Prevalence of Depression and Balance Affection in Postmenopausal Women-A Cross-Sectional Study
Background: Menopause is an essential and normal developmental process in a women’s life that may result in a wide variety of symptoms hence creating different problems. Psychological disorders particularly depression and balance affection are the most frequently observed public health problems of postmenopausal women requiring attention and even physiotherapy intervention. Hence, this study aimed to evaluate the prevalence of depression and balance affection in post-menopausal women. Materials and Methods: This study was conducted on 210 post-menopausal women aged between 45-60 years fulfilling the inclusion criteria. The subjects were selected by convenient sampling with prior consent and general assessment was taken. Gujarati version of Patient Health Questionnaire-9 (PHQ-9) and Berg Balance Scale (BBS) were used as outcome measures and data analysis was conducted for descriptive and analytical statistics. Results and Discussion: The mean value of age was 53.22 + 4.5 years. The mean score of depression for the subjects was 8.58 ± 3.59, which indicated mild depression. The results showed that 17.14% of women had minimal depression, 41.43% had mild depression, 32.86 had moderate depression and 8.57% had moderately severe depression. For balance affection mean value was 48.64±3.59, which indicated low fall risk. In balance affection, results showed that 97.63% had low fall risk, 2.38% had medium fall risk and 0% had high fall risk. Conclusion: A significant percentage of women in their menopause experienced depression and balance affection. This study showed that the majority of women included in the study had experienced mild depression and low fall risk for balance affection.
Introduction
A woman’s life is influenced by the two most important physiological transitions–former menarche and the latter menopause [1]. The term “Menopause” can be described as a permanent cessation of menstruation marking the end of reproductive life influenced by the loss of ovarian follicular activity [2]. The North American and European female populations normally experience menopause around the average age of 50 years, the range being between 40 and 58 years of age [3]. A period of great hormonal adjustments sets in which is followed by menopause, including a time frame of emotional and physical challenges in a woman’s life [4].
Females in their menopausal phase experience a wide variety of symptoms [5]. Amongst these, psychological symptoms remain at the forefront during these phases including depression, loss of memory, irritability, poor concentration, tiredness, and loss of confidence, which have an influence on menopausal women in modern societies [5]. Moreover research shows that depression becomes more prominent in females at the age of menopause, which can be attributed to hormonal fluctuations [6]. Depression can be described as an abnormal emotional state characterized by exaggerated feelings of sadness, melancholy, worthlessness, emptiness, and hopelessness that are resulting from negative cognition towards self.1 The National Co-morbidity Study found rates of recurrent depression to be highest among women between the ages of 45 and 54 years when compared with those of older women [7]. These can be described to be influenced by a decrease in gonadal hormone levels, which subsequently leads to fatigue, loss of sleep, and night-time hot flashes [6]. It is known that depressed postmenopausal women experience a low concentration of estradiol and serotonin and on the other hand FSH concentrations are high hence leading to changes in the functions of the nervous system, and eventually depression during this period [8]. Moreover several kinds of research are undertaken demonstrating balance affection in postmenopausal women. The term “balance” can be defined as the capability to move with the help of body weight without losing stability [9]. It could be defined as a dislocation of the body to an inferior level to the initial position unknowingly along with incapacity for correction in due time and a multi-factorial etiology [10]. This can be again attributed to hormonal influences. As menopause approaches, there is a dramatic reduction in estrogen production and acceleration of bone loss, which may lead to fractures if a fall is sustained [11]. Postural changes in postmenopausal women include forward head, rounded shoulders, increased kyphosis, decreased lumbar lordosis and flexed hips as well as knees [12]. These changes may result from loss of elasticity in connective tissues, diminished ability to counteract gravitational forces, and decline of muscle strength as well as, endurance [13]. All of these postural changes affect daily living activities, balance, and gait, hence; increase the risk of falling [12]. Postural balance control deteriorates with increasing age, reducing functional capacity in postmenopausal women [13]. The falls are more pronounced from age 45 in women and maximum in the 55-59 years of age [11]. Postural stability and balance decrease with age [14]. The estrogen loss that occurs with menopause has a significant impact on various body systems such as; vestibular, visual, musculoskeletal, and nervous systems [12].
