Occupational Ergonomic and Safety Assessments Survey at Various Blacksmith Shops in Jeddah City
Purpose: Determine risk factor exposure and prevalence of musculoskeletal disorder (MSD) symptoms among blacksmiths in Jeddah City, Saudi Arabia, and environmental exposures to noise and particulate matter. Methods: 36 blacksmiths completed a modified Nordic Musculoskeletal Questionnaire for MSD symptoms, frequently performed tasks were assessed for MSD risk factors using the Rapid Upper Limb Assessment (RULA), and blacksmith work environments were monitored for noise and particulate matter. Results: Blacksmiths reported high prevalence for MSD symptoms in the past 12-months (neck 67%, wrists/hands 78%, lower back 86%, knees 67%, ankles/feet 86%). RULA indicated frequent tasks had moderate to high magnitudes of risk factor exposure. 8-hour time weighted noise exceeded OSHA thresholds, whereas particulate matter exceeded World Health Organization recommended levels. Conclusion: Blacksmith workers in Saudia Arabia are exposed to environmental hazards, risk factors for MSDs, and have elevated MSD symptom prevalences. Interventions are necessary to reduce exposures to musculoskeletal and environmental hazards.
Introduction
Occupational disorders are becoming increasingly growing over time among the workforce worldwide. Worldwide, about 1.71 billion individuals suffer from musculoskeletal disorders and 149 million of years lived with disability [1]. Frequent injuries negatively influence productivity due to the increased absenteeism. The costs of productivity loss per individual were estimated to be €343/workday due to absenteeism and €227/workday due to work assessment allowance and disability pension in Norway [2]. Work-related musculoskeletal disorders (WMSDs) are common among workers who perform manual jobs and commonly affect the lower back, neck, shoulder, and upper limbs. The WMSDs are linked to biomechanical loading mainly due to the manual material handling, upper limb repetitive movements, as well as awkward postures [3].
Besides the WMSD problems, working in a noisy environment can lead to hearing problems. It has been estimated that 16% of all disabling hearing loss among adults worldwide stems from occupational noise exposure [4]. Additionally, a review by Fang SC, et al. [5] found strong evidence for a relationship between occupational particulate exposures and heart rate variability as well as systemic inflammation. Worldwide, about one million individuals are prone to the risk of death from cardiovascular disease annually as a result of exposure to particulate air pollution [6].
Working in blacksmith shops involves various manual tasks such as welding, drilling, clipping, saw cutting, hammering, heating metals in the furnace, and sketching out new order designs. The blacksmith job also involves exposure to various WMSD risk factors, including heavy lifting, forceful exertions, awkward body postures, and prolonged standing hours [7, 8, 9, 10]. Akter S, et al. [7] found a high prevalence (85%) of WMSD symptoms among metalworkers in Bangladesh, with the upper back and lower back demonstrating the highest (65%) discomfort ratings. Ajayeoba AO, et al. [8] found 86% and 64% of metalworkers in Nigeria who perform blacksmithing and welding activities reported discomfort in one or more body regions during the last 12 months and the last 7 days, respectively, where the lower back had the highest (63%) discomfort rating, whereas Sumaila FG, et al. [9] reported 68% of the blacksmiths in Nigeria reported WMSD symptoms for the shoulder (40%) and lower back (29%). A later study by Susihono W, et al. [11] indicated welders reported WMSD symptoms in numerous body parts, including the upper neck (88%), waist (84%), right shoulder (82%), left shoulder (76%), right knee (70%), right calf (70%), left knee (68%), left calf (68%), buttocks (64%), and lower neck (62%). Collectively, these studies have demonstrated elevated WMSD symptoms to multiple body parts among workers performing blacksmith tasks in several countries.
Air pollution accounted for 4 million to 9 million death cases annually and more than one hundred million lost years due to the disease burden observed in low to middle-income countries [12, 13, 14, 15]. Particulate matter (PM), considered a common source of air pollution, consists of micro-size solid and/or liquid particles suspended in the air. Sources of PM include industrial activities [16], and the iron and steel industries [17]. The World Health Organization (WHO) [14] reported strong evidence for causal relationships between exposure to PM2.5 and all-cause mortality, acute respiratory diseases, chronic obstructive pulmonary disease, ischemic heart disease, lung cancer, and stroke.
Blacksmith shop environments are rich in toxic substances and unhealthy welding fumes. Occupational exposure to metal fumes with aerodynamic diameters such as PM2.5, which may negatively impact human health, especially the cardiovascular and renal systems. Table 1 shows the WHO exposure guidelines reference standards for the particles [14]. For highly polluted areas, the WHO suggested interim targets, which are pollutant levels above the WHO Air Quality Guidelines (AQGs), that authorities in such areas can target to achieve by implementing the proper changes to reach to the AQGs levels gradually within doable timeframes (Table 1). Chuang et al. showed that an 8-h mean PM2.5 was 50.3μg/m3 resulting from welding fumes [18], and concluded that exposure to such heavy metals in PM2.5 increases the risk of renal injury among welding workers. A later study by Lai CY, et al. [19] showed that inhaling metal fume PM2.5 could increase the risk of cardiovascular toxicity among welding workers, where ass concentrations for metal fume PM10 (<10μm), PM2.5, and PM0.1 were 899, 755, and 81μg/m3, respectively [19]. Another study showed that exposure to welding PM2.5 resulted in an acute decline in heart rate variability [20].
| Pollutant | Averaging Time | Interim Target | 2021 AQGs | |||
|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | |||
| PM (μg/m3) 2.5 | Annual | 35 | 25 | 15 | 10 | 5 |
| 24-hour | 75 | 50 | 37.5 | 25 | 15 | |
| PM (μg/m3) 10 | Annual | 70 | 50 | 30 | 20 | 15 |
| 24-hour | 150 | 100 | 75 | 50 | 45 |
Table 1: World Health Organization guidelines for PM2.5 and PM10 concentration exposures [14].
Note: AQGs = Air Quality Guidelines. Table 1: World Health Organization guidelines for PM2.5 and PM10 concentration exposures [14].
Noise is another environmental hazard at workplaces that can result in an increased risk of noise-induced hearing loss (NIHL). Zhou J, et al. [21] reviewed occupational NIHL cases in China and reported that NIHL cases were about 55% [22], >80% [23], and 61% [24] for workers exposed to noise from forging, welding (automobile tire industry), and welding (steel industry) tasks, respectively. The noise levels ranged between 92 dB to 100 dB, which exceeds the U.S. Occupational Safety and Health Administration (OSHA) permissible exposure of 90 dB for the 8-hour Time Weighted Average (TWA). A growing body of evidence suggests that the exposure to noise more than 80-85 dB also increases the risk of cardiovascular disease [25, 26, 27].
