The Logistics of Production and Use of Blood and Blood Components
The logistics of the manufacturing and consumption of human blood and blood components: WHO has defined the most important steps as the need, the clinical demand and the supply to be organized in a national blood system with the blood services or blood establishments. The blood establishments provide the need, where the hospitals of health care institutions provide the patent care and establish the therapeutic demand. In the developing world, home to around 86% of the global population, the health care and blood transfusion support are in a development face supported by WHO guided and advised projects which include financing and human expert guidance. Cutting external foreign aid and guidance have dramatic effects on the outcome of the running projects and block progress.
Abbreviations
WHO: World Health Organisation; LMIC: Low-and Middle-Income Countries; QS: Quality System; PDs: Process Descriptions; SOPs: Standard Operating Procedures; EQAS: External Quality Assessment Schemes; PBM: Patient Blood Management.
Introduction
Blood collection in many Low-and Middle-Income Countries (LMIC) does not really align the clinical consumption. There are shortages but also surpluses because the calculated need of the consumers and the manufacturers may substantially differ.
Commentary
In those situations, the hospitals and the manufacturers are usually not adequately communicating with each other. Result may be an over requesting by the hospitals and an under supply of the hospitals, illustrating the gap in understanding and service provision between supplier (blood establishment) and consumer (hospital).
Logistics of Supply and Need
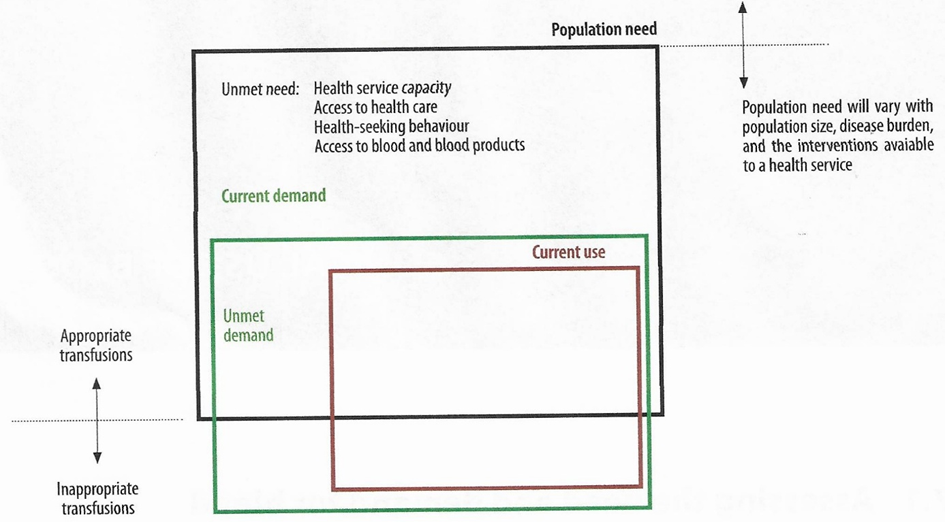
WHO has developed definitions to evaluate the differences between ‘need for, demand for, and use of blood’ [1]. These definitions and Figure 1, summarize current concepts on trying to measure the ‘need for, demand for, and use of blood’. Many factors influence the requirements for blood to meet the health care needs of a given population, as with all other treatment modalities. These include income levels, current status and rate of development of the health care and blood system, and accessibility of health care facilities to the public. Additionally, the ‘need for, demand for, and use of blood’’ in a given country could be affected by geography, population migration, and epidemiology of diseases for which blood or blood components are needed.
Need: An estimation of the amount of blood needed to meet the transfusion requirements of the patient population accord- ing to current policies, clinical guidelines and best practices.
Demand: The amount of blood that would be transfused if all prescriptions for blood were met. Demand may reflect appro- priate or inappropriate indications and practices.
Use: The actual amount of blood currently transfused; use may be appropriate or inappropriate.
In developed countries demographic change is likely to be one of the major drivers of long-term increases in blood needs and demands [2, 3]. It can be modelled by describing current blood use by age, and by applying the results to predictions of future population size and structure [4]. In developing countries, the introduction and implementation of new medical interventions and technologies like AI may also impact future blood requirements, but these are more difficult to predict and may in fact serve to reduce the need for blood transfusion as well as potentially increase it.