The incidence of depression and risk of fall is twice in women compared to men. There are very few researches that show that depression and balance affection can be seen in post-menopausal women. Hence this study aims to find out the prevalence of depression and balance affection in post- menopausal women.
Methodology
A cross-sectional study was conducted on 210 postmenopausal women residing in Nadiad and Anand city of Gujarat by a convenient sampling method. Females in the age group between 45-60 years with normal hip, knee, and ankle joint ROM were included in the study. Women who were not willing to participate, undergone hysterectomy, on hormonal therapy, history of smoking and alcohol drinking, or had any major medical illness in the last 6 months were excluded from the study. Based on inclusion and exclusion criteria, written informed consent was obtained from all subjects before enrolment in the study. The institutional ethical clearance has been obtained for this study. The subjects were assessed for depression by Gujarati version of PHQ – 9 Questionnaire and balance by BBS.
Results
All statistical analysis was performed using the SPSS version 19 for windows. Basic parameters like age, height, weight, and Body Mass Index (BMI) were taken from 210 post-menopausal women. Descriptive statistics, including mean, Standard Deviation (SD), and Standard Error (SE) were analysed (Tables 1-4 & Graphs 1 & 2).
| Mean | Standard Deviation (SD) | Standard Error (SE) | |
|---|---|---|---|
| Age (Year) | 53.22 | 4.5 | 0.31 |
| Height (cm) | 154.83 | 4.8 | 0.33 |
| Weight (kg) | 70.08 | 10.27 | 0.71 |
| BMI (kg/m2) | 29.18 | 3.82 | 0.26 |
| PHQ-9 | 8.58 | 3.97 | 0.27 |
| BBS | 48.64 | 3.59 | 0.25 |
Table 1: Descriptive analysis of the obtained data.
The prevalence of depression by using PHQ-9 scale in 45 – 60 years of the age group for postmenopausal females mean was 8.58 + 3.97. The prevalence of balance affection by using BBS in 45 – 60 years of the age group for post-menopausal females mean was 48.64 + 3.59.
| Mean | Grading | |
|---|---|---|
| PHQ-9 | 8.58 | Mild Depression |
| BBS | 48.6 | Low Fall Risk |
Table 2: Mean scores of Depression and Balance affection.
While observing the mean data for the entire group and correlating it with grading, the given study population experiences Mild depression and Low fall risk.
| Severity | Percentage (%) | |
|---|---|---|
| 1 | Minimal Depression | 17.14 |
| 2 | Mild Depression | 41.43 |
| 3 | Moderate Depression | 32.86 |
| 4 | Moderately Severe Depression | 8.57 |
| 5 | Severe Depression | 0 |
Table 3: Severity and Percentage of PHQ-9 scores.
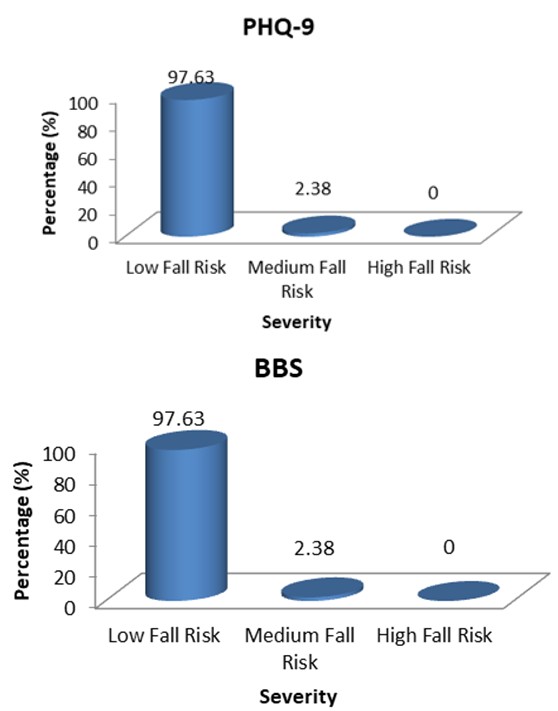
Graph 1: Graphical representation of PHQ-9 scores.
