Outcomes of Lenalidomide Relapsed/Refractory Patients
Lenalidomide constitutes a key component of therapeutic strategies for multiple myeloma (MM), both in combination with dexamethasone and as maintenance treatment. However, patients exhibit substantial heterogeneity in response and duration of benefit. In order to focus only on the benefit of Lenalidomide, we retrospectively analyzed 186 MM patients treated with doublet, lenalidomide–dexamethasone (n=158) and lenalidomide maintenance post-ASCT (n=18). Patients were stratified into five groups based on time to progression: primary refractory (PRMM), very resistant (VRMM), resistant (ResMM), initially sensitive (ISMM), and long-lasting responders (RALR). Median overall survival after lenalidomide (LenOS) varied markedly: PRMM 2 months, VRMM 8 months, ResMM 12 months, ISMM 39 months, and RALR 106 months (p
Abbreviations
MM: Multiple Myeloma; PRMM: Primary Refractory Multiple Myeloma; VRMM: Very Resistant Multiple Myeloma; ResMM: Resistant Multiple Myelomac; PFS: Progression-free Survival; MRD: Minimal Residual Disease; TTT: Time to next Treatment.
Introduction
Lenalidomide has become a cornerstone of therapy across the course of multiple myeloma (MM) management. As an immunomodulatory agent, it exerts potent antimyeloma effects through direct tumor suppression, immune activation, and modulation of the bone marrow microenvironment. Historically, its adoption in the frontline setting began with the lenalidomide–dexamethasone (Rd) doublet, which demonstrated meaningful improvements in response rates and progression-free survival (PFS) [1]. With the emergence of triplet combinations such as daratumumab-Rd (D-Rd), lenalidomide remains a core building block in first-line therapy. In the post-transplant setting, randomized trials firmly established lenalidomide maintenance as a therapy capable of significantly extending remission. The pivotal IFM 2005-02 trial demonstrated a doubling of PFS with lenalidomide compared with placebo (41 months versus 23 months) after ASCT [2]. Real-world analyses from the Mayo Clinic and other centers have further shown that extended lenalidomide therapy, particularly beyond three years, is associated with improved outcomes, including deeper responses and achievement of minimal residual disease (MRD) negativity [3, 4].
From 2024 onward, lenalidomide’s influence on the treatment algorithm expanded even further. The updated EMN guidelines classify patients according to lenalidomide exposure and refractoriness when selecting subsequent lines of therapy. In this framework, lenalidomide-sensitive versus lenalidomide- refractory status is now one of the primary determinants of second- and third-line regimen selection [5]. This underscores the drug’s centrality in shaping the entire disease trajectory: patients who receive lenalidomide early, either as Rd frontline therapy or as prolonged maintenance, will almost inevitably transition to lenalidomide-refractory disease at relapse. As a result, lenalidomide’s duration of use has direct implications for the feasibility and sequencing of later therapeutic classes, including proteasome inhibitors and monoclonal antibodies [5].
Despite its broad applicability and clinical value, lenalidomide-treated patients exhibit substantial heterogeneity in both depth and duration of response. While some individuals progress within the first six months of therapy, others remain relapse-free for many years. The biological basis of this divergence remains insufficiently defined and may reflect a combination of baseline cytogenetic risk, clonal evolution under therapeutic pressure, immune system competence, and microenvironment-mediated resistance pathways.
This variability has become increasingly important in contemporary myeloma practice, given that lenalidomide exposure now heavily influences subsequent therapeutic strategy. Early relapse may signify inherently aggressive disease while simultaneously narrowing future treatment options due to lenalidomide refractoriness. In contrast, patients who maintain prolonged sensitivity to lenalidomide often achieve durable disease control and retain greater therapeutic flexibility upon relapse. Clarifying the determinants of early versus prolonged lenalidomide benefit is therefore essential for optimizing treatment sequencing, improving patient stratification, and enhancing long-term disease management.