There is still no simple formula to provide reliable or useful estimates of the need and demand for blood in a national health system. A national assessment of blood demands and needs would usually be necessary for short- term or long-term national blood supply planning. For example, using a survey of a representative sample of hospitals, Drammeh et al. estimated that approximately 6.2 blood donations per 1000 population are needed in the United Republic of Tanzania [5]. This number is only slightly more than half of the 10 per 1000 population value that is used as a rough formula to provide reliable or useful estimates of the need and demand for blood in a national health system. A national assessment of blood needs and clinical education would usually be necessary for short-term or long-term national blood supply planning. This number is only slightly more than half of the 10 per 1000 population value that is used as a rough and general estimation for developing countries or LMICs. However, Mammen et al.
estimated that, based on the population, 26.2 million units (95% CI 17.9–38.0) of whole blood collections would need to be collected annually, equivalent to a donation rate of approximately 19.4 donations per 1000 population [6]. A different approach was used for the study, which included the determination of diseases and conditions requiring transfusion, estimation of the population at risk through a comprehensive literature review, and estimation of the percentage of people with diseases and conditions requiring transfusion and transfusion needed through the Delphi method. This study also identified a gap between need and demand (estimated at 13 million units of whole blood) and highlighted the importance of addressing the multifactorial factors and causes that lead to the existence of the gap [6].
However, in all countries, there is a need to monitor, evaluate and balance the supply of blood for requirements (clinical need and demand). Even in countries with mature and developed blood systems, the clinical demand for blood is not always met, and a range of initiatives is implemented to maintain or increase blood donations among the donor population. All blood establishments and hospital blood banks, to varying degrees, invest considerable time and resources in predicting demand for blood and adjusting donations. Shortages of blood, whether real or potential, have impacted all countries at differing times, including more recently during the global COVID-19 pandemic. In the early stages of the pandemic there were major concerns about a growing lack of availability of blood for transfusion due to the global social restrictions. Strategies and recommendations for responding to potential blood shortages must be incorporated into resilience planning for blood supply by countries and their blood establishments [7].
Blood Availability and Supply
The real need for blood products/components is difficult to measure directly and can be influenced by many factors. Using a population (/1000) blood donation rate as a general measure for blood availability, higher-income countries clearly have more blood products available for transfusion. The blood donation rate per 1000 population varies from 0.6 to 53. High-income countries collected 40% of the global donations while their population made up 16% of the global population [8]. However, population-based rates do not take into account availability and accessibility of blood products throughout the country and significant variability may exist, e.g., between urban and rural settings. Despite remarkable progress that has been made, the transfusion rates of blood components in developing countries are much lower than in developed countries. Correlated with the disparity of blood availability is the funding level and guarantee for blood centres. In general, funding per collection was higher in more economically developed countries with adequate annual health care, including transfusion, budgets. Strategies to improve blood collection and distribution in less economically developed countries (LMICs) need to be developed and effectively implemented as well as a stable voluntary and regular blood donor panel. The starting point of a safe, regular and sustainable blood supply is a stable population of regular voluntary non-remunerated blood donors. Globally, 82.8% of whole blood donations were collected from voluntary non-remunerated blood donors [1]. This proportion was 95.6% for high-income countries and 62.8% for low- income countries. However, repeat voluntary donations carry the least risk of infection. While the whole blood donation from repeat donors ranged from less than 0.1% to 100%, the median rate was 90% for European countries versus 20% to 56% for countries in the other five WHO regions. Although estimates of residual risk levels for TTIAs are not readily available, prevalence rates of TTIA markers are correlated with the level of residual risk. For HIV, HBV, HCV and syphilis agent markers, the prevalence rates for all four infections were lowest in high-income countries and highest in low-income countries [1].
Systematic screening and testing of donations for TTIA markers is an important step in reducing the risk of TTI diseases. The majority of countries have national policies for screening for major TTIAs (HIV, HBV, HCV and syphilis), though there are variations in details of screening policy and screening for additional TTIAs (such as Chagas disease, HTLV, malaria and West Nile fever, etc.), with a major reason being regional differences in infectious disease epidemiology. The effectiveness of TTIA screening can only be guaranteed with well designed and implemented quality assurance (QA) systems [1]. Two major components of a basic quality system (QS) are 1. the consistent and sustained use of process descriptions (PDs), standard operating procedures (SOPs) and a comprehensive documentation system. 2. participation in external quality assessment schemes (EQAS).