The prior research regarding safety and health aspects of the blacksmith industry across various countries indicates that blacksmith workers are at increased risk of WMSD symptoms and elevated exposure to environmental factors such as noise and airborne toxic substances from tasks such as welding, increasing the risk of occupational injuries and illnesses. The blacksmith industry is a major industry in Saudi Arabia, where the workers work long hours performing various tasks such as welding and forging. This industry is also highly unregulated in terms of workplace safety and health. While research has shown elevated exposures to WMSD and environmental factors that may increase the risk of injuries and illnesses to blacksmiths in other countries, it is unclear if this is the current situation in the blacksmith industry in Saudi Arabia. As such, the objectives of this research were to document the prevalence of WMSD symptoms among blacksmith workers, evaluate WMSD risk factors for common blacksmith tasks, as well as assess environmental workplace exposures to noise and particulate matter resulting from the various blacksmith tasks in small to medium workshops in Jeddah City, Saudi Arabia. Findings from this exposure assessment research may provide insight into current levels of exposure to factors that may be harmful to the health of blacksmiths in Saudi Arabia and if warranted, bring attention to worker safety and health needs in this industry.
Methods
Participants
Sixty-five blacksmith workers in the north industrial city in Jeddah were approached to participate in this study, where 36 male blacksmiths from six blacksmith shops voluntarily agreed to participate. To qualify for participation, blacksmiths must have worked in this career for at least 12 months and not have had WMSD symptoms from previous accidents not related to their job as a blacksmith.
Materials
The body mass (without shoes) of each participant was measured using a weight scale and each participants height was measured using a stadiometer. An informed consent form approved by the University of Jeddah Bioethics Committee of Scientific and Medical Research (#UJ-REC-103) was reviewed with each participant which included an explanation of the role of their participation and the study’s purpose and objectives. Upon accepting inclusion in the study, participants were asked to sign a consent form. A modified Nordic Musculoskeletal Questionnaire (MSQ) [28, 29] was made available online and utilized to evaluate the WMSD symptoms and the potential risk factors among blacksmiths. With the assistance of the one of the investigators (e.g., making sure the participants understood all the questions) each participant completed an online version of the modified Nordic MSQ using an iPad.
A smartphone video recorded the blacksmith shops and workers while they performed various tasks. The blacksmiths’ awkward body postures used for postural analysis were snapshots from the recorded videos. A freely available motion analysis software Kinovea (version 0.8.15) was utilized to measure blacksmith body parts’ angles. The Rapid Upper Limb Assessment (RULA) assessment method [30] was utilized to assess the WMSD risk level associated with the various blacksmith tasks. A cloud-based ErgoPlus© software on a Windows 10 laptop analyzed the awkward postures using RULA [30].
Postural Assessment
RULA is a validated [31, 32, 33] ergonomic assessment method that was used to examine the exposure to WMSD risk factors involved in various blacksmith tasks. The tasks of welding, drilling, and clipping were selected for assessment as they were most frequently performed daily (as identified by the participants) and involved awkward body postures. The various RULA postural scores helps an analyst to identify the most extreme body postures with the largest loadings while performing the work tasks. Based on the RULA final score, the assessment suggests the next steps. RULA final scores of 1-2 indicate a negligible risk, and thus, the body postures are acceptable if not maintained for an extended period. RULA final scores of 3-4 indicate a minimal risk and further investigation and interventions may be required to correct the body posture. RULA final scores of 5-6 indicate a moderate risk, which further indicates that the tasks are to be investigated soon, and necessary changes need to be made quickly to control the risks associated with performing the job. Finally, a RULA final score of 7 indicates that the job is associated with a high risk, which requires further investigation, and necessary changes should be made immediately [30].
Workshops’ Environmental Assessment
The blacksmith workshops’ air quality was assessed by measuring the concentration levels of particulate matter PM2.5 and particulate matter PM10 using a portable Temtop® (Elitech Technology, Inc., Model M2000, USA) air quality monitor. The monitor, which stores concentration magnitudes once every minute, was held next to welding workstation for 10 minutes at three workshops to evaluate short-term exposures.
Assessment of the occupational noise exposure generated from the blacksmith tasks (such as iron cutting and forging) was performed using the VLIKE LCD Digital Audio Decibel Meter device (VLIKE, Model VL6708, China). The U.S. OSHA standard for permissible daily noise exposure is tabulated in Table 2. A-weighted (i.e., similar to the ear’s response) maximum sound levels were measured near the operations of welding, saw cutting, and forging. The measurements were conducted at the three workshops and lasted for 5 minutes for each assessed operation in each workshop. Since noise exposure was composed of three sources of noise (i.e., welding; saw cutting; forging) at different levels, the total noise dose (D) over the workday was estimated using Equation 1:
$$ D = 1 0 0 \left(\frac {C _ {1}}{T _ {1}} + \frac {C _ {2}}{T _ {2}} + \frac {C _ {n}}{T _ {n}}\right) $$
(1) OSHA)
1 2 100 n
1 2 Where Cn indicates the total exposure time at a specific noise level, and Tn indicates the reference duration for that level as given in Table 2. The reference duration (T) was estimated using Equation 2:
$$ T = \frac {8}{2 ^ {(L - 9 0) / 5}} \tag {2} $$
Where L is the measured A-weighted sound level. After
computing the noise dose (D), the 8-hour TWA, in decibels,
was computed using Equation 3:
( ) 10
1 6.61 log
$$ T W A = 1 6. 6 1 \times \log_ {1 0} \left(\frac {D}{1 0 0}\right) + 9 0 \tag {3} $$
Data Analysis
Descriptive statistics (mean and SD) were used to describe the participants’ demographic and anthropometric information (i.e., age, weight, and height). The modified Nordic MSQ survey responses were summarized as frequencies (i.e., number of participants who responded to each survey question) and percentages. Means (standard deviation) of the measured PM2.5 and PM10 concentrations were estimated for each workshop and compared to the 24-hour averaging time concentrations shown in Table 1. The estimated TWA sound levels were compared to the U.S. OSHA permissible 8-hour TWA daily noise level limit shown in Table 2. TWA values greater than the threshold of 90 dB were considered unsafe working environment that poses the risk of NIHL.
| Daily Exposure Duration (Hrs) | Exposure Limit (dB) |
|---|---|
| 8 | 90 |
| 6 | 92 |
| 4 | 95 |
| 3 | 97 |
| 2 | 100 |
| 1½ | 102 |
| 1 | 105 |
| ½ | 110 |
| ¼ or less | 115 |
Table 2: US OSHA standards for permissible daily noise exposure.