Patients and Methods
One hundred and eighty-six patients MM patients were studied out of which 158 were treated with Lenalidomide- Dexamethasone and 18 received lenalidomide maintenance after ASCT, from 2005 to 2016 treated to our department with updated survival in 2024. Clinical and laboratory characteristics were collected for all patients following the provision of informed consent. Baseline disease characteristics obtained at MM diagnosis included hemoglobin concentration (Hb), creatinine (Cr), serum calcium, bone marrow plasma cell infiltration, presence of bone disease, platelet count (PLTs), β2-microglobulin, albumin serum levels (alb), ISS stage and LDH levels. A comprehensive review of medical records was performed to document the number of treatment lines, the specific therapeutic regimens administered prior to lenalidomide– dexamethasone initiation, and all subsequent treatments received thereafter. These data were recorded to enable robust evaluation of treatment sequence, response patterns, and outcomes across the cohort. Response to treatment was evaluated according to the International Myeloma Working Group (IMWG) response criteria 2016 [6]. Correlation coefficients (r) and corresponding p-values were calculated to determine the strength and significance of these relationships across all Lenalidomide relapsed/ refractory categories. Time to next Treatment (TTT) was defined as the time from start of treatment until progression or death, with TTT-Len1 denoting the time from lenalidomide initiation to the first relapse requiring a new treatment line, TTT-Len2 representing the time to the second relapse after lenalidomide. Overall survival after Lenalidomide (LenOS) was defined as the time from Lenalidomide initiation until death from any cause; OS curves were plotted by using the Kaplan–Meier method and comparisons were performed with the log rank test. The statistical significance level (p-values) was assessed using the Likelihood ratio method. The statistical significance boundary was set to 5%. Statistical analysis was performed by conventional methods with the SPSS v. 29.0 software.
Results
Patients were separated into 5 groups, including patients (1) with no response within two months (defined as primary resistant MM - PRMM) in the first, (2) progressing under treatment within 6 months from Len initiation in the 2nd (referred as very resistant MM - VRMM) , (3) presenting progression under treatment within 7-12 months (Resistant MM - ResMM), (4) initially sensitive (ISMM), progressing under treatment after more than 12 months and less than 4 years and (5) long-lasting response presenting eventually relapse (RALR) after more than 4 years from Len initiation.
Primary resistant MM (PRMM)
Out of 16 PRMM patients only 6 (37,5%) patients (pts) received next treatment after Rd and managed a further time to next treatment of 9 months. Patients were at 1st line (2 pts), 2nd line (4pts), 3rd line (4 pts), 4th line (3pts), 6th line (2 pts). Next line treatment was in the majority of patients Bortezomib-Dexamethasone (3 pts). Other treatment regimens used after LD were PAD and then Bortezomib- Thalidomide-Dexamethasone (VTD) in one patient and VTD and then Ixazomib-Lenalidomide-Dexamethasone (IRD) in another patient. Median overall survival after Len (LenOS) was 2 months for PRMM patients with 2,4,4,3,1,2 being in 1st, 2nd, 3rd and > 4th line treatment. Only 5 PRMM patients received next treatment line after len and managed a further time to next treatment of 9 months.
Very resistant MM (VRMM)
Twenty-three patients (15%) were classified as VRMM. Among them, three patients achieved responses of sCR, CR, and VGPR, respectively: eight achieved PR, and twelve achieved MR. Of the twenty-three patients, four were receiving first-line treatment, while seven, six, four, and two patients were on second-, third-, fourth- and fifth-line therapy, respectively. Subsequent treatments included Bortezomib- Cyclophosphimide- Dexamethasone (VCD; 8 patients), salvage therapy with conventional chemotherapy followed by Bortezomib-Dexamethasone (Vel-Dex; 1 patient), Vel-Dex alone (4 patients), VTD (6 patients). Median LenOS was 8 months (range: 6–119 months).
Resistant MM (ResMMP)
Twenty-five patients were categorized as ResMM. Most patients (n=9) were receiving second-line therapy; one patient was on first line, and five, six, and four patients were on third-, fourth-, and ≥fifth-line therapy, respectively. Response rates included one sCR, three CR, three VGPR, nine PR, and seven MR. Median time from lenalidomide initiation to next treatment was 8 months (range: 6–12), and median LenOS was 12 months (range: 7–79). LD was the final line of therapy in seven patients, while subsequent treatments in others included VCD (4 patient), Bortezomib Dexamethasone Doxorubicin (PAD ; 4 patients), daratumumab- containing regimens (7 patients) and multiple lines of therapy (3 patients) including selinexor combinations, bispecific B-cell maturation antigen engager, teclistamab and the bispecific T-cell engager, talquetamab.