| Severity | Percentage (%) | |
|---|---|---|
| 1 | Low Fall Risk | 97.63 |
| 2 | Medium Fall Risk | 2.38 |
| 3 | High Fall Risk | 0 |
Table 4: Severity and percentage of BBS scores.
Graph 2: Graphical representations of BBS scores.
Discussion
The two most important public health problems affecting postmenopausal women are depression and balance that require attention. The present study showed that the majority of women had experienced mild depression according to the PHQ-9 scale and the severity of balance affection is very low according to the BBS scale.
Afshari, et al. [6] have suggested that the mean depression scores of the subjects, was 9.7 ± 4.19. Approximately 59.8% of the study subjects had depression (mild, moderate, and severe). This was explained by the phenomenon that low concentrations of estradiol and serotonin and high concentrations of follicle-stimulating hormone may be responsible for changes in the functions of the nervous system, and hence leading to depression.
Another study conducted by Polisseni, et al. [15] in Brazil found that the prevalence of depression during menopause was 40%. Dolatian, et al. [16] conducted a study evaluating the prevalence of depression and its associated factors at various phases of menopause in women living in Kermanshah and found that 32.2% of residents turned out to be depressed. Further evaluating based on stages of menopause, the highest prevalence of depression was found to be 39.3% among postmenopausal women, and the lowest of 21.6% in women in their premenopausal phase [16].
These differences could be attributed to factors like culture, religion, race, and attitude.
Moreover, there is evidence suggesting growing recognition of the relationship between osteoporosis, fragility, falls, and fractures. The result of this study is also in correlation with a study done by Sumit Kalra et al. where the effect of menopause on balance score was compared in females with menopause to those with regular menstrual cycle by using the Star Excursion Balance Test (SEBT) and Timed Up and Go test (TUG) where they concluded that balance score was significantly affected in the menopausal group [17]. In a study conducted by Cangussu, et al. [14] 57.8% of women experienced falls in the last 2 years and 16.2% of these falls were observed following fractures. In fact, 90% of the steady incline in hip fractures related to hip and the sixth cause of death amongst these sufferers in the age group of more than 65 years was attributed to falls [17].
Crilly, et al. [18] suggested that hormonal changes have effects on postural stability hence leading to increases in incidences of falls during menopause. Nitz, et al. [19] carried out a study to investigate the changes in the mediolateral balance of women in 40 to 80 years of age group and concluded that the ability for mediolateral balance shows a significant reduction in the 40 to 60 years of the age group which corresponds to the menopausal age. Further this can be explained by the phenomenon that there is a withdrawal of estrogen after menopause which is responsible for information processing in the brain, an essential requirement for postural stability that is mediated through identification of sensory input and initiation of an appropriate physical response and hence disturbances in these phenomena leads to the adverse consequences of instability in this postmenopausal phase.
Conclusion
This study found mild depressive symptoms in the postmenopausal period in the majority of women. The balance affection was with a very low severity in postmenopausal women.
References
-
Lee young W (2003) RN. Depression in Posit Menopausal Women. J Korean Acad Nurs 33(4):471–477.
-
Dutta D (2013) DC Dutta’s Textbook of Gynecology. In: Konar H (Ed.), 6th (Edn.), Panama: JP Brothers Medical Publisher New Dehli, London, Philadelphia, USA, pp: 57.
-
Fu S, Low Choy N, Nitz J (2009) Controlling balance decline across the menopause using a balance-strategy training program: A randomized, controlled trial. Climacteric 12(2): 165-176.