In low-income countries, only 76.2% of donations were screened following basic quality-assured procedures. Investing in establishing quality assurance programmes will be key to improving blood safety globally which is seriously hampered by the recent deliberate foreign aid and guidance cuts.
Clinal Demand for and Use of Blood and Blood Components
Differences in clinical transfusion practices between advanced and resource-poor countries are reflected in many aspects of transfusion practice. Most blood transfusions in low-income countries are still used for childbirth related complications and severe childhood anaemia, while in high-income countries transfusions are mostly given to support patients for surgery, critical illness and cancer treatment. The use of (frozen) fresh plasma is significantly less common in low-income countries than in high-income countries; the same applies to the use of platelet transfusions. Comprehensive data on patterns and the epidemiology of blood use in all countries, but specifically low-income countries, is needed to understand issues of demand, need and supply. One major aspect of uncertainty is blood use in acute injury and trauma in low- and middle-income countries, as well as in the advanced world, as illustrated in a recent systematic review [9].
Safe and effective clinical transfusion practices can be improved by hospital transfusion committees, providing critical local oversight of the transfusion process and more systematic patient-oriented education. The 2021 GSR data reported by 92 countries indicated that 48% of hospitals, where transfusion has been performed, reported having a hospital transfusion committee (HTC) of which 62% in high- income countries and only 25% in low-income countries. However, the status of these committees, whether dormant or active, has not been reported. The proportion of hospitals that have a reporting system for adverse transfusion events was heigher for resource-rich countries and lower for resource-poor countries. National haemovigilance programmes have increasingly been implemented, first for systematically monitoring and assessing the safety of the entire transfusion process and more recently also for measuring transfusion outcomes. Most of these structures were established in the absence of a well-developed quality sand documentation system. In 2018, 81% of countries in Europe had such a system propagated by the EU [10], while the percentage rates were lower for all other WHO regions. More research to improve the implementation of appropriate evidence-based manufacturing and utilization of blood products/components and the use of alternatives to transfusion will benefit the entire global transfusion community. Even though many resource-poor countries are still focusing on fundamental challenges, including blood availability and safety, security and sustainability of the blood supply remain an important issue for all blood services and operators. Appropriate and rational utilization of blood supported by patient blood management (PBM) programmes will help to decrease unnecessary blood transfusions and reduce transfusion risks and improve patient care and outcomes [11]. Strategies must address fundamental concerns about shortages and lack of availability of blood, for example how to treat severe life- threatening anaemia in children with malaria or to manage major blood loss in trauma and postpartum bleeding. This applies for all countries and especially low-resource countries.
The Use of Blood and Blood Components
There is evidence of significant differences in patterns of blood and blood component use between high-, middle-, and low-income countries (H-, M-, LICs).
Data reported to WHO before the foreign aid and guidance cuts indicated already significant differences in the age distribution of patients and the number of components transfused. In high-income countries, the most frequently transfused patient group is aged over 60 years, which accounts for up to 76 % of all transfusions. In low-income countries, up to 54% of all transfusions are for children under 5 years of age (most malaria anaemia), usually followed by females aged between 15 and 45 years (most obstetric bleeding).
Data from the 2021 WHO Global Status Report on Blood Safety and Availability (GSR) [1] on distribution of units of blood transfused in different clinical departments in hospitals or other transfusion performing healthcare facilities from 19 countries in the African Region showed that among 2 248 721 blood units transfused, 466 625 (21%) were transfused to patients in paediatrics departments, and 427 289 (19%) were transfused to patients in obstetrics and gynaecology departments In five of the 19 countries, more than 30% of blood was transfused to paediatric patients:
Democratic Republic of the Congo 60%;
Benin 58%;
Burkina Faso 39%;
Congo 33%;
Comoros 31%. [1]
Five countries reported that more than 30% of blood collected was transfused to gynaecological and obstetric patients:
Burkina Faso 61%;
Cameroon 55%;
Comoros 40%;
Eswatini 32%;
Burundi 32%.
Blood use for trauma and major bleeding varied considerably, although generally at lower rates than for patients in paediatrics, and obstetrics and gynaecology departments.
Similar data from the WHO African Region suggest that rates of usage in emergency and resuscitation departments in some countries approaches 23% (Madagascar) to 34 (Cabo Verde):
Madagascar 23%;
Gabon 26%;
Sao Tome and Principe 28%;
Cabo Verde 34%.
