Impact of Self-Esteem Training on Individuals with Disabilities Aged 17-30
- Effects of a Psychotherapeutic Pathway Based on Mindfulness, Acceptance and Commitment Therapy and Creative Contact with Nature in People with Mild Intellectual Disability