Results
Modified Nordic Musculoskeletal Questionnaire
The mean (SD) of the 36 participants’ age, body weight, and height were 40.0 (7.6) years, 79.3 (13.0) kg, and 166.8 (5.7) cm, respectively. The participants reported having 13.0 (9.1) years of working experience and worked an estimated 66.3 (7.7) hours per week.
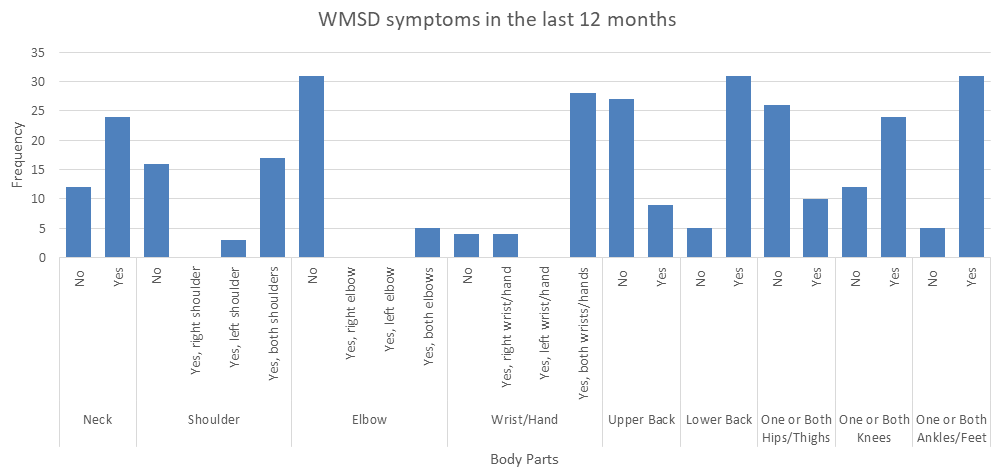
During the past 12-months (Table 3, Figure 1) many participants reported they suffered from pain/discomfort in the lower back (86%), ankles/feet (86%), both hands (78%), neck (67%), knees (67%), and shoulders (47%). A few participants reported that they were prevented from performing their normal activities either at work or home in the past 12-months due to the pain/discomfort in the lower back (22%), ankles and feet (14%), knees (8%), neck (6%), and shoulders (6%) (Table 4), whereas very few participants (3% for shoulder, lower back and one/both ankles) reported that their normal activities were limited due to the WMSD symptoms in the last 7 days (Table 5).
Have you at any time in the last 12 months had trouble (ache, pain, discomfort, numbness) in:
Body Part Response Frequency (%)
Shoulder
Neck No 12 33%
Yes 24 67%
No 16 44%
Yes, right shoulder 0 0%
Yes, left shoulder 3 8%
Yes, both shoulders 17 47%
| Elbow | No | 31 | 86% |
|---|---|---|---|
| Yes, right elbow | 0 | 0% | |
| Yes, left elbow | 0 | 0% | |
| Yes, both elbows | 5 | 14% | |
| Wrist/ Hand | No | 4 | 11% |
| Yes, right wrist/hand | 4 | 11% | |
| Yes, left wrist/hand | 0 | 0% | |
| Yes, both wrists/hands | 28 | 78% | |
| Upper Back | No | 27 | 75% |
| Yes | 9 | 25% | |
| Lower Back | No | 5 | 14% |
| Yes | 31 | 86% | |
| One or Both Hips/ Thighs | No | 26 | 72% |
| Yes | 10 | 28% | |
| One or Both Knees | No | 12 | 33% |
| Yes | 24 | 67% | |
| One or Both Ankles/Feet | No | 5 | 14% |
| Yes | 31 | 86% |
Table 3: Participants reporting WMSD symptoms in the last 12 months.
- Have you at any time during the last 12 months been prevented from doing your normal work (at home or away from home) because of the trouble?
- Body Part
- Response
- Frequency (%)
- Neck
- No
- 34
- 94%
- Yes
- 2
- 6%
- Shoulder
- No
- 34
- 94%
- Yes
- 2
- 6%
- Elbow
- No
- 36
- 100%
- Yes
- 0
- 0%
- Wrist/Hand
- No
- 36
- 100%
- Yes
- 0
- 0%
- Upper Back
- No
- 36
- 100%
- Yes
- 0
- 0%
- Lower Back
- No
- 28
- 78%
- Yes
- 8
- 22%
- One or Both Hips/Thighs
- No
- 36
- 100%
- Yes
- 0
- 0%
- One or Both Knees
- No
- 33
- 92%
- Yes
- 3
- 8%
- One or Both Ankles/Feet
- No
- 31
- 86%
- Yes
- 5
- 14%
Table 4: Participants reporting WMSD symptoms affecting their job in the last 12 months.
- Have you at any time during the last 7 days been prevented from doing your normal work (at home or away from home) because of the trouble?
- Body Part
- Response
- Frequency (%)
- Neck
- No
- 36
- 100%
- Yes
- 0
- 0%
- Shoulder
- No
- 35
- 97%
- Yes
- 1
- 3%
- Elbow
- No
- 36
- 100%
- Yes
- 0
- 0%
- Wrist/Hand
- No
- 36
- 100%
- Yes
- 0
- 0%
- Upper Back
- No
- 36
- 100%
- Yes
- 0
- 0%
- Lower Back
- No
- 35
- 97%
- Yes
- 1
- 3%
- One or Both Hibs/Thighs
- No
- 36
- 100%
- Yes
- 0
- 0%
- One or Both Knees
- No
- 35
- 97%
- Yes
- 1
- 3%
- One or Both Ankles/Feet
- No
- 35
- 97%
- Yes
- 1
- 3%
Table 5: Participants reporting WMSD symptoms affecting their job in the last 7 days.
