Effects of a Psychotherapeutic Pathway Based on Mindfulness, Acceptance and Commitment Therapy and Creative Contact with Nature in People with Mild Intellectual Disability
Mild intellectual disability is characterized by a limited ability to adapt to novel situations and difficulties in managing emotions. Common challenges faced by individuals with mild intellectual disability include difficulty managing anger and reduced psychological flexibility, factors that can hinder their ability to cope with daily challenges and negatively impact their quality of life. The current study demonstrates that an integrated psychotherapeutic program, incorporating Mindfulness exercises, the third-generation cognitive-behavioural approach known as Acceptance and Commitment Therapy (ACT), and interactions with nature inspired stimuli either imagined or co-created with the participant (for example billboards depicting sea or mountain landscapes, plants present in the psychotherapeutic work context, background nature sounds, etc.), can enhance psychological flexibility, anger management skills, reduce perceived stress, and improve subjective well-being in individuals with mild intellectual disability. The sample, consisting of 20 people with mild intellectual disability aged 17-26 years showed significant improvements after the intervention. These results fill the existing gap in the literature. Historically, research has often emphasized the limitations associated with patients’ cognitive impairments, overlooking their inherent strengths and underutilizing their personal resources. As a result, reduced cognitive ability has frequently been cited as a barrier to benefiting from psychological counselling, leading to limited therapeutic options being offered to this population
Abbreviations
ACT: Acceptance and Commitment Therapy; DSM-V: Diagnostic and Statistical Manual of Mental Disorders; MBSR: Mindfulness-Based Stress Reduction; MBCT: Mindfulness- Based Cognitive Therapy; SWLS: Satisfaction with Life Scale; PSS: Perceived Stress Scale.
Introduction
Mild intellectual disability is characterized by a limited ability to adapt to novel situations and difficulties in managing emotions. According to the WHO classification, “Intellectual developmental disorders are a group of etiologically diverse conditions that originate during the developmental period, characterized by significantly below average intellectual functioning and adaptive behavior, i.e., about two or more standard deviations below the mean” [1]. According to the Diagnostic and Statistical Manual of Mental Disorders (DSM-V), deficits in intellectual function include reasoning, problem solving, planning, abstract thinking, judgment, and, finally, academic and experiential learning [2].
Adults with mild intellectual disability show deficits and limitations in executive functions such as planning, organizing, prioritizing, and abstract thinking [2]. Moreover, they present limitations in activities requiring short- term memory. In addition, they run a higher risk of being manipulated by others, show difficulties to accurately judge or understand the norms of discourse and social interactions, and, often, their behavior in social situations may be considered immature or inappropriate to the context [2]. Therefore, deficits in adaptive functioning result in failure to meet sociocultural developmental standards for personal independence and social responsibility [3]. They also limit social awareness of others’ thoughts, feelings, and experiences, empathy, interpersonal communication skills, ability to develop friendships, and social judgment skills [3].
Common challenges faced by individuals with mild intellectual disability include difficulty managing anger and reduced psychological flexibility, factors that can hinder their ability to cope with daily challenges and negatively impact their quality of life. Indeed, the literature shows that adolescents with mild intellectual disability are three- to four times more likely to develop behavioural problems compared to their peers without intellectual disability [4]. The risk includes externalizing problems such as aggression and delinquency [5], as well as challenges with self-regulation, emotion regulation, behaviors, and cognition [6].
Both children and adolescents with mild to moderate intellectual disabilities have a lower capacity for self- regulation compared to their peers with typical development [7]. In addition, research on coping strategies, the conscious efforts to regulate emotions, cognition, behaviors, and physiology in response to stressful events or circumstances [8], show that adults with mild intellectual disability tend to use fewer emotion-focused coping strategies, which could indicate specific difficulties in emotional management [9].
Several psychotherapeutic approaches have consistently proven effective in enhancing emotional management and psychological flexibility, which are recognized as two central constructs for biopsychosocial well-being [10]. The third-generation Cognitive Behavioral approach known as Acceptance and Commitment Therapy (ACT) appears in the literature to be functional and it gains added value when integrated with Mindfulness exercises. The term “Mindfulness-based interventions” refers to a set of practices that aim to intentionally bring one’s attention to experiences occurring in the present moment, without applying judgment to them [11]. They derive from an intervention formalized by Kabat Zinn in the 1990s called “Mindfulness-Based Stress Reduction” (MBSR), aimed at cultivating non-processing moment-to-moment attention to achieve awareness of external and internal events, such as thoughts, emotions, and bodily sensations [12, 13].
The focus is on the awareness of the present moment and acceptance of things as they are, however they are in reality, rather than chasing a specific desired outcome in the future [14]. It implies mindfulness through an open and receptive attitude to what is happening in the present moment, cultivating a present experience with acceptance [15]. Mindfulness practice and mindful attitude can help people to embrace evaluative thoughts that have already occurred as they are, without suppression or distortion, maintain a subtle distance from mental experiences, and observe thoughts as mental events that do not necessarily reflect the facts of reality [16].