Also, these data indicate that children and women are the recipients who are most frequently transfused in low- income countries. However, it should be noted that these results are dependent on the accuracy of reporting and coding – e.g., in a number of LMI-countries it is possible and, in some situations, even likely that blood use in emergency departments is also covered by surgical departments.
One area that deserves special attention is the lingering lack of specific and up to date legislation covering the safety and quality of blood and blood products for transfusion in many countries. While 95% of European countries reported having such legislation, the proportions were only 51% in Africa, 52% in the Americas, and 56% in the Western Pacific. Appropriate and knowledgeable governance through a system of inspection and licensing is important for national blood availability and safety. Only 59% of countries had a system of regular inspection and licensing by the national regulatory agency, and only 33% of countries had an accreditation system for blood transfusion services.
Building up a system for inspection and licensing should be a priority for countries that do not currently have such programmes. Committed government support in funding, legislation and regulation of national blood services will be fundamental for achieving the progress needed to reach the goal of providing sustainably safe and sufficient blood to all patients who need blood transfusion. In this aspect, useful lessons could be learned from the experience in the European Union in ensuring sufficiency and access to safe blood products through implementing a harmonized legislative and up to date regulatory framework across all Member States [12]. In addition to the above overall concerns, specific challenges such as documentation and building a transparent database, related to the logistics of blood and blood product availability, blood safety and clinical transfusion practice are discussed in the following section.
The Importance of Clean and Transparent Data
The existence of a well-organized documentation and data collection and retrievable reporting system is an important element of a well-managed, nationally coordinated blood system. Having an adequate national database on blood availability and safety allows a country to set priorities and to further strengthen the national blood system:
- There is a need to establish systems of surveillance on the incidence and prevalence of HIV, HBV, HCV and other infections in blood donors and vigilance on the transfusion outcomes of recipients, including post- transfusion risk of infection.
- Information on clinical transfusion, including patterns of use by indication and department (epidemiology of transfusion), forms the basis for monitoring clinical transfusion practice and provides critical performance measures to influence desirable changes in the prescription and administration of blood and to reduce variations in transfusion practice.
- Information on lack of availability of blood to meet clinically justified need is not routinely collected but is an important measure of the effectiveness of the blood transfusion service.
- Countries providing partial and non-transparent data should consider instituting standardized systems for data collection and management at national level such as AI.
- National blood transfusion services need to provide greater structure and support for information management systems.
- Hospitals need to establish mechanisms for improving standardized data collection for the traceability and utilization of blood and for haemovigilance.
The introduction of AI with its deep and machine learning capacities might introduce a new era of development.
Conclusion
The issue of the logistics of an adequate blood availability (safe, effective, quality-assured) lies at the centre of the various challenges faced by the global blood transfusion medicine community. However, although with economic development, the currently low- and middle- income countries are expecting to experience growth of their national health care systems, there are unfortunately serious new challenges introduced through the deliberate foreign aid and guidance cuts imposed by advanced countries. Advances in health care – including increased accessibility for the population to health care and greater availability of treatment options – might likely bring an increased demand and need for clinical blood transfusion support.
An inadequate blood supply will impede the progress of the national health care. Different factors will be relevant to explain potential or actual shortages of blood donations in countries, for example due to lack of repeat donations from voluntary non-remunerated donors or the recent foreign aid cuts. In many resource-poor countries, inadequacy of blood supply already coexists with inadequate funding and less vigorous guidance, and weak government legislation and regulation.
Safe blood vein-to-vein chains depend on an effective TTIA screening system with strong quality and documentation systems, and quality management systems, and effective clinical adverse event monitoring mechanisms or national haemovigilance systems. The goal of achieving an adequate and secure blood supply vein-to-vein chain is of great significance, not only for the blood banking and transfusion medicine community but also for the overall public health of a nation.
Finally, the WHO GSR surveys continue to show significant variations in the availability, safety and use of blood and blood components between resource-rich and resource-poor countries. Despite progress in some areas there are still challenges, especially for resource-poor countries, in reaching the goal of providing sufficient, secure, effective, quality-assured and safe blood for all people who need blood transfusion. Vital to achieving that goal is:
- Improving the funding support for blood systems, establishing specific legislation, governance and developing national programmes for providing effective motivation of voluntary non-remunerated donors and regular blood collection services will be critical in order to continuously improve global blood availability and safety.