Initially Sensitive MM (ISMM)
Seventy patients were classified as ISMM. Seven were receiving first-line therapy, 27 were on second-line, 21 on third line, and 7 and 8 patients on fourth- and ≥fifth-line therapy, respectively. Six patients achieved sCR, 14 achieved CR, 18 VGPR, and 28 PR. Median time to next treatment after LD was 26 months (range: 13–48), and median LenOS was 39 months (range: 13–139). Subsequent treatment lines following lenalidomide included regimens containing daratumumab, as well as melflufen, selinexor, belantamab mafodotin, teclistamab and talquetamab. Twenty-nine patients received ≥2 subsequent lines of therapy after lenalidomide–dexamethasone (LD), and 12 received ≥3 lines, with a median time to next treatment after the first and second lenalidomide-based regimens of 33 months (range: 15–80) and 38 months (range: 18–49), respectively.
Relapse after long-lasting response MM (RALR)
Twenty-seven patients were classified as RALR. Three were in first-line therapy, 12 in second-line, three in third- line, and four and five were in fourth- and fifth-line therapy, respectively. Responses included eight sCR, five CR, seven VGPR, and five PR. Median LenOS in this subgroup was 106 months (range: 47–192), and median time to next treatment after LD was 68.5 months (range: 27–110). Six patients required ≥2 subsequent treatment lines and four required ≥3 lines, with median PFS2 and PFS3 of 72 months (range: 60– 124) and 86 months (range: 68–108), respectively.
Lenalidomide Maintenance
Eighteen patients received lenalidomide as maintenance therapy following ASCT. Six patients achieved a deeper response during maintenance: three improved from VGPR to sCR, one from PR to CR, and one from CR to sCR. Six patients who had already achieved sCR maintained this response, while three and one patient maintained VGPR and PR, respectively. No significant difference in LenOS was observed between patients who deepened their response and those who maintained their pre-maintenance response (p=0.383). Median time from lenalidomide maintenance to relapse was 28 months. Three patients developed resistance during maintenance at 4 months (two patients) and 6 months (one patient). Median time from lenalidomide maintenance to next treatment correlated with LenOS (r=0.526, p=0.26).
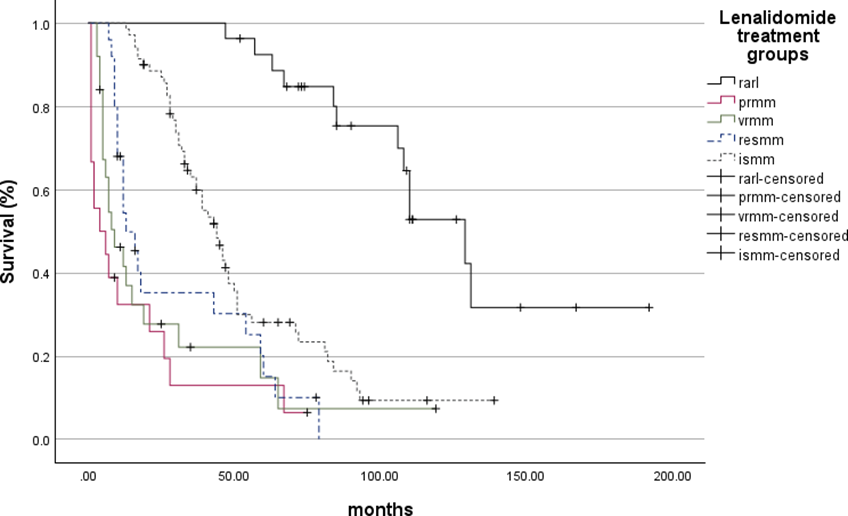
Survival Analysis of Relapsed/Refractory MM patients
Median LenOS differed significantly across subgroups: 2 months (range: 1–3) in PRMM, 8 months (range: 6– 119) in VRMM, 12 months (range: 7–79) in ResMM, 39 months (range: 13–139) in ISMM, and 106 months (range: 47–192) in RALR patients. LenOS was significantly different between all groups (p<0.0001) (Figure: 1).
Correlation Analysis of Multiple Myeloma (MM) Disease Characteristics at Diagnosis with Lenalidomide-Relapsed/Refractory Subgroups
Correlation analysis demonstrated that patients with primary refractory MM (PRMM) showed significant associations with several adverse laboratory parameters at diagnosis, including hypercalcemia (Ca ≥11 g/dL; r = 0.204, p = 0.029), thrombocytopenia (platelets ≤100,000/µL; r = 0.264, p = 0.003), renal impairment (creatinine ≥2 g/dL; r = 0.177, p = 0.050), elevated β2-microglobulin (B2M ≥5.5 mg/L; r = 0.244, p = 0.008), and hypoalbuminemia (albumin ≤3.5 g/dL; r = 0.181, p = 0.046). Patients with very rapid MM relapses (VRMM) demonstrated a significant correlation only with elevated LDH levels (r = 0.193, p = 0.034). No significant correlations were observed between diagnostic clinical or laboratory features and the groups classified as RESMM, ISMM, or RARL.