Overall, the greatest effectiveness of Mindfulness- based practice as a treatment has been found in treating recurrent depression [17]; indeed, rumination tendency predicts future depressive symptoms in adults [18]. Research conducted by Cladder-Micus, et al. [19] showed that participants who practiced MBCT had a decrease in negative intrusive thoughts, compared to the control group. Studies conducted by Proeve, et al. [20] showed significant reductions in shame, anxiety, stress, and rumination through the use of Mindfulness. Mindfulness interventions train two stress resilience pathways at the brain level: they increase activity and functional connectivity in the stress-regulatory regions of the prefrontal cortex and decrease activity and functional connectivity in the stress-alert system regulatory brain regions [21]. Large randomized studies show that Mindfulness interventions can improve pain management outcomes [22, 23]. In addition, those who practice Mindfulness regularly report improved performance in working memory and sustained attention [24], as well as reduced symptoms of anxiety [25, 26].
Acceptance and Commitment Therapy is a third- generation cognitive behavioural therapy capable of working on six processes: acceptance, defusion, values, committed actions, self as context, and contact with the present moment, so that human beings can choose to change certain behavioural traits [27]. ACT promotes acceptance of unpleasant and intense emotions, helping people to live according to their values [28]. The main purpose is to help individuals acquire the skills to control effectively pain and suffering in order to lead a meaningful and successful life experience [29]. The main message of ACT is “to accept things as they are when they are beyond one’s control and to commit to doing so while maintaining behavior that enrich one’s life [30].” ACT is considered a method for moderating anger and aggression by teaching individuals to accept evens of life and maintain a responsible attitude in line with their personal values [31]. ACT aims to teach individuals to notice and recognize anger-related thoughts and feelings in order to respond to them less impulsively and decrease their credibility by engaging in the pursuit of important life goals [32]. Indeed, ACT teaches individuals to “act out life, not anger” by choosing to consistently live according to their personal values [32].
Psychological flexibility lies at the core of ACT [33, 34] and it is defined as the “ability to engage more fully with the present moment as a conscious human being, while adapting or maintaining behaviors that align with one’s valued goals” [35]. In contrast, psychological inflexibility is characterized by a behavioural pattern of excessive control of thoughts, feelings, and emotions, with a tendency to avoid unpleasant internal experiences at the expense of more effective or valuable actions [36]. Experiential avoidance is the most widely studied component of psychological inflexibility [37]. It is defined as behavior that attempts to “alter the frequency or form of undesirable internal events, including thoughts, memories, and bodily sensations, even when it causes personal harm” [38]. Experiential avoidance has been linked to a wide range of relevant clinical phenomena [39, 40].
For example, experiential avoidance has been found to be a key process in emotional disorders [41], depressive symptoms [42], uncontrolled eating [43], body image disorders [44], in social anxiety [45], in chronic pain [46], in anxiety and stress sensitivity [47], in trauma [48], and in post-traumatic stress disorder [49]. The present study aims to integrate the use of Acceptance and Commitment Therapy with Mindfulness and contact with elements belonging to nature reproduced by the user or constructed by the therapist, within the psychotherapy room. The literature suggests that interaction with nature or natural elements in artificial environments (such as billboards depicting landscapes of the sea or mountains, real plants to take care of, background nature sounds, etc.) can have numerous psychological benefits and have a significant increase in people’s physical and mental well-being [50].
Physical health benefits include, for example, greater physical fitness, lower blood pressure and fewer symptoms of illness [51]; on the other hand, in terms of mental health benefits, it includes greater satisfaction and motivation, lower levels of stress and anxiety, greater comfort, better problem solving, and higher levels of creativity. In addition, there may also be benefits in terms of behavioural change: this includes better coping skills, increased attention and concentration, improved social interaction, and less hostility and aggression [51].
Oh and coworkers [52], highlighted the connection with nature as the key element moderating the relationship between the duration of exposure to nature and mental well-being outcomes: in fact, individuals with a stronger connection with nature were less likely to experience symptoms of depression, stress, and anxiety, regardless of the time spent in nature; whereas, individuals with a weaker connection to nature were more likely to experience more symptoms as the duration of time spent in nature increased.
Therefore, the researchers did not identify a direct relationship between the amount of exposure to nature and positive outcomes in terms of mental well-being, since mediating this relationship was the sense of connectedness to nature [52]. Similarly, Colding and Barthel [53] found that even as little as 10-20 minutes of time spent sitting or walking in nature can have a beneficial effect on young adults’ mental health, compared to the same amount of time spent in urbanized environments. In Herrington and Brussoni’s [54] study, natural elements were incorporated into the playgrounds of two kindergartens that had only structured and artificial play spaces. Before the installation, children displayed behaviors such as “channel surfing” (tendency to move from one game to another without ever completing any of them) and repetitive movements, such as walking back and forth. After the installation of the new natural material, the children’s movement pattern became more complex [54].
These findings highlight the benefits of engaging with nature and participating in pro-nature behaviors [55]. Connecting with nature increased concentration, creativity and happiness; it stimulates the immune system and pro- social behaviors [56]. In fact, according to Gordon [56], the natural context consciously or unconsciously draws attention, and promotes calm, rest, and contemplation. The aim of the current study is to evaluate improvements in psychological flexibility and anger management in a sample of 20 individuals with mild intellectual disability (ages 17-26 years) who participated in an integrated psychotherapeutic program based on Mindfulness, ACT, and nature connection interventions.