- Building quality assurance programmes for TTIA screening of donations will help to reduce residual TTI disease risks.
- Improving the safety and efficacy of clinical transfusions through the work of national haemovigilance systems and hospital transfusion committees should be a priority for all countries, especially resource-poor countries.
- Investing in improved systems for collecting data like AI on hospital-based blood transfusion, on transfusion safety and on blood utilization will in turn establish the foundations for building a global evidence-based approach to safe transfusion medicine practices in the future.
Unfortunately, the recent deliberate foreign aid and guidance cuts already show a destructive effect on the developmental programmes and progress of the health care and blood systems in the LMICs and will result in a dramatic loss in what globally has been initiated and achieved.
Dr. Yuyun Maryuningsih, Team Lead, Blood and Other Products of Human Origin of the former WHO Department of Health Product Policy and Standards (now Biological Norms and Standards, and Transplantation Team), strongly believes that this ‘2021 Global Status Report continues to recognize that inadequate and unsustainable financing (foreign aid cut) of blood services is a major factor that impedes efforts to improve blood safety in developing countries’. Governments are urged to ensure adequate, sustainable financing for national or regional blood programmes.
The financing mechanisms for blood systems and services should be integrated and strengthened within the financial structure of national health care systems. Countries with significant external donor funding (foreign aid) and support (guidance) should take proactive measures to mobilize domestic sources and reduce dependence on external funding and guidance to ensure the quality and sustainability of blood transfusion services in the future in order to guarantee adequate logistics of blood and blood component production and clinical use.
Conflict of Interest
The author has no conflicts of interest to disclose
Funding
No funds were received
References
-
(2022) Global Status Report on Blood Safety and Availability 2021.Geneva. World Health Organization.
-
Ehling M, Potzsch O (2010) Demographic changes in Germany up to 2060: consequences for blood donation. Transfusion Medicine and Hemotherapy 37: 131-139.
-
Greinacher A, Fendrich K, Alpen U, Hoffmann W (2007) Impact of demographic changes on the blood supply: Mecklenburg West Pomerania as a model region for Europe. Transfusion 47: 395-401.
-
Volken T, Buser A, Castelli D, Fontana S, Beat M, et al. (2018) Red blood cell uses in Switzerland: trends and demographic challenges. Blood Transfusion 16: 73-82.
-
Drammeh B, De A, Bock N, Pathak S, Juma A, et al. (2018) Estimating Tanzania’s national met and unmet blood demand from a survey of a representative sample of hospitals. Transfusion Medicine Reviews 32(1): 36-42.
-
Mammen JJ, Asirvatham ES, Lakshmanan J, Sarman CJ, Mani T, et al. (2021) National level estimation of population need for blood in India. Transfusion 61(6): 1809-1821.
-
Stanworth SJ, New HV, Apelseth TO, Brunskill S, Cardigan R, et al. (2020) Effects of the COVID-19 pandemic on supply and use of blood for transfusion. Lancet Haematology 7(10): e756-e764.
-
(2025) Blood Safety and Availability. WHO.
-
Yang L, Romano J, Marques CG, Uwamahoro C, Twagirumukiza FR, et al. (2020) Evaluation of blood product transfusion therapies in acute injury care in low- and middle-income countries: a systematic review. Injury 51(7): 1468-1476.
-
(2025) Directive 2002/98/EC of the European Parliament and Council of 27 January 2003 setting standards of quality and safety for collection, testing, processing, storage and distribution of human blood and blood components and amending Directive 2001/81/ EC. Official Journal of the European Union.
-
(2025) The urgent need to implement patient blood management: policy brief. Geneva: World Health Organization.
-
(2019) Evaluation of the Union legislation on blood, tissues and cells. Document SWD (2019) 375 final. Brussels: European Commission.
- How to Identify and Overcome Barriers in Developing Blood Systems?
- Why Was Transfusion Medicine Not Recognized as a Clinical Discipline?
- Outcomes of Lenalidomide Relapsed/Refractory Patients
- Is Transfusion Always Necessary?
- The Challenge for Component Therapies
- Effect of Monoclonal Gammopathy on Risk of Kidney Failure among Patients with Chronic Kidney Disease