-
Frey BN, Lord C, Soares CN, Frey BN, Lord C, et al. (2008) Depression during menopausal transition: a review of treatment strategies and pathophysiological correlates. Menopause Int 14(3): 123-128.
-
Bruce D, Rymer J (2009) Best Practice & Research Clinical Obstetrics and Gynaecology Symptoms of the menopause. Best Pract Res Clin Obstet Gynaecol 23(1): 25-32.
-
Afshari P, Manochehri S, Tadayon M, Kianfar M, Haghighizade M (2015) Prevalence of Depression in Postmenopausal Women. Jundishapur J Chronic Dis Care 4(3): 5.
-
Bosworth HB, Bastian LA, Kuchibhatla MN, Steffens DC, McBride CM (2001) Depressive Symptoms, Menopausal Status, and Climacteric Symptoms in Women at Midlife. Psychosom Med 63(4): 603-608.
-
Unsal A, Tozun M, Ayranci U (2011) Prevalence of depression among postmenopausal women and related characteristics. Climacteric 14(2): 244-251.
-
Lu SY, Tseng HF, Lin LL, Luh WM, Shu BC (2009) Factors Related to Depression During Menopause: A Study in Southern Taiwan. J Nurs Res 17(2): 128-135.
-
Pereira VV, Maia RA, Maria S, Azevedo CD (2013) The functional assessment Berg Balance Scale is better capable of estimating fall risk in the elderly than the posturographic Balance Stability System. Arq Neuropsiquiatr 71(1): 5-10.
-
Ekblad S, Bergendahl A, Enler P, Ledin T, Mollen C, et al. (2000) Disturbances in postural balance are common in postmenopausal women with vasomotor symptoms. Climacteric 3(3): 192-198.
-
El-mekawy HS, Kamel DM, Moursi MS, El- AM (2007) Effect of Balance Training on Postural Stability in Obese Postmenopausal Women. 12(2): 159-167.
-
Nahas-neto J, Cangussu LM, Buttros DDA (2012) Effect of hormone therapy on postural balance in postmenopausal women Menopause 19(7): 768-775.
-
Cangussu L, Nahas Neto J, Petri Nahas E, Rodrigues Barral A, Buttros D, et al. (2012) Evaluation of postural balance in postmenopausal women and its relationship with bone mineral density - A cross-sectional study. BMC Musculoskelet Disord 13(2).
-
Polisseni AF, de Araujo DA, Polisseni F, Mourao Junior CA, Polisseni J, et al. (2009) Depression and anxiety in menopausal women: associated factors. Rev Bras Ginecol Obstet 31(1): 28-34.
-
Dolatian M, Bakhteh A, Valaie N, Afshar F (2006) Prevalence of Menopausal Related Depression and Its Relative Factors. J of Kermansha Uni of Med Sci 10(10): 76.
-
Sumit K, Nidhi K (2015) Effect of Menopause on Balance Score. Physiotherapy and Occupational Therapy Journal 8(4): 133-137.
-
Crilly RG, Richardson LD, Roth JH, Vandervoort AA, Hayes KC, et al. (1987) Postural stability and colles’ fracture. Age Ageing 16(3): 133-138
-
Nitz JC, Choy NL, Isles RC (2003) Medial-lateral postural stability in community-dwelling women over 40 years of age. ClinRehabil 17(7): 765-767.
- Potential Medicinal Herbs and Secondary Metabolites in Combating Corona Virus
- Monkeypox and its Clinical Implications in Pregnancy
- Pharmacognostical Analysis of the Leaves of Important Nervine Medicinal Plant: Strychnos Nux-Vomica L
- Assessment of Antibacterial Activity of Various Solvent Extracts of Dictyota Dichotoma Against Multidrug Resistant Bacterial Strain
- An Insights of Bioactive Elements on Malignancy: Mechanistic Avenues
- Advances and Future Directions in Pharmacognosy and Chinese Medicine