Materials and Methods
Sample
The sample consisted of 20 people with mild intellectual disability, with an average age of 21.5 years (ds=3.2), referred to the Disability Service S.C. Corporate Psychology on referral from the Child Neuropsychiatry South and North, East and West and the S.C. Care and Disability of the City of Turin. The diagnosis of mild intellectual disability was confirmed by clinical evaluation and standardized cognitive tests. All participants were informed about the purpose of the study and provided informed consent. The disabilities in the sample included both physical (n = 2) and mild cognitive (n = 18) problems. The sample consisted of 9 females and 11 males. Seventeen participants had already graduated from high school. All participants live in Turin in the Piedmont region.
Materials and Procedures
The individual psychotherapeutic program was structured in 8 weekly meetings lasting 90 minutes each, for a total duration of 8 weeks. Interventions were conducted on the basis of a multimodal model integrating the third- generation cognitive behavioural approach known as Acceptance and Commitment Therapy, Mindfulness exercises and nature-based activities. Specifically, interventions followed protocols from the Mindfulness-Based Cognitive Therapy (MBCT), which has demonstrated remarkable results; it is a group psychosocial intervention that includes training in Mindfulness and elements of cognitive behavioural psychotherapy [19].
The primary objective of this program is to help participants relate to their thoughts, emotions, and bodily sensations with awareness, thereby interrupting the dysfunctional cycles of rumination, maladaptive emotion regulation, and self-criticism [57]. The intervention is designed to encourage a more “decentered” perspective, where the person is less identified with the content of thoughts and feelings and more able to observe them as transient phenomena on which there is no need to act [57]. These Mindfulness interventions included exercises such as body scans, mindful breathing, and present- moment meditation. Interventions based on Acceptance and Commitment Therapy (ACT) have centered work on psychological flexibility, a broad and overarching construct composed of six distinct sub-processes: acceptance, cognitive defusion, self-considered as context, present- moment awareness, values, and enactment of actions oriented to one’s values [35]. ACT seeks to reduce cognitive rigidity, which often manifests as experiential avoidance, cognitive fusion, an overly fixed sense of self, lack of present-moment awareness, disconnection from personal values, and actions that do not align with one’s values [36]. Specifically, the interventions aimed to convey exercises based on acceptance of intense and unpleasant emotions, identification of personal values, and engagement in behaviors that reflect one’s own values.
Finally, sessions were organized with the presence or construction of elements belonging to the outdoors and natural parks (such as billboards depicting landscapes of the sea or mountains, real plants to take care of, background nature sounds, etc.), including activities of observing and interacting with the natural environment to reduce stress and promote emotional well-being. Indeed, it has been shown by several researches that engaging in nature directly or indirectly in a variety of forms (through nature walks, nature-based tourism, living closer to nature, and immersive experiences provided by virtual and imaginative reality) positively affects well-being [58]. A study from Franco and colleagues in 2017 showed that when we are surrounded by nature we use our sensory organs and even some non-sensory ones to stimulate the brain, reduce stress and unpleasant emotions, and increase pleasant ones instead. The following questionnaires were administered to each participant before and after the intervention: AAQ-II, STAXI-2 and a series of multiple-choice questionnaires to assess levels of perceived stress and well-being [59].
The AAQ-II is the “Psychological Flexibility Questionnaire”; it is a validated 7-item scale that measures psychological flexibility, defined as the ability to accept unpleasant thoughts and emotions without avoiding them, while maintaining value-oriented behavior. A lower score indicates greater psychological flexibility. The initial effort in developing a measure of the psychological variables covered by the ACT was the design of a unidimensional self-assessment measure called the Acceptance and Action Questionnaire [60]. The AAQ was presented as a measure of experiential avoidance, although its items contemplated a broader construct.
For instance, the AAQ items contained descriptions related to negative evaluations of feelings, avoidance of private events, distancing from thoughts, and behavioural flexibility in the presence of difficult personal events. The second version of the AAQ was designed to overcome the difficulties encountered with the first version; specifically, to develop a unidimensional measure, Bond, et al. [61] asked a group of 12 ACT researchers and practitioners to create items describing psychological flexibility and inflexibility. The preliminary 10-item version of the AAQ-II contained seven items describing psychological inflexibility and three describing psychological flexibility.
However, the final version of the AAQ-II eliminated the three items describing psychological flexibility through factor analysis that produced a two-factor solution. Therefore, the final version of the AAQ-II was presented as a measure of psychological inflexibility [61]. The 7-item version of the AAQ-II revealed stronger psychometric properties than both the 10-item version of the AAQ-II and the first version of the AAQ [61]. In addition, the 7-item version of the AAQ-II has acceptable reliability and validity values for measuring psychological inflexibility [62].
The STAXI- 2 is the Anger Expression Scale [63]: it is a measure of the frequency, intensity and patterns of anger expression, with subscales to assess withheld anger, expressed anger and anger control. The STAXI-2 contains 57 items divided in 3 sections (anger as a state, anger as a trait and expression and control of anger). Responses range from 1 (almost never) to 4 (almost always) on a Likert-type scale and scores are converted to percentiles based on gender and age [63]. Anger as a trait is measured using 10 items to assess the frequency with which anger is experienced over time [64]. In contrast, the anger expression and anger control subscales have 8 items each: the externalizing anger expression subscale (AX-O) assesses how often anger is expressed with physical or verbal aggression, while the internalizing anger expression subscale (AX-I) assesses how often anger is experienced but is repressed [64].
The externalizing anger control subscale (AC-O) measures how often a person attempts to control the expression of anger, while the internalizing anger control subscale (AC-I) assesses how often a person attempts to control feelings of anger by actively calming down [64]. Finally, participants completed a series of multiple-choice questionnaires to assess levels of perceived stress and subjective well-being. The Perceived Stress Scale (PSS) by Sheldon Cohen [65] is a psychometric instrument designed to measure the level of stress perceived by individuals, providing a subjective assessment of their stress status.
The Perceived Stress Scale (PSS; Scale for Perceived Stress) is one of the most widely used tool for assessing stress perception in various life context. Its items are designed to capture the extent to which respondents perceive their lives as unpredictable, uncontrollable, or overwhelming. The scale also contains a series of direct questions about current levels of perceived stress. The PSS is suitable for the general population with an educational level of at least junior high school. Both the items and the response alternatives are easy to understand.
The questions are general, making them applicable to diverse populations. The PSS questions are about feelings and thoughts related to the past month. For each item people are asked to indicate how often they felt a certain way. Responses are recorded on a 5-point Likert scale ranging from “never (0)” to “very often (4).” Higher PSS scores were found to be associated with high perceived stress. Scores are calculated by reversing the responses (e.g., 0 = 4, 1 = 3, 2 = 2, 3 = 1, and 4 = 0) given to the four positively worded items (items 4, 5, 7, and 8) and then summing all items on the scale. The others remain unchanged. A short scale of 4 items can be obtained from questions 2, 4, 5 and 10 of the 10-item PSS scale.
Finally, the Satisfaction with Life Scale (SWLS), developed by Ed Diener and colleagues is a questionnaire that measures subjective well-being and helps to understand how happy and fulfilled a human being feels in the present moment. The SWLS consists of 5 questions, which must be answered using a Likert scale (5 response types ranging from totally disagree, disagree, neutral, agree, fully agree). The SWLS also allows one to assess how life satisfaction evolves during a course of psychotherapy. Therefore, it can be considered a very reliable and interesting tool in the field of psychology and research. Low scores on the test indicate a low degree of perceived subjective well-being.
Data Analysis and Results
To evaluate the effectiveness of the intervention, data were collected before and after the psychotherapeutic program. Statistical analyses were conducted using the paired samples t-test to compare pre- and post-intervention scores with respect to psychological flexibility, anger management, and levels of perceived stress and subjective well-being.
A p value < 0.05 was considered significant in the analysis of the results and their comparison. The study employed a within-subjects design, comparing each participant’s results before (pre) and after (post) the intervention. Therefore, individual’s changes were assessed in order to obtain a measure of the effectiveness of the intervention with respect to the variables analyzed.
The results obtained, shown in the graph below, outline the observed changes for each variable examined:
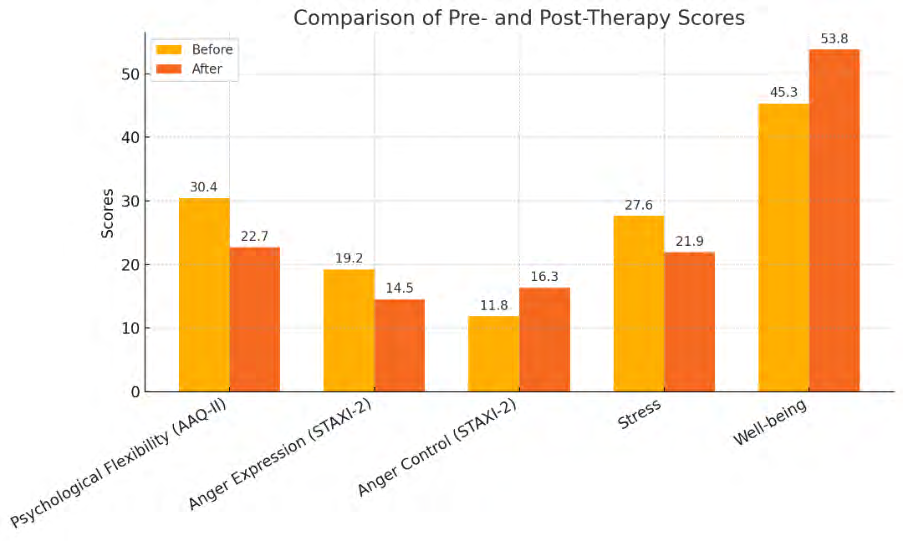
Psychological flexibility, as measured by the AAQ-II, showed notable improvement following the intervention. The pre-intervention mean score on the AAQ-II scale was 30.4 (SD = 6.2), while the post-intervention mean score dropped to 22.7 (SD = 5.1). Since the AAQ-II measures Psychological Flexibility through items that reflects its opposite, i.e., Psychological Inflexibility, it is expected that individuals with high levels of Psychological Flexibility would obtain lower scores than individuals with higher Psychological Inflexibility. The results reveal a significant reduction in scores from the pre- to post-intervention assessment, indicating substantial improvement (t(19) = 5.12, p < 0.001). Specifically, 75% of participants experienced a reduction in their AAQ-II scores, with an average improvement of 25%. These results suggest that the integrated psychotherapy intervention based on ACT, Mindfulness and contact with nature led to a 25% improvement in Cognitive Flexibility.
With respect to the management of Anger, as measured by the STAXI-2, the pre- and post-intervention results of the Expressed Anger and Anger Control sections were compared. The mean scores on the STAXI-2 scale for Expressed Anger pre-intervention were 19.2 (SD = 3.8), while post- intervention scores were 14.5 (SD = 3.2) (t(19) = 4.45, p < 0.01). The Expressed Anger scale assesses how often anger is expressed with physical or verbal aggression and how often anger is experienced but is repressed (Mc Ewan et al., 2009). These results indicate a 24.5 percent improvement in the Expressed Anger variable.
Regarding the Anger Control scale, the mean scores of the pre-intervention administration were 11.8 (SD = 2.9), while the mean post-intervention scores were 16.3 (SD = 3.4) (t(19) = 5.23, p < 0.001). These results show that the integrated intervention enhanced in a 27.6 percent Anger Control. The Perceived Stress Scale (PSS) indicated a 20.7% reduction in stress levels. The mean pre-intervention score was 27.6 (SD = 4.5), while the post-intervention mean dropped to 21.9 (SD = 4.1) (t(19) = 4.16, p < 0.01). This decline reflects a significant decrease in perceived stress levels among participants. Regarding subjective well-being, as measured by the Satisfaction With Life Scale (SWLS), mean scores increased from 45.3 (SD = 6.7) pre-intervention to 53.8 (SD = 6.2) post-intervention (t(19) = 4.68, p < 0.001). This 15.8% improvement highlights the positive impact of the intervention of ACT, Mindfulness and contact with nature on participants’ perceived life satisfaction. This study followed standard research criteria, reporting quantitative and objective data to support the initial hypotheses and providing rigorous statistical analysis. There are significant improvements in all areas: Psychological Flexibility, Psychological Wellbeing and Anger Control; in addition, there was a reduction in levels of Perceived Stress.
Discussion
The objective of the present study was to evaluate improvements in psychological flexibility and anger management, as well as in perceived stress and subjective well-being in a sample of 20 persons with mild intellectual disability (ages 17-26 years) who participated in an integrated psychotherapeutic program based on Mindfulness interventions, Acceptance and Commitment Therapy, and nature connection interventions. The results of the study highlight the effectiveness of this approach in anger management, perceived stress and subjective well-being, as well as psychological flexibility. Specifically, the results showed a 25 percent increase in psychological flexibility, a 24.5 percent improvement in anger expression, a 27.6 percent increase in anger control, a 20.7 percent decrease in perceived stress, and a 15.8 percent increase in psychological well-being. The 25% improvement in psychological flexibility is particularly noteworthy, as this skill plays a pivotal role in adapting to daily emotional difficulties.
Psychological flexibility is at the core of ACT [33, 34] and it is defined as the “ability to contact the present moment more fully as a conscious human being and to change or persist in behavior when it serves the esteemed ends” [35]. In fact, ACT interventions aim to teach individuals to notice and recognize anger-related thoughts and feelings in order to respond to them less impulsively and diminish their credibility by engaging in the pursuit of important life goals [32]. Such interventions aim to limit the rigidity given by cognitive inflexibility, which includes experiential avoidance, cognitive fusion, the self-viewed as content, lack of awareness of the present moment, lack of values, and enactment of actions not oriented toward the pursuit of one’s personal values [36].
For individuals with mild intellectual disabilities, the tendency to rely heavily on others for decision-making and problem-solving can often result in feelings of frustration and discomfort, leading to manifestations of anger and aggression [66]. This study demonstrated that an integrated therapeutic approach can support these individuals in learning more functional strategies for handling problems and conflicts, as evidenced by the significant reduction in expressed anger and the improvement in anger control scores. In addition, research on coping strategies shows that adults with mild intellectual disability use fewer emotion- focused coping strategies than non-emotion-focused coping strategies, which could indicate specific difficulties in emotional management [9].
Improvement in psychological flexibility and anger management was also reflected in reduced perceived stress and increased psychological well-being. Indeed, these findings further confirm the effectiveness of an integrated intervention between ACT, Mindfulness, and connection with nature in improving cognitive flexibility and anger management in a sample of people with mild intellectual disability. However, a limitation of the study is the small experimental sample size of 20 people and the lack of a control group. Indeed, such a small sample makes generalization of the results difficult; nevertheless, these results serve as an important foundation for future research. In the future, randomized trials with larger samples could confirm the applicability and validity of the results.
In addition, the presence in the future of a control sample would ensure a more specific evaluation of the validity of an integrated intervention between ACT, Mindfuness and contact with nature in improving cognitive flexibility, anger management, reduction of perceived stress and psychological well-being. The possibility of long- term follow-up data should be included in order to test the sustainability of the effects of time intervention. Future studies could also explore individual differences in response to the intervention to refine the strategies and improve the target or the effectiveness of the intervention could be tested in a real natural context such as a park, beach or mountain.
