Neuroprotective Effects of Ginkgo Biloba Extract on Bilateral Common Carotid Artery Ischaemic Stroke Induced in Wistar Rat
Stroke is one of the most prevalent vascular diseases in the world and has persistently ranked as at least the third leading cause of death globally over the past few decades (WHO). Ginkgo biloba extract (GBE) contains flavonoids and ginkgolides making it a promising anti-oxidative natural product. The aim was to evaluate neuroprotective effects of GBE on hippocampus and cerebrum of Wistar rat with acute ischaemia induced by the bilateral common carotid artery occlusion (BCCAO).Thirty adult male Wistar rats were randomly assigned to 5 study groups (n=6) and acclimatized in clean cages for a week. Group A, received Normal saline, Group B received GBE only, Group C had BCCAO only, Group D received GBE presurgery, and Group E received GBE postsurgery. The safe oral GBE daily dose of 100 mg/kg/day was administered for 14 days. 2 rats shared 1 capsule per day at average weight of 200 grams. Giloba, the soft gel capsule used, was manufactured by Mega Life Sciences Nigeria Ltd.: NAFDAC Reg. No. A7-0404L. After adequate anaesthesia at 80-100mg/kg of intraperitoneal Ketamine, BCCAO was performed with 3/o silk suture ligation. Reperfusion was allowed after 30 minutes. Analgesia and antibiotic prophylaxis were with intramuscular paracetamol injection and topical penicillin cream. Neurobehavioral changes in spatial exploration was assessed using Y-Maze toolkit. On day 21, from onset of acclimatization, the rats were sacrificed by gentle cervical dislocation under mild anaesthesia and the whole brain harvested for histomorphological studies.GBE offered neuroprotection as evidenced by remarkably less pyknotic cells and perineuronal vacuolations in the brain tissue with prophylactic effect being more pronounced than therapeutic action. It also boosted spatial working memory in the rats.
Abbreviations
WHO: World Health Organization; GBE: Ginkgo Biloba Extract; BCCAO: Bilateral Common Carotid Artery Occlusion; GBD: Global Burden of Disease; DALYs: Disability-adjusted Life-years; WHF: World Heart Federation; AHA: American Heart Association; ICA: Internal Carotid Artery; TIA: Transient Iscahemic Attack; ACUREC: Animal Care and Use Research Ethics Committee.
Introduction
Globally, more than 80 million people have survived a stroke. About 70% of incident strokes are ischaemic (9.5 million) and the rest are intracerebral and or subarachnoid haemorrhage, the proportion of ischaemic strokes in the US is estimated to be higher, at about 85%- 87%. According to the most recent Global Burden of Disease (GBD) estimates, there were around 12.2 million incident cases of stroke,
143 million disability-adjusted life-years (DALYs) lost, and 6.6 million deaths globally in 2019, making stroke transit from the third to the second leading cause of death, hence a rising stroke burden across the globe is remarkable. Stroke is one of the most prevalent vascular diseases in the world and persistently ranks as the 5th leading cause of death in the United States. The World Heart Federation (WHF) stated that, every year, 15 million people worldwide suffer a stroke, nearly six million die and another five million are left permanently disabled and this disability include confusion, paralysis, loss of vision and/or speech. Despite the gravity of stroke and the advances of technologies nowadays, clinical therapy of the deliberating disorder is still not in the satisfaction level; therefore, the prophylactic protection against stroke with neuroprotective agent has gained much attention [1]. The 2019 American heart association (AHA) report on heart disease and stroke statistics estimates that twenty million Americans greater than 20 years of age have had a stroke. Approximately 795,000 people have a stroke each year. Prevalence increases with age, with nearly 75% of cases affecting people over the age of 65. Strokes prevalence is greater among African Americans and Hispanic people than Caucasians.
The prevalence of stroke is approximately the same in both females and males, with a slight female predominance as prevalence decreased in males over the past 15 years [2]. Increasing interest