Discussion
In this analysis of 186 multiple myeloma patients treated with lenalidomide, either in combination with dexamethasone (LD) or as post-ASCT maintenance, we observed marked heterogeneity in treatment outcomes. Stratifying patients into five groups, from primary refractory (PRMM) to long-lasting responders (RALR), highlighted substantial differences in median LenOS, ranging from 2 months in PRMM to 106 months in RALR.
Lenalidomide refractoriness has been the focus of numerous recent investigations, reflecting its central role in the prognostic stratification of patients with multiple myeloma. Dhakal B, et al. [7], using the SEER- Medicare database, demonstrated that patients who become refractory to lenalidomide after one to three prior lines of therapy experience significantly inferior overall survival, underscoring early lenalidomide refractoriness as a major determinant of post-refractory outcomes [7]. Goel U, et al. [8] compared outcomes between patients refractory to standard-dose versus low-dose lenalidomide and reported substantially worse survival among those with primary refractoriness, highlighting the challenging biology of this subgroup [8].
The extremely poor median LenOS of 2 months observed in our PRMM group demonstrates a subgroup with aggressive biology and limited salvage options. Comparable findings were observed in earlier series of primary refractory MM, where primary refractory patients experienced markedly worse overall survival compared with responders [9].
Further supporting the prognostic relevance of refractoriness, Suzuki K, et al. [9] evaluated real-world treatment sequences incorporating daratumumab, lenalidomide, and dexamethasone in transplant-ineligible patients and showed that early lenalidomide refractoriness was consistently associated with shorter subsequent PFS and OS, although some patients were still able to achieve meaningful responses with salvage regimens [9]. In a similar vein, Kastritis E, et al. [10] demonstrated that patients relapsing after first-line lenalidomide had heterogeneous outcomes depending on the timing and nature of subsequent treatments, reinforcing the concept that lenalidomide sensitivity influences both depth and durability of later therapeutic responses [10].
In all these studies, lenalidomide-refractory disease was operationally defined as progression occurring within 60 days of initiating lenalidomide–dexamethasone. However, this binary classification fails to capture the clinically relevant heterogeneity observed in real-world practice. Specifically, these analyses do not distinguish between patients who relapse within 6 months, within 12 months, or at the other extreme, those who experience late relapse after more than five years of therapy. The present study addresses this gap by delineating a more granular spectrum of lenalidomide responsiveness and emphasizing, for the first time, distinct outcome trajectories across early, intermediate, and late relapsers.
The VRMM and ResMM groups in our cohort progression within 6–12 months, demonstrated intermediate survival (median LenOS 8–12 months) and partial responsiveness to subsequent therapies, including bortezomib-based or daratumumab-containing regimens. In contrast, our ISMM and RALR cohorts representing patients with delayed progression and sustained therapeutic benefit demonstrated markedly prolonged median LenOS (39 and 106 months, respectively). The RALR subgroup closely resembles the “exceptional responders” described in prior literature, highlighting that extended lenalidomide exposure can maintain durable disease control and enable multiple subsequent effective treatment lines. Notably, this observation is consistent with our own earlier report characterizing the clinical and biological features of this distinct patient population [11, 12, 13], further supporting the existence of a subgroup with inherently favorable disease biology and prolonged sensitivity to immunomodulatory therapy.
In the maintenance cohort of 18 patients, median time to relapse was 28 months, with isolated cases of early resistance (4–6 months). These findings align with observations from the Myeloma XI trial and other real- world series [14, 15], where a subset of patients progressed early despite maintenance, highlighting the biological heterogeneity of lenalidomide responsiveness even in a post-ASCT setting. Our data underscore that early resistance during maintenance, though uncommon, has important prognostic implications and may influence the choice and timing of subsequent therapies [16]. Resistance to proteasome inhibitors (PIs) in multiple myeloma does not uniformly represent a class-defining refractoriness, as several clinical and translational observations indicate that PI resistance can often be overcome through rational combination strategies rather than through mandatory switching to a different drug class. In practice, the addition of synergistic agents, including monoclonal antibodies, IMiDs, or selective nuclear export inhibitors, has been shown to partially restore PI responsiveness by modulating pathways such as unfolded protein response signaling, oxidative stress, and apoptosis regulation, thereby enhancing PI potency even in clinically challenging settings [17, 18, 19]. A similar pattern is observed in the context of resistance to monoclonal antibodies, where refractoriness may also be partially overcome through the incorporation of mechanistically synergistic agents. Early- phase reports and meeting abstracts describe activity of selinexor combinations (including selinexor + daratumumab ± dexamethasone) in daratumumab- refractory cohorts, providing preliminary clinical evidence that selinexor may re-sensitize or augment anti- CD38 activity in selected patients [17, 20, 21, 22]. Τhese effects are plausibly mediated via restoration of pro- apoptotic signaling and modulation of immune-related pathways that complement antibody- mediated cytotoxicity [18, 20].