During the last 12-months (Table 6) some participants reported pain/discomfort for duration of 8-30 days in the knees (28%), shoulders (22%), wrists/hands (22%), neck (17%), lower back (14%), hips/thighs (14%), upper back (11%), ankles/feet (11%), and elbows (6%). However, many participants also reported lower back (72%), wrist/ hand (67%), ankles/feet (64%), and neck (50%) pain/ discomfort for more than 30 days (but not every day) during the last 12-months, and one participant indicated he is experiencing shoulder pain/discomfort every day. Finally, three participants responded that they experience ankles/ feet pain/discomfort every day and related this to prolonged standing while working.
| Body Parts | Length of time that you have had trouble during the last 12 months? | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 0 days | 1-7 days | 8-30 days | More than 30 days, But Not Every Day | Every Day | ||||||
| N | (%) | N | (%) | N | (%) | N | (%) | N | (%) | |
| Neck | 12 | 33% | 0 | 0% | 6 | 17% | 18 | 50% | 0 | 0% |
| Shoulder | 16 | 44% | 0 | 0% | 8 | 22% | 11 | 31% | 1 | 3% |
| Elbow | 31 | 86% | 1 | 3% | 2 | 6% | 2 | 6% | 0 | 0% |
| Wrist/Hand | 4 | 11% | 0 | 0% | 8 | 22% | 24 | 67% | 0 | 0% |
| Upper Back | 27 | 75% | 0 | 0% | 4 | 11% | 5 | 14% | 0 | 0% |
| Lower Back | 5 | 14% | 0 | 0% | 5 | 14% | 26 | 72% | 0 | 0% |
| One or Both Hibs/Thighs | 27 | 75% | 2 | 6% | 5 | 14% | 2 | 6% | 0 | 0% |
| One or Both Knees | 12 | 33% | 1 | 3% | 10 | 28% | 13 | 36% | 0 | 0% |
| One or Both Ankles/Feet | 5 | 14% | 1 | 3% | 4 | 11% | 23 | 64% | 3 | 8% |
Table 6: Duration of WMSD symptoms during the last 12 months.
Postural Assessment
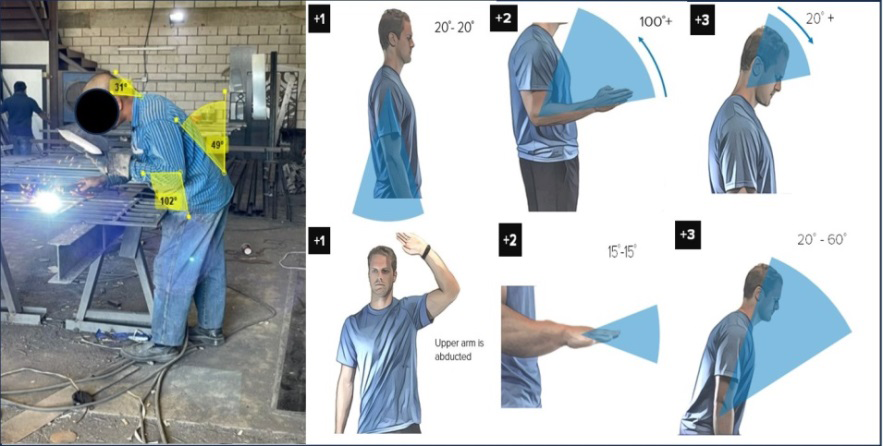
The results of the RULA postural evaluation while blacksmiths performed three of the more frequently performed tasks (i.e., iron welding, sheet metal drilling, iron clipping) are shown in Figures 2-4. The assessment of the welding task (Figure 2), left side assessment, resulted in a final RULA score of 6, which indicates poor body postures adopted by the blacksmith, and thus, investigation for the reasons for poor postures and changes are required soon. While performing the welding task, the lower arm of the blacksmith was elevated 102°, the neck was flexed forward 31°, and the torso was flexed forward 49°. The force load was rated as < 2kg since the blacksmith was holding a lightweight hand-held welding face shield.
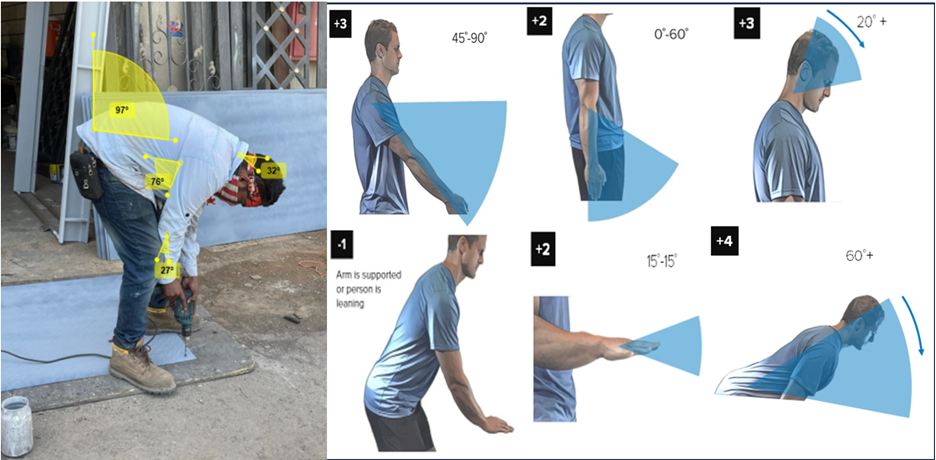
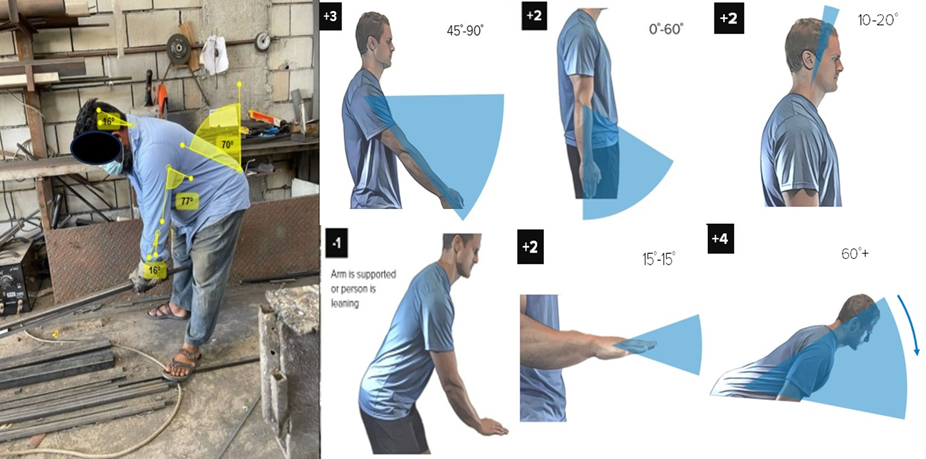
Assessment of both sheet metal drilling (right side assessment) and iron clipping (left side assessment) tasks showed a final RULA score of 7, which indicates that the awkward body postures adopted by the blacksmiths could increase the exposure to WMSD risk factors, and thus, workplace interventions are required to be implemented immediately to reduce or eliminate the exposure. For the sheet metal drilling task (Figure 3), the upper arm was away from the torso at an angle of 76°, the neck was flexed 32°, and the torso was flexed 97°. The force load was rated as between 2 kg to 10 kg as the drill utilized by the blacksmith was 3 kg. Finally, for the iron clipping task (Figure 4), the upper arm was away from the torso at an angle of 77°, the neck was flexed 16°, and the torso was flexed 70°. The blacksmith rated the applied force to operate the clipping equipment as about 9 kg, and thus, the force load was between 2 to 10 kg. The awkward body postures adopted by the blacksmiths in the three assessed tasks were repeated more than four times per minute.
