Spontaneous Celiac Artery Dissection: A Case Report
Spontaneous visceral artery dissection is an exceptional condition. In the literature, about a hundred of cases are reported. It most often involves the superior mesenteric artery, and secondarily the celiac trunk. The presentation is non-specific and the diagnosis is usually made on imaging or at autopsy. Pre-existing vascular diseases, hypertension and pregnancy are the most involved risk factors. We report the case of a 58-year-old patient who presented for a spontaneous dissection of the celiac artery treated medically.
Case Report
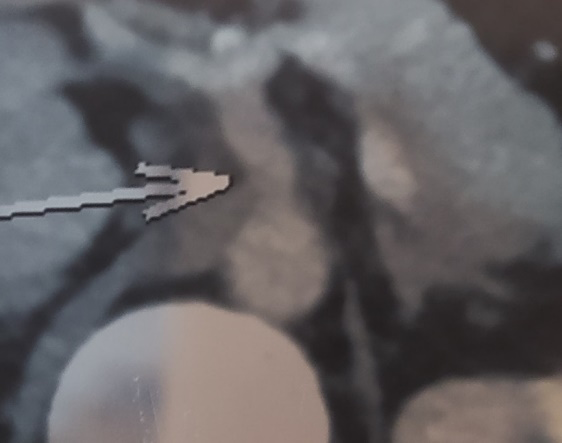
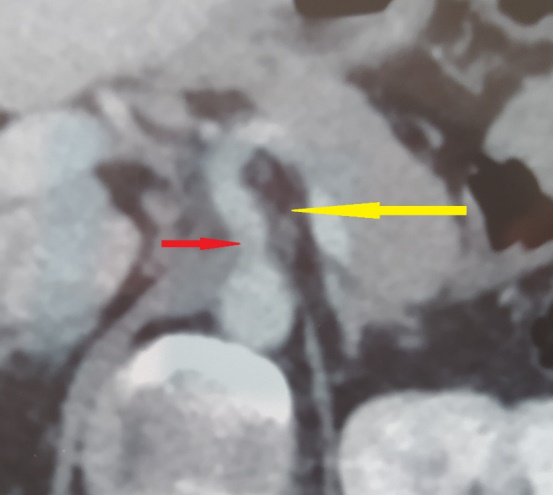
A 58-year-old patient with a high blood pressure history, presented to our emergency room with epigastralgia of sudden onset evolving from hours without vomiting or other associated signs. On examination, the patient was hemodynamically stable and had tenderness in the epigastric region. There were no other abnormalities. The biology tests revealed white blood cells count of 13800elm/ ml and a CRP level at 22mg/l. Blood lipase and liver tests were normal. Due to this clinical presentation mimicking an acute pancreatitis, we decided to proceed to an abdominal CT-scan. It revealed a false channel of the celiac trunk without associated aneurysmal dilation (Figure 1) and an infiltration of the peri- vascular fatty tissue (Figure 2). The patient was admitted and a treatment with calcium channel blockers, analgesics and platelet aggregation inhibitors was prescribed. The evolution was favorable with total disappearance of pain after 72 hours from the start of treatment. He was discharged on the fifth day of treatment and a CT imaging, for control, is planned in one month.
Discussion
Spontaneous visceral artery dissection is a rare condition that was first described by Baurersfeldin 1947 [1]. It can affect the left gastric, hepatic, splenic, or celiac artery but the superior mesenteric artery is the one that is more affected [2]. The spontaneous celiac artery dissection was first reported in 1959[3]. It seems to be more frequent with-in men with an average age of 55 years [4]. The most known risk factors are those leading to weakening of arterial wall like pregnancy, hypertension, fibromuscular dysplasia, and aortic aneurysm [5] or those causing mechanical stretching and microtrauma like lifting or sneezing [6]. Visceral artery dissection has no specific clinical presentation. It is mostly asymptomatic if there is no ischemia [7]. However patients commonly present for severe epigastric or hypochondrial pain [3]. The diagnosis is usually made by imaging. In fact CT-angiography is considered to be the imaging technique of choice because it can display luminal borders and extra luminal disease [3, 7, 8]. Medical management consists in limiting the progression of the dissecting hematoma, controlling the blood pressure and preventing the thrombo embolic complication [7]. Outcomes are usually simple. However, it can progress to splenic infarction, intra peritoneal hemorrhage, and intestinal ischemia [9]. After the acute episode, in addition to a strict blood pressure control, and in order to prevent the thrombo embolic complications, the use of anticoagulant or platelet aggregation inhibitor is recommended during 3-6 months with a target INR of 2.0-3.0 [7, 10]. Surgery is usually indicated when medical therapy fails [3]. It consists in the resection of the dissected segment with anastomosis or by creating a bypass [7]. While endovascular treatment is being more and more reported there is no published data supporting its superiority to surgery [3]. Given the risk of aneurysmal transformation, a clinical and radiological monitoring is necessary [11]. A doppler ultrasonography should be performed at the first, the third, the sixth month and then annually. In case of modification or anomaly a CT- angiography must be performed [11, 12].