By contrast, lenalidomide refractoriness has proven more refractory to simple “add-on” strategies aimed at re- sensitization. Randomized and pooled analyses established that pomalidomide (a next-generation IMiD) combined with dexamethasone yields consistent antimyeloma activity in patients who have progressed on lenalidomide and proteasome inhibitors, improving progression-free and overall survival compared with older regimens and becoming the standard IMiD choice after lenalidomide failure [19, 22]. Translational data suggest that pomalidomide retains activity against certain lenalidomide-resistant clones through distinct modulatory effects on cereblon-dependent substrates and on the immune microenvironment, which likely explains the superior clinical efficacy of a class-switch approach rather than attempting to re-sensitize to lenalidomide itself [22, 23].
In addition, PRMM patients demonstrated clear associations with several high‐risk clinical and laboratory features at diagnosis, indicating the aggressive biological behavior characteristic of primary refractory disease. Conversely, none of the baseline diagnostic characteristics evaluated in our cohort were able to differentiate the remaining lenalidomide-resistant subgroups (RESMM, ISMM, RARL), suggesting that conventional clinical parameters may lack sufficient discriminatory power to identify patients at risk of developing later resistance. This highlights a critical unmet need for the incorporation of novel prognostic or predictive biomarkers such as genomic, cytogenetic, or microenvironmental indicators that can better capture the underlying biology of therapeutic resistance.
Limitations of our study include its retrospective design, heterogeneous prior therapy, and lack of cytogenetic and molecular profiling. However, the real-world nature of our cohort provides valuable context for understanding clinical variability and complements larger databases and trial-based analyses. Importantly, our stratification approach provides a practical framework to predict patient outcomes and guide therapeutic sequencing in routine practice, especially in light of evolving guidelines that classify subsequent therapy based on lenalidomide exposure.
Conclusion
Our findings confirm that the timing of relapse represents a robust predictor of survival in multiple myeloma. Disease progression within 12 months of lenalidomide– dexamethasone initiation, irrespective of transplant status or depth of response, is associated with markedly reduced overall survival. Despite the expanding availability of novel therapeutic agents, this subgroup continues to experience poor clinical outcomes. In particular, patients with primary refractory (PRMM) and very resistant (VRMM) disease, although representing a minority of the cohort, exhibit extremely limited salvage treatment options. The proposed relapse-based categorization might offer a more refined understanding of underlying disease biology and informs strategic sequencing of therapy in contemporary multiple myeloma management. Future prospective investigations integrating genomic, immunologic, and clinical variables are warranted to enhance risk stratification and optimize individualized treatment sequencing in the era of modern therapeutic modalities.
Acknowledgement
The authors acknowledge Abbio Therapeutics for supporting the publication of this article.
References
-
Benboubker L, Dimopoulos MA, Dispenzieri MD, John C, Andrew MD, et al. (2014) Lenalidomide and dexamethasone in transplant-ineligible patients with newly diagnosed multiple myeloma (FIRST trial). N Engl J Med 371: 906-917.
-
Attal M, Lauwers V, Marit G, Caillot D, Moreau P, et al. (2012) Lenalidomide maintenance after stem-cell transplantation for multiple myeloma. N Engl J Med 366: 1782-1791.
-
Abeykoon JP (2021) Real-world outcomes of lenalidomide maintenance in multiple myeloma. Leuk Lymphoma 62: 2925-2932.
-
Holstein SA (2020) Updated analysis of lenalidomide maintenance therapy in multiple myeloma. Blood Adv 4: 2163-2171.
-
Dimopoulos MA, Terpos E, Boccadoro M, Moreau P, Mateos MV, et al. (2025) EHA–EMN evidence-based guidelines for diagnosis, treatment, and follow-up of patients with multiple myeloma. Nat Rev Clin Oncol 22: 680-700.