Conclusion
In conclusion, this study provides preliminary evidence on the effectiveness of an integrated psychotherapeutic intervention based on Mindfulness, Acceptance and Commitment Therapy and contact with nature in improving psychological flexibility and anger management in people with mild intellectual disability. The results suggest that these approaches may be effective in promoting emotional well- being and reducing stress symptoms. Moreover, an integration of these methods could be useful in psychological support programs for people with intellectual disabilities, contributing to a higher quality of life and better management of difficult emotions. Psychotherapy for individuals with mild intellectual disabilities also provides a valuable opportunity to establish a secure therapeutic relationship, promote self-awareness and self-esteem, encourage emotional expression, and cultivate more socially appropriate behavioural strategies [67, 68, 69, 70, 71].
References
-
WHO (2020) Disorders of intellectual development. World Health Organisation.
-
APA (2013) Diagnostic and Statistical Manual of Mental Disorders. 5th(Edn.), American Psychiatric Press, Washington DC, USA, pp: 31-86.
-
Patel DR, Cabral MD, Ho A, Merrick J (2020) A clinical primer on intellectual disability. Translational pediatrics 9(1): S23.
-
Dekker MC, Koot HM, Ende JVD, Verhulst FC (2002) Emotional and behavioural problems in children and adolescents with and without intellectual disability. Journal of Child Psychology and Psychiatry 43(8): 1087-1098.
-
Douma JC, Dekker MC, Ruiter KPD, Tick NT, Koot HM (2007) Antisocial and delinquent behaviors in youths with mild or borderline disabilities. American Journal on Mental Retardation 112(3): 207-220.
-
Bridgett DJ, Oddi KB, Laake LM, Murdock KW, Bachmann MN (2013) Integrating and differentiating aspects of self-regulation: effortful control, executive functioning, and links to negative affectivity. Emotion 13(1): 47.
-
Nader-Grosbois N (2014) Self-perception, self- regulation and metacognition in adolescents with intellectual disability. Research in developmental disabilities 35(6): 1334-1348.
-
Compas BE, Jaser SS, Bettis AH, Watson KH, Gruhn MA, et al. (2017) Coping, emotion regulation, and psychopathology in childhood and adolescence: A meta-analysis and narrative review. Psychological bulletin 143(9): 939.
-
Hartley SL, MacLean Jr WE (2008) Coping strategies of adults with mild intellectual disability for stressful social interactions. Journal of mental health research in intellectual disabilities 1(2): 109-127.
-
Renshaw TL (2018) Probing the relative psychometric validity of three measures of psychological inflexibility. Journal of Contextual Behavioral Science 7: 47-54.
-
Garcia-Campayo J, Hoyo YLD, Navarro-Gil M (2021) Contemplative sciences: A future beyond mindfulness. World Journal of Psychiatry 11(4): 87.
-
Kabat-Zinn J (1990) Full catastrophe living: The program of the stress reduction clinic at the University of Massachusetts Medical Center, USA.
-
Kabat-Zinn J (1990) Full Catastrophe Living: Using the Wisdom of Your Body and Mind to Face Stress, Pain, and Illness. Delacorte, Newyork.
-
Kabat-Zinn J (2003) Mindfulness-based stress reduction (MBSR). Constructivism in the Human Sciences 8(2): 73.
-
Kabat-Zinn J (2013) Some reflections on the origins of MBSR, skillful means, and the trouble with maps. Mindfulness, Routledge, UK, pp: 281-306.
-
Kang Y, Rahrig H, Eichel K, Niles HF, Rocha T, et al. (2018) Gender differences in response to a school- based mindfulness training intervention for early adolescents. Journal of school psychology 68: 163-176.
-
Kuyken W, Warren FC, Taylor RS, Whalley B, Crane C, et al. (2016) Efficacy of mindfulness-based cognitive therapy in prevention of depressive relapse: an individual patient data meta-analysis from randomized trials. JAMA Psychiatry 73(6): 565-574.
-
Nolen-Hoeksema S (1991) Responses to depression and their effects on the duration of depressive episodes. J Abnorm Psychol 100: 569-582.
-
Cladder-Micus MB, Becker ES, Spijker J, Speckens AE, Vrijsen JN (2019) Effects of mindfulness-based cognitive therapy on a behavioural measure of rumination in patients with chronic, treatment-resistant depression. Cognitive Therapy and Research 43(4): 666-678.
-
Proeve M, Anton R, Kenny M (2018) Effects of mindfulness‐based cognitive therapy on shame, self‐ compassion and psychological distress in anxious and depressed patients: A pilot study. Psychology and Psychotherapy: Theory, Research and Practice 91(4): 434-449.
-
Creswell JD, Lindsay EK (2014) How does mindfulness training affect health? A mindfulness stress buffering account. Current directions in psychological science 23(6): 401-407.
-
Cherkin DC, Sherman KJ, Balderson BH, Cook AJ, Anderson ML, et al. (2016) Effect of mindfulness-based stress reduction vs cognitive behavioural therapy or usual care on back pain and functional limitations in adults with chronic low back pain: a randomized clinical trial. Jama 315(12): 1240-1249.
-
Morone NE, Greco CM, Moore CG, Rollman BL, Lane B, et al. (2016) A mind-body program for older adults with chronic low back pain: A randomized clinical trial. JAMA Internal Medicine 176(3): 329-337.
-
Jha AP, Stanley EA, Kiyonaga A, Wong L, Gelfand L (2010) Examining the protective effects of mindfulness training on working memory capacity and affective experience. Emotion 10(1): 54.
-
Khoury B, Lecomte T, Fortin G, Masse M, Therien P, et al. (2013) Mindfulness-based therapy: a comprehensive meta-analysis. Clin Psychol Rev 33: 763-771.
-
Goyal M, Singh S, Sibinga EMS, Gould NF, Rowland- Seymour A, et al. (2014) Meditation programs for psychological stress and well-being a systematic review and meta-analysis. JAMA Intern Med 174: 357-368.
-
Yavuz F (2015) Acceptance and commitment therapy (ACT): An overview. Turkiye Clinics Journal of Psychiatry Special Topics 8(2): 21-27.
-
Hayes SC, Strosahl KD, Wilson KG (2011) Acceptance and Commitment Therapy: The Process and Practice of Mindful Change. Guilford Press, Newyork.
-
Honarparvaran N (2014) The efficacy of acceptance and commitment therapy (ACT) on forgiveness and marital adjustment among women damaged by marital infidelity. J Woman Soc 5(3): 135‐150.
-
Harris R (2017) ACT Made Simple. In: Karatepe HT, et al. (Eds.), Learning the ACT is Easy. 2nd(Edn.), Litera Publishing, Istanbul, Turkey.
-
Tabrizi F, Nezhadmohammad NA (2017) Effectiveness of acceptance and commitment therapy on psychological well-being and anger reduction among mothers with deaf children in Tehran.
-
Eifert GH, Forsyth JP (2011) The application of acceptance and commitment therapy to problem anger. Cognitive and Behavioral Practice 18(2): 241-250.
-
Hayes SC, Strosahl KD, Wilson KG (2003) Acceptance and commitment therapy: An experiential approach to behavior change. Guilford Press, New York.
-
Hayes SC, Strosahl KD, Wilson KG (2011) Acceptance and commitment therapy: The process and practice of mindful change. 2nd (Edn.), Guilford Press, New York.
-
Hayes SC, Luoma JB, Bond FW, Masuda A, Lillis J (2006) Acceptance and commitment therapy: Model, processes, and outcomes. Behavior Research and Therapy 44: 1-25.
-
Levin ME, MacLane C, Daflos S, Pistorello J, Hayes SC, et al. (2014) Examining psychological inflexibility as a trandiagnostic process across psychological disorders. Journal of Contextual Behavioral Science 3: 155-163.
-
Tyndall I, Waldeck D, Pancani L, Whelan R, Roche B, et al. (2020) Profiles of psychological flexibility: A latent class analysis of the acceptance and commitment therapy model. Behavior Modification 44(3): 365-393.
-
Hayes SC, Pistorello J, Levin ME (2012) Acceptance and commitment therapy as a unified model of behavior change. The Counselling Psychologist 40: 976-1002.
-
Chawla N, Ostafin B (2007) Experiential avoidance as a functional dimensional approach to psychopathology: An empirical review. Journal of Clinical Psychology 63: 871-890.
-
Hayes SC, Wilson KG, Gifford EV, Follette VM, Strosahl K (1996) Experiential avoidance and behavioral disorders: A functional diagnostic approach to diagnosis and treatment. Journal of Consulting and Clinical Psychology 64: 1152-1168.
-
Spinhoven P, Drost J, Rooij MD, Hemert AM, Pennix BW (2014) A longitudinal study of experiential avoidance in emotional disorders. Behavior Therapy 45: 840-850.
-
Schut DM, Boelen PA (2017) The relative importance of rumination, experiential avoidance and mindfulness as predictors of depressive symptoms. Journal of Contextual Behavioral Science 6(1): 8-12.
-
Lillis J, Hayes SC, Levin ME (2011) Binge eating and weight control: The role of experiential avoidance. Behavior Modification 35(3): 252-264.
-
Blakey SM, Reuman L, Bucholz JL, Abramowitz JS (2017) Experiential avoidance and dysfunctional beliefs in the prediction of body image disturbance in a non-clinical sample of women. Body Image 22: 72-77.
-
Kashdan TB, Rottenberg J (2010) Psychological flexibility as a fundamental aspect of health. Clinical Psychology Review 30: 865-878.
-
Karademas EC, Karekla M, Flourini M, Vasilou VS, Kasinopoulos, et al. (2017) The impact of experiential avoidance on the relationship between illness representations, pain catastrophising, and pain interference in chronic pain. Psychology & Health 32: 1461-1484.
-
Bardeen JR, Fergus TA, Orcutt HK (2014) The moderating role of experiential avoidance in the prospective relationship between anxiety sensitivity and anxiety. Cognitive Therapy and Research 38: 465- 471.
-
Lewis M, Naugle A (2017) Measuring experiential avoidance: Evidence toward mutlidimensional predictors of trauma sequelae. Behavioral Sciences 7: 9.
-
Kashdan TB, Kane JQ (2011) Post-traumatic distress and the presence of post-traumatic growth and meaning in life: Experiential avoidance as a moderator. Personality and Individual Differences 50: 84-89.
-
Clayton S (2003) Environmental identity: A conceptual and an operational definition. Identity and the natural environment: The psychological significance of nature, pp: 45-65.
-
Kellert SR, Calabrese EF (2015) The Practice of Biophilic Design: A Simplified Framework. The Practice of Biophilic Design.
-
Oh RR, Fielding KS, Chang CC, Nghiem LT, Tan CL, et al. (2021) Health and wellbeing benefits from nature experiences in tropical settings depend on strength of connection to nature. International Journal of Environmental Research and Public Health 18(19): 10149.
-
Colding J, Barthel S (2017) The role of university campuses in reconnecting humans to the biosphere. Sustainability 9(12): 2349.
-
Herrington S, Brussoni M (2015) Beyond physical activity: The importance of play and nature-based play spaces for children’s health and development. Current obesity reports 4: 477-483.
-
Khan F (2020) Nature Contentedness Through Nature’s Affordances.
-
Gordon WV, Shonin E, Richardson M (2018) Mindfulness and nature. Mindfulness 9(5): 1655-1658
-
Schanche E, Vøllestad J, Visted E, Svendsen JL, Osnes B, et al. (2020) The effects of mindfulness-based cognitive therapy on risk and protective factors of depressive relapse–a randomized wait-list controlled trial. BMC psychology 8(1): 57.
-
Richardson M, Passmore HA, Lumber R, Thomas R, Hunt A (2021) Moments, not minutes: The nature-wellbeing relationship. International Journal of Wellbeing 11(1).
-
Franco LS, Shanahan DF, Fuller RA (2017) A review of the benefits of nature experiences: More than meets the eye. International journal of environmental research and public health 14(8): 864.
-
Hayes SC, Strosahl K, Wilson KG, Bissett RT, Pistorello J, et al. (2004) Measuring experiential avoidance: A preliminary test of a working model. The psychological record 54: 553-578.
-
Bond FW, Hayes SC, Baer RA, Carpenter KM, Guenole N, et al. (2011) Preliminary psychometric properties of the Acceptance and Action Questionnaire–II: A revised measure of psychological inflexibility and experiential avoidance. Behavior therapy 42(4): 676-688.
-
Pennato T, Berrocal C, Bernini O, Rivas T (2013) Italian version of the acceptance and action questionnaire-II (AAQ-II): dimensionality, reliability, convergent and criterion validity. Journal of Psychopathology and Behavioral Assessment 35: 552-563.
-
Spielberger CD (1999) State-Trait Anger Expression Inventory-2 (STAXI-2): Professional Manual. Psychological Assessment Resources.
-
McEwan TE, Davis MR, MacKenzie R, Mullen PE (2009) The effects of social desirability response bias on STAXI‐2 profiles in a clinical forensic sample. British Journal of Clinical Psychology 48(4): 431-436.
-
Cohen S, Williamson G (1988) Perceived stress in a probability sample of the US. In: Spacapam S, et al. (Eds.), The Social Psychology of Health: Claremont Symposium on Applied Social Psychology.
-
Ziegler E, Bennet-Gates D (1999) Personality development in individuals with mental retardation. In: Vianello R, et al. (Eds.), Cambridge University Press, pp: 284.
-
Trucchia S (2011) Cognitive-behavioral therapy with the patient with mental retardation. Six-monthly magazine edited by students of the School of Specialization in Cognitive Psychotherapy and the Association of Cognitive Psychology 38.
-
Polat H, Karakaş SA (2021) The effect of acceptance and commitment therapy orientated anger management training on anger ruminations and impulsivity levels in forensic psychiatric patients: A randomized controlled trial. Perspectives in psychiatric care 57(4): 1616-1627.
-
Raffensperger MK (2009) Factors that influence outcomes for clients with an intellectual disability. British Journal of Guidance & Counselling 37(4): 495- 509
-
Ruiz FJ, Bianchi J, Bastidas-Suárez DM, Ramírez ES, Peña-Hernández V (2024) Is the AAQ-II that bad? Journal of Contextual Behavioral Science, pp: 100854.
-
Brinke LWT, Menting AT, Schuiringa HD, Deković M, Weisz JR, et al. (2021) Emotion regulation training as a treatment element for externalizing problems in adolescence: A randomized controlled micro-trial. Behaviour research and therapy 143: 103889.
- The Expanding Landscape of Road Rage: A Systematic Review of Conflicts Involving Drivers, Pedestrians, and Micromobility
- Validating Cognitive Models of Royal Navy Performance on Control Systems
- Comparing Standard and State-of-the-art Firefighter Coats on Postural Balance and Gait in a Live Burn Environment
- Investigating the Integration of Telemedicine into Clinicians Workflow: A Review of Methods
- Risk Assessment of Ergonomic Factors in a Textile Firm by RULA, REBA and Fine Kinney Methods
- Impact of Self-Esteem Training on Individuals with Disabilities Aged 17-30