Conclusion
Spontaneous dissection of the celiac artery is a rare condition. Its diagnosis is difficult in the absence of particular clinical orientation signs. The diagnosis is usually confirmed by angiography or CT angiography. Evolution is most often favorable under medical treatment. Nevertheless, radiological monitoring is necessary given the risk of aneurysmal transformation.
References
-
Zhang WW, Killeen JD, Chiriano J, Bianchi C, Teruya TH, et al. (2009) Traitement des dissections spontanées: symptomatiques isolées des artères digestives l’intervention en urgence est-elle nécessaire. Annales de Chirurgie Vasculaire 23(1) : 97-101.
-
Glehen O, Feugier P, Aleksic Y, Delannoy P, Chevalier JM (2001) Spontaneous dissection of the celiac artery. Annals of vascular surgery 15(6): 687-692.
-
Dent MO, Shabaneh B, Dougherty KG, Strickman NE (2012) Spontaneous celiac artery dissection case report and literature review. Texas Heart Institute journal 39(5): 703-706.
-
D’Ambrosio N, Friedman B, Siegel D, Katz D, Newatia A, et al. (2007) Spontaneous isolated dissection of the celiacartery: CT findings in adults. AJR Am J Roentgenol 188(6): W506-511.
-
Zeebregts CJ, Schepens MA, Hameeteman TM, Morshuis WJ, de la Rivière AB (1997) Acute aortic dissection complicating pregnancy. The Annals of thoracic surgery 64(5): 1345-1348.
-
Woolard JD, Ammar AD (2007) Spontaneous dissection of the celiac artery. Journal of Vascular Surgery 45(6): 1256-1258.
-
Sandeep V, Dighe M (2010) Spontaneous celiac artery dissection and its management. Journal of Radiology Case Reports 4(4): 30-33.
-
Subhas G, Gupta A, Nawalany M, Oppat WF (2009) Spontaneous isolated superior mesenteric artery dissection: a case report and literature review with management algorithm. Annals of Vascular Surgery 23(6): 788-798.
-
Nordanstig J, Gerdes H, Kocys E (2009) Spontaneous isolated dissection of the celiac trunk with rupture of the proximal splenicartery:a case report. Eur J Vasc Endovasc Surg 37(2): 194-197.
-
Fenoglio L, Allione A, Scalabrino E, Alberto G, Benedetti V, et al. (2004) CASE REPORT: Spontaneous Dissection of the Celiac Artery: A Pitfall in the Diagnosis of Acute Abdominal Pain. Presentation of Two Cases. Digestive diseases and sciences 49(7-8): 1223-1227.
-
Palma SP, Lacroix A, Akoum N, Guillemard O, Brousse B (2013) Une cause rare de douleur lombaire: la dissection spontanée isolée dutronc coeliaque. Annales françaises de médecine d’urgence 3(6): 384-386.
-
Subhas G, Gupta A, Nawalany M, Oppat WF (2009) Spontaneous isolated superior mesenteric artery dissection: a case report and literature review with management algorithm. Annals of Vascular Surgery 23(6): 788-798.
- Pattern of Breast Lesions in Ovu Inland, Delta State, South Southern Nigeria
- Morphometric Analysis of the Human Femur: Exploring Platymetric and Robusticity Indices Among the Nigerian Population
- Anatomical Variation of Arteria Lusoria: Clinical Implications for Dysphagia Lusoria and Surgical Risk
- Morphometric Study of the Vertebral Body and Pedicle of Typical Cervical Vertebrae Using Radiological Image
- Epigenetic Mechanisms Driving Human Evolutionary Changes
- Neuroprotective Effects of Ginkgo Biloba Extract on Bilateral Common Carotid Artery Ischaemic Stroke Induced in Wistar Rat