-
Kumar S, Paiva B, Anderson KC, Durie B, Landgren O, et al. (2016) International Myeloma Working Group consensus criteria for response and minimal residual disease assessment in multiple myeloma. The Lancet Oncology 17: e328-e346.
-
Dhakal B, He J, Schecter JM, Deraedt W, Slaughter A, et al. (2025) Real-world treatment patterns and outcomes in patients with lenalidomide-refractory multiple myeloma with 1–3 prior lines. Clin Lymphoma Myeloma Leuk 25: e394-e403.
-
Goel U, Charalampous C, Kapoor P, Binder M, Buadi FK, et al. (2024) Outcomes of patients with multiple myeloma refractory to standard-dose versus low-dose lenalidomide. Blood Cancer J 14: 55.
-
Suzuki K, Fujimori Y, Sakai C, Tsuchiya H, Koroki Y (2025) Real-world treatment outcomes of different sequencing options with daratumumab, lenalidomide, and dexamethasone in transplant-ineligible multiple myeloma in Japan. Cancers 17: 1389.
-
Majithia N (2015) Outcomes of primary refractory multiple myeloma. PMC.
-
Kastritis E, Stathopoulos I, Theodorakakou F, Migkou M, Roussou M, et al. (2024) Characteristics and outcomes of patients with relapsed/refractory multiple myeloma after exposure to lenalidomide in first-line therapy: a single- center database review in Greece. Clin Lymphoma Myeloma Leuk 24: 468-477.
-
Kyrtsonis MC, Gkioka AI, Nikolaou E, Bartzis V, Papaioannou P, et al. (2017) Long-lasting Responses to Immunomodulatory Drugs (IMIDs) in Combination with Dexamethasone in Multiple Myeloma; Identification of Exceptional Responders at any Treatment Line. Haematology International Journal 1(2): 1-6.
-
Ho M, Zanwar S, Kapoor P, Gertz M, Lacy M, et al. (2021) Impact of duration of lenalidomide maintenance on outcomes of salvage regimens in multiple myeloma. PMC.
-
Alonso R, Cedena MT, Wong S, Shah N, Tamayo R, et al. (2020) Prolonged lenalidomide maintenance and clinical outcomes in multiple myeloma. Blood Adv 4: 2163-2171.
-
Jackson GH, Joseph NS, Kaufman JL (2019) Long-term follow-up results of lenalidomide, bortezomib, and dexamethasone induction therapy and risk-adapted maintenance approach in newly diagnosed multiple myeloma. Lancet Oncol 20: 57-73.
-
Biran N (2025) Phase IIb study of selinexor plus daratumumab in daratumumab-refractory multiple myeloma. Haematologica. PubMed.
-
Huang Q, Zhao R, Xu L, Hao X, Tao S (2024) Mechanistic and clinical review of selinexor in multiple myeloma and its combination strategies. Hematology Review Series.
-
San Miguel JF, Weisel K, Moreau P, Lacy M, Song K, et al. (2013) Pomalidomide plus low-dose dexamethasone versus high-dose dexamethasone in relapsed/refractory multiple myeloma (MM-003 trial). Lancet Oncol 14: 1055-1066.
-
Mateos MV (2024) Post-hoc analyses providing mechanistic rationale for selinexor in overcoming proteasome inhibitor resistance in multiple myeloma. Scientia Salut Technical Reports.
-
Gasparetto C (2024) Phase 1b evaluation of selinexor in combination with daratumumab ± dexamethasone in relapsed/refractory multiple myeloma. ASCO Meeting Abstracts.
-
Dimopoulos MA (2014) Pooled analyses of pomalidomide efficacy in lenalidomide-resistant relapsed/refractory multiple myeloma. Blood.
-
Fujita H (2022) Differential cereblon modulation explains preserved activity of pomalidomide in lenalidomide- resistant myeloma cells. Blood Advances 6: 1452-1463.
-
Manier S (2021) Advances in understanding multiple myeloma biology: emerging biomarkers and therapeutic targets. Journal of Hematology & Oncology 14: 143-156.
- How to Identify and Overcome Barriers in Developing Blood Systems?
- Why Was Transfusion Medicine Not Recognized as a Clinical Discipline?
- Is Transfusion Always Necessary?
- The Logistics of Production and Use of Blood and Blood Components
- The Challenge for Component Therapies
- Effect of Monoclonal Gammopathy on Risk of Kidney Failure among Patients with Chronic Kidney Disease