Workshop Environmental Assessment
Air quality measurements results from near the welding stations at the three workshops are shown in Table 7. The measured PM2.5 and PM10 at the three workshops exceeded the WHO 2021 AQG for the 24-hour concentrations exposure (15 μg/m3 for PM2.5, 45 μg/m3 for PM10), indicating that blacksmith workers are exposed to unhealthy PM concentrations.
| PM | Workshop 1 | Workshop 2 | Workshop 3 |
|---|---|---|---|
| PM2.5(μg/m3) | 55.93(12.90) | 53.47(11.65) | 65.33(14.64) |
| PM10(μg/m3) | 59.33(12.64) | 62.20(10.38) | 73.20(13.96) |
Table 7: Mean (SD) particulate matter (PM) concentrations at various shops.
Sound level measurements for welding, saw cutting, and forging tasks at the three workshops are shown in Table 8. The daily exposure time to each task was defined by the blacksmiths performing the task during the measurements.
The TWA sound levels at each of the workshops exceeded the U.S. OSHA permissible 8-hour TWA noise level limit of 90 dB.
| Tasks | Variables | Workshop 1 | Workshop 2 | Workshop 3 |
|---|---|---|---|---|
| Welding | A-weighted sound level, L (dB) | 98.7 | 92.4 | 97.2 |
| Exposure time, C (hr) | 3.3 | 2.5 | 2.84 | |
| Reference time, T (hr) | 2.39 | 5.74 | 2.95 | |
| Saw Cutting | A-weighted sound level, L (dB) | 130.4 | 109.8 | 131 |
| Exposure time, C (hr) | 3 | 2.5 | 4.8 | |
| Reference time, T (hr) | 0.03 | 0.51 | 0.03 | |
| Forging | A-weighted sound level, L (dB) | 103.2 | 101.4 | 106.5 |
| Exposure time, C (hr) | 0.75 | 0.66 | 1 | |
| Reference time, T (hr) | 1.28 | 1.65 | 0.81 | |
| Dose, D | 10343.6 | 570 | 17863.4 | |
| TWA (dB) | 123.5 | 102.6 | 127.4 |
Table 8: Noise level measurements at various workshops.
Discussion
Tasks performed by blacksmiths has been shown in different world-wide regions to result in exposures to awkward body postures and environmental exposures of noise and particulate matter that may increase the risk of musculoskeletal disorders and compromise the workers’ health. The main findings from this assessment of blacksmith tasks in Saudi Arabia indicate that workers work long hours, they are exposed to elevated environmental exposures of noise and particulate matter from commonly performed blacksmith tasks, and experience elevated body part discomfort in several body regions likely due to awkward body postures. Body Part Discomfort As observed in the current study after assessing the three more frequently performed tasks including iron welding, sheet metal drilling, and iron clipping tasks, the workers adopted severe trunk forward flexion ranging between 49° to 97°, which likely contributed to the high prevalence of lower back pain/discomfort (86%) among blacksmiths. Previous studies on blacksmiths reported comparable lower back pain/discomfort prevalence of 65% [7] and 63% [8]. Another study by Sumaila FG, et al. [9] showed a lower prevalence (29%) of lower back pain/discomfort, but a comparable prevalence of shoulder pain/discomfort (40%) to that reported in the current study (55%). Epidemiological evidence supports the relationship between working with torso flexion and low back pain/disorders as Punnett L, et al. [34] found low back disorder cases were about seven times more likely (OR=6.7, 95% CI: 1.6-20.4) than non-cases to work with severe torso flexion (>45 °), whereas workers who adopted extreme torso flexion (≥60°) for more than 5% of the working time were 47% more likely to be at increased of low back pain [35].
The findings of this current study also revealed that the recruited blacksmiths reported an elevated prevalence of pain/discomfort in the lower extremities. The prevalence of discomfort anytime in the last 12-months in one or both knees and in one or both ankles/feet was 67% and 86% respectively, and 64% of the blacksmiths reported trouble with one or both ankles/feet more than 30 days but not every day. These findings are comparable to the prevalence reported by Susihono’s W, et al. [11] for welders’ right knee (70%) and left knee (68%), Pandit S, et al. [36] who found a somewhat lower prevalence (40.6%) of ankle/feet discomfort, and Ajayeoba AO, et al. [8] who found approximately 40% and 30% of welders reported MSD discomfort for the knees and ankles, respectively, during the last 12-months. The current study findings on lower extremity pain/discomfort, however, are in contrast with findings from other studies on metal workers, where Akter MZ, et al. [7] found knee and ankle prevalence of musculoskeletal symptoms in the previous 12-months of 33.3% and 9% for the knee and ankle, respectively. As shown in Figures 2-4 for the posture analysis, blacksmith tasks are often performed in standing positions. Prior epidemiological research has found that increasing duration of standing is highly associated with lower leg or calf pain, especially for those who stand at work without freedom to sit down [37], and increased risk for plantar fasciitis results with increased time spent standing on hard surfaces [38]. The blacksmiths in this current study worked a self-reported average of 66.3 hours per week. Although not specifically documented, given the elevated number of hours worked per week, it is possible that standing while performing the blacksmith tasks over the long duration workweeks may have contributed to the elevated prevalence of knee and ankle pain/discomfort reported by the blacksmiths in this study.
Elevated prevalence of pain/discomfort was also reported for the neck by the blacksmiths in this study, where 67% reported neck pain/discomfort in the past 12 months and 50% indicated they had neck musculoskeletal symptoms more than 30 days (but not every day) in the past 12-months. These findings are consistent with the prevalence of neck WMSD symptoms found by other researchers in blacksmiths, metal workers and welders, ranging from 20% to 88% in the past 12-months ([11]: welders, upper neck 88%; [8]: blacksmiths, ~20%; welders, ~30%; [7]: metal workers: 33.3%; [39]: German welders: 71%). From the RULA analyses, the neck was in flexion greater than 20° for the iron welding (Figure 2) and sheet metal drilling (Figure 3) tasks, and between 10° to 20° for the iron clipping task (Figure 4). Neck flexion, either static or repetitive, has been associated with neck pain in previous epidemiological reviews. Ariens GA, et al. [40] found some evidence of positive relationship of neck flexion with neck pain, and Palmer KT, et al. [41] found moderate evidence of static loading of neck-shoulder musculature in combination with repetition and neck flexion increases risk of neck pain, and suggestive evidence that static loading of the neck-shoulder musculature makes an independent contribution. Specific to metal working and welding, in a systematic review of WMSD symptoms among welding/metal fabrication workers, median neck flexion was associated with neck pain in the previous year [42]. Shahriyari M, et al. [43] also found median neck flexion (18.6°) was significantly associated with neck pain in welders with symptoms during past year (prevalence of 46.7%), and pain was characterized by significantly more awkward postures and percentage of time spent with neck flexed more than 20°. Collectively, the elevated prevalence of neck WMSD symptoms is consistent with prior findings from other studies, and it is likely that static or repeated neck flexion contributed to this elevated prevalence. Awkward joint postures, such as torso flexion and neck flexion, can be dictated by the design of the welding and metal working tasks and workstations. Thus, as suggested by Suman D, et al. [44], welding workstations should be adjustable to permit more neutral working postures of the head, neck, arms, and torso. A study of Susihono W, et al. [11] reported the prevalence of right wrist and right hand pain/discomfort of welders to be 52% and 48%, respectively. On the other hand, the current study findings showed a higher prevalence (78%) of both wrists/hands pain/discomfort. That could be attributed to the blacksmith tasks exposing workers to wrist/hand loadings due to repetitive flexion/extension (15°-15°) (e.g., iron welding, sheet metal drilling, and iron clipping), lifting heavy metals, forceful exertions (e.g., iron clipping task), vibration (e.g., sheet metal drilling), and extended working hours. The tasks examined by Susihono W, et al. [11] were welding tasks only, which might explain the relatively lower prevalence. The findings from the study of Ajayeoba AO, et al. [8] showed a 100% prevalence of wrists/hands discomfort where related the musculoskeletal discomfort to the nature of blacksmith tasks including improper material handling, awkward postures, and forceful and repetitive activities. Khavanin SM [45] examined the musculoskeletal disorders of the upper limbs among steel industry workers who perform tasks such as steel handling, cutting, and tempering, among others. The highest prevalence of musculoskeletal disorders was found for right (85.6%) and left (83.9%) hands, right (74.4%) and left (77.8%) wrists, and left elbow (74.4%), where the author Khavanin SM [45] recommended redesigning the hand tools and workstation layout to reduce the forceful exertions. They also suggested implementing job rotation to reduce the exposure hours.
Postural Assessment
The RULA assessment of welding, sheet metal drilling, and iron clipping tasks resulted in final RULA scores of 6, 7, and 7, respectively. This suggests that the blacksmiths in the assessed shops might be at increased risk of WMSDs due to the awkward body postures while performing the various blacksmith tasks. As shown in Figures 2-4 , the awkward body postures included trunk flexion (49°-97°), neck flexion (16°-32°), upper arm flexion (20°-76°), lower arm flexion (16°-102°), and wrist/hand flexion/extension (15°-15°). A previous study Susihono W, et al. [11] reported a similar final RULA score (i.e., 7) for welding workers. Another study by Suman D, et al. [44] assessed the body postures of 10 workers while performing the welding task and found a final RULA score of 7 for seven workers and a score of 6 for three workers. These elevated RULA final scores in the current study suggest a great need for interventions particularly aimed at reducing awkward body postures during these tasks. Suman D, et al. [44] suggested using a height-adjustable welding table to improve the posture of the trunk, neck, and arms while performing the welding task. The reorientation of the working surface to face the worker might also be necessary to reduce or eliminate the awkward body postures. Finally, providing training and education to the blacksmiths could increase their awareness about the importance of adopting neutral body postures while performing the job tasks to reduce the loadings on the body parts, and thus, possibly reduce the WMSD symptoms.
Environmental Assessment
Particulate Matter: The PM2.5 and PM10 concentrations measured near the welding stations in three workshops in the current study ranged from 53.47 μg/m3 to 65.33 μg/m3 and 59.33 μg/m3 to 73.20 μg/m3, respectively, which exceeds the 2021 AQG by WHO for the 24-hour concentrations exposure. Similar findings were reported by Chuang KJ, et al. `[18] where they showed that the welding fumes resulted in an 8-h mean PM2.5 of 50.3μg/m3. Findings by Liu S [46] showed relatively lower metal fumes PM (ranging between 0.0338 μg/m3 to 27.8 μg/m3) generated from welding activities in three different factories. Lai CY, et al. [19] reported higher mass concentrations for welding fumes PM10 (899 μg/m3) and PM2.5 (755 μg/m3). The significant difference between concentration levels in [19] and those measured in the current study could be due to the number of active welding stations during the data collection. There were two active welding stations at most during the air quality measurements in the assessed workshops in the current study. Even though not mentioned, there could be more than two active welding stations during the measurements at the shipyard site by Lai’s colleague. It is worth noting that very few participants in the current study were wearing any protective masks that filter out the fine particles. It can be concluded that blacksmiths in the current study were exposed to high levels of particulate concentrations with minimal respiratory protection, and thus, could be at increased risk of renal injury [18], cardiovascular diseases [6, 19], and heart rate variability [5, 20]. It is recommended that workshop owners and managers provide masks (e.g., particulate respirators) that protect blacksmiths from unhealthy occupational particulates.
Noise Exposure Assessment: The findings from the current study showed that the 8-hour TWA noise levels from the welding, saw cutting, and forging tasks at the three assessed workshops ranged from 102.6 dB to 127.4 dB which exceeded the OSHA 8-hour TWA permissible exposure of 90 dB. Previous studies [19, 20, 21] showed a comparable noise level from forging and welding activities ranging between 92 dB to 100 dB. A study by Colucci D, et al. [47] reported slightly higher noise levels for metal forging and hammering tasks ranging between 120 dB to 140 dB. Another study by Aliyu S, et al. [48] reported a lower noise level (Lmax = 72.42 dB) measured in an iron work market, however, it was not specified which blacksmithing activities were measured. None of the participants in the current study were wearing hearing protection (e.g., earplugs, earmuffs). Given the elevated noise exposure levels (102.6 dB to 127.4 dB) and that none of the participants were wearing hearing protection, this suggests that the blacksmiths may be at elevated risk of auditory effects such as NIHL [21, 22, 23, 24] and other non-auditory effects such as cardiovascular disease [25, 26, 27] due to their continuous exposure to such high levels of noise.
Limitations
The findings of this study should be considered in light of several methodological limitations. First, although blacksmiths perform numerous tasks as part of their job, three of the most frequently performed tasks were assessed using RULA. These three frequently performed tasks all demonstrated moderate to high exposure to postural risk factors for WMSDs, thus, other less frequently performed tasks would be expected to add to already elevated WMSD risk factor exposures. Second, only three blacksmith workshops were sampled for particulate matter and noise. However, all three workshops monitored demonstrated magnitudes of particulate matter and noise exposure that exceeded maximum thresholds recognized by authoritative health agencies (i.e., WHO for particulate matter, U.S. OSHA for noise), suggesting potentially harmful environmental conditions for at least those three workshops. Finally, the participant pool consisted of only male blacksmiths when ascertaining the musculoskeletal discomfort prevalence. This is reflective of the gender mix of blacksmith in Saudi Arabia, which consists almost exclusively of males.
Conclusion
This study assessed musculoskeletal disorder symptoms, postural risk factors for musculoskeletal disorders, and environmental exposures to noise and particulate matter for blacksmith workers in Jeddah City, Saudi Arabia. Blacksmiths reported high prevalence for MSD symptoms in the past 12-months (neck 67%, wrists/hands 78%, lower back 86%, knees 67%, ankles/feet 86%), and postural risk factor assessments using RULA indicated the frequently performed blacksmith tasks of welding, drilling and clipping had moderate to high magnitudes of musculoskeletal disorder risk factor exposure. Blacksmith workers were also exposed to 8-hour TWA noise levels that exceeded U.S. OSHA thresholds, whereas particulate matter exposure exceeded World Health Organization recommended levels. These findings indicate blacksmith workers in Saudia Arabia are exposed to environmental hazards, risk factors for MSDs, and have elevated prevalence of MSD symptoms. The blacksmith workshop owners and managers are recommended to reorient the working surface for iron welding and sheet metal drilling tasks to face the workers, and thus, eliminate the extreme torso and neck flexion. Also, they are recommended to provide training and education sessions to guide the workers about safe working postures and practices. Additionally, adequate ventilation systems must be installed in the workshops to remove the contaminations resulting from the various blacksmith activities. It is recommended that workshop owners and managers provide high-quality particulate respirators and hearing protection gears to reduce exposures to environmental hazards. Future efforts might consider a larger sample size as well as assess more blacksmith tasks for potential MSDs risk factors and environmental hazards.
Ethical Approval
Ethical approval was obtained from the University of Jeddah Bioethics Committee of Scientific and Medical Research (Application#UJ-REC-103).
Conflict of Interest
The authors declare no conflict of interest.
Funding
This research received no external funding.
References
-
Cieza A, Causey K, Kamenov K, Hanson SW, Chatterji S, et al. (2006) Global estimates of the need for rehabilitation based on the Global Burden of Disease study 2019: a systematic analysis for the Global Burden of Disease Study 2019. The Lancet 396(10267): 2006-2017.
-
Killingmo RM, Tveter AT, Pripp AH, Tingulstad A, Maas E, et al. (2024) Modifiable prognostic factors of high societal costs among people on sick leave due to musculoskeletal disorders: findings from an occupational cohort study. BMJ Open 14(3): e080567.
-
Bonfiglioli R, Caraballo-Arias Y, Salmen-Navarro A (2022) Epidemiology of work-related musculoskeletal disorders. Current Opinion in Epidemiology and Public Health 1(1): 18-24.
-
Nelson DI, Nelson RY, Concha‐Barrientos M, Fingerhut M (2005) The global burden of occupational noise‐induced hearing loss. American Journal of Industrial Medicine 48(6): 446-458.
-
Fang SC, Cassidy A, Christiani DC (2010) A systematic review of occupational exposure to particulate matter and cardiovascular disease. International Journal of Environmental Research and Public Health 7(4): 1773- 1806.
-
Cohen AJ, Ross Anderson H, Ostro B, Pandey KD, Krzyzanowski M, et al. (2005) The global burden of disease due to outdoor air pollution. Journal of Toxicology and Environmental Health, Part A 68(13-14): 1301-1307.
-
Akter S, Maruf MZ, Chowdhury SK (2015) Prevalence of musculoskeletal symptoms and associated factors: a cross-sectional study of metal workers in Bangladesh. Work 50(3): 363-370.
-
Ajayeoba AO, Onawumi AS, Adebiyi KA, Olagunju TO, Oyediran DD (2016) Assessment of musculoskeletal disorders (MSDs) in workers in selected metalworking micro-enterprises (MMEs) in south-western Nigeria. Advances in Multidisciplinary scientific Research 2(2): 1.
-
Sumaila FG, Zakari MK, Radda MI (2018) Prevalence and pattern of work related musculoskeletal disorders among blacksmiths in Kurmi market, Kano: north- western Nigeria. World Scientific News 94(2): 149-162.
-
Tahmasebi R, Motamedzade M, Torkashvand S, Anbarian M, Olfatifar M, et al. (2019) Validity and reliability of the Persian version of the Dutch musculoskeletal questionnaire. Medical Journal of the Islamic Republic of Iran 33: 27.
-
Susihono W, Selviani Y, Dewi IA, Liswahyuningsih NL (2020) Advances in Social Science, Education and Humanities Research, Atlantis Press, Netherlands, pp: 270-276.
-
Burnett R, Chen H, Szyszkowicz M, Fann N, Hubbell B, et al. (2018) Global estimates of mortality associated with long-term exposure to outdoor fine particulate matter. Proceedings of the National Academy of Sciences 115(38): 9592-9597.
-
Vohra K, Vodonos A, Schwartz J, Marais EA, Sulprizio MP, et al. (2021) Global mortality from outdoor fine particle pollution generated by fossil fuel combustion: Results from GEOS-Chem. Environmental research 195: 110754.
-
World Health Organization (2018) Burden of disease from ambient air pollution for 2016.
-
World Health Organization (2021) WHO global air quality guidelines: particulate matter (PM2. 5 and PM10), ozone, nitrogen dioxide, sulfur dioxide and carbon monoxide.
-
Silva FMO, Alexandrina EC, Pardal AC, Carvalhos MT, Schornobay Lui E (2022) Monitoring and prediction of particulate matter (PM2. 5 and PM10) around the IPBeja Campus. Sustainability 14(24): 16892.
-
Zhang H, Sun W, Li W, Wang Y (2022) Physical and chemical characterization of fugitive particulate matter emissions of the iron and steel industry. Atmospheric Pollution Research 13(1): 101272.
-
Chuang KJ, Pan CH, Su CL, Lai CH, Lin WY, et al. (2015) Urinary neutrophil gelatinase-associated lipocalin is associated with heavy metal exposure in welding workers. Scientific Reports 5(1): 18048.
-
Lai CY, Lai CH, Chuang HC, Pan CH, Yen CC, et al. (2016) Physicochemistry and cardiovascular toxicity of metal fume PM2. 5: a study of human coronary artery endothelial cells and welding workers. Scientific Reports 6(1): 33515.
-
Fan T, Fang SC, Cavallari JM, Barnett IJ, Wang Z, et al. (2014) Heart rate variability and DNA methylation levels are altered after short-term metal fume exposure among occupational welders: a repeated-measures panel study. BMC Public Health 14: 1279.
-
Zhou J, Shi Z, Zhou L, Hu Y, Zhang M (2020) Occupational noise-induced hearing loss in China: a systematic review and meta-analysis. BMJ Open 10(9): e039576.
-
Zhang GY, Tang ZF, Yao YP (2012) A comparative study of high-frequency hearing impairment caused by noise from punching machine and steady state noise in workers. Chin J Occup Med 30(5): 356-358.
-
Wu L, Zhu ZC, LF Y (2009) Effects of welding dust and noise on hearing loss in workers. Chin Public Health 25: 75-76.
-
Chen XX, JY L, SS S (2009) Investigation on hearing impairment of workers under combined effects of welding smoke and noise. Chin J Occup Med 36: 87-88.
-
Pretzsch A, Seidler A, Hegewald J (2021) Health effects of occupational noise. Current Pollution Reports 7: 344- 358.
-
Teixeira LR, Pega F, Dzhambov AM, Bortkiewicz A, da Silva DT, et al. (2021) The effect of occupational exposure to noise on ischaemic heart disease, stroke and hypertension: A systematic review and meta-analysis from the WHO/ILO Joint Estimates of the Work-Related Burden of Disease and Injury. Environment International 154: 106387.
-
Bolm-Audorff U, Hegewald J, Pretzsch A, Freiberg A, Nienhaus A, et al. (2020) Occupational noise and hypertension risk: a systematic review and meta- analysis. International Journal of Environmental Research and Public Health 17(17): 6281.
-
Kuorinka I, Jonsson B, Kilbom A, Vinterberg H, Biering-Sorensen F, et al. (1987) Standardised Nordic questionnaires for the analysis of musculoskeletal symptoms. Applied ergonomics 18(3): 233-237.
-
Crawford JO (2007) The Nordic musculoskeletal questionnaire. Occupational medicine 57(4): 300-301.
-
McAtamney L, Corlett EN (1993) RULA: a survey method for the investigation of work-related upper limb disorders. Applied Ergonomics 24(2): 91-99.
-
Kee D (2020) An empirical comparison of OWAS, RULA and REBA based on self-reported discomfort. International Journal of Occupational Safety and Ergonomics 26(2): 285-295.
-
Kee D, Na S, Chung MK (2020) Comparison of the Ovako working posture analysis system, rapid upper limb assessment, and rapid entire body assessment based on the maximum holding times. International Journal of Industrial Ergonomics 77: 102943.
-
Kee D (2022) Comparison of LEBA and RULA Based on Postural Load Criteria and Epidemiological Data on Musculoskeletal Disorders. International Journal of Environmental Research and Public Health 19(7): 3967.
-
Punnett L, Fine LJ, Keyserling WM, Herrin GD, Chaffin DB (1991) Back disorders and nonneutral trunk postures of automobile assembly workers. Scandinavian Journal of Work, Environment & Health 1: 337-346.
-
Hoogendoorn WE, Bongers PM, De Vet HC, Douwes M, Koes BW, et al. (2000) Flexion and rotation of the trunk and lifting at work are risk factors for low back pain: results of a prospective cohort study. Spine 25(23): 3087-3092.
-
Pandit S, Thakur SK, Khalode TG, Aakriti, Sahu A, Kamble R (2022) Ergonomic Risk Assessment Among the Welders Working in Darbhanga District of Bihar. In: Deepak BBVL, et al. (Eds.), Recent Trends in Product Design and Intelligent Manufacturing Systems: Select Proceedings of IPDIMS 2021. Springer Nature, Singapore, pp: 71-76.
-
Messing K, Tissot F, Stock S (2008) Distal lower-extremity pain and work postures in the Quebec population. American Journal of Public Health 98(4): 705-713.
-
Werner RA, Gell N, Hartigan A, Wiggerman N, Keyserling WM (2010) Risk factors for plantar fasciitis among assembly plant workers. PM&R 2(2): 110-116.
-
Weyh C, Pilat C, Kruger K (2020) Musculoskeletal disorders and level of physical activity in welders. Occupational Medicine 70(8): 586-592.
-
Ariens GA, Van Mechelen W, Bongers PM, Bouter LM, Van Der Wal G (2000) Physical risk factors for neck pain. Scandinavian Journal of Work, Environment & Health 26(1): 7-19.
-
Palmer KT, Smedley J (2007) Work relatedness of chronic neck pain with physical findings-a systematic review. Scandinavian Journal of Work, Environment & Health 33(3): 165-191.
-
Chiboyiwa E, Ncube F, Erick PN (2020) Ergonomic risk factors associated with work-related musculoskeletal symptoms among welding and metal fabrication workers: a systematic review. International Journal of Human Factors and Ergonomics 7(4): 359-382.
-
Shahriyari M, Afshari D, Latifi SM (2018) Physical workload and musculoskeletal disorders in back, shoulders and neck among welders. International Journal of Occupational Safety and Ergonomics 26(4): 639-645.
-
Suman D, Kumar PP, Debamalya B, Shankarashis M (2021)Postural Analysis, Occupational Health, and Ergonomic Intervention of Welding Workers in Different Small-Scale Welding Units: A Report. In: Muzammil M et al. (Eds.), Ergonomics for Improved Productivity: Proceedings of HWWE 2017. Springer, Singapore, pp: 295-307.
-
Khavanin SM (2007) Work related musculoskeletal disorders of the upper limbs among steel industry populations. Acta Medica Iranica 45(5): 405-414.
-
Liu S (2010) Assessing exposures to particulate matter and manganese in welding fumes. University of California, Berkeley.
-
Colucci D (2020) Noise-Induced Hearing Loss Among Blacksmiths, Boilermakers, and Metal smiths. The Hearing Journal 73(1): 44-46.
-
Aliyu S, Tsamiya PS (2020) Evaluation of noise levels in Kara market Sokoto, Sokoto state, Nigeria. IOSR journal of applied physics 12(3): 56-61.
- The Expanding Landscape of Road Rage: A Systematic Review of Conflicts Involving Drivers, Pedestrians, and Micromobility
- Validating Cognitive Models of Royal Navy Performance on Control Systems
- Comparing Standard and State-of-the-art Firefighter Coats on Postural Balance and Gait in a Live Burn Environment
- Investigating the Integration of Telemedicine into Clinicians Workflow: A Review of Methods
- Risk Assessment of Ergonomic Factors in a Textile Firm by RULA, REBA and Fine Kinney Methods
- Impact of Self-Esteem Training on Individuals with Disabilities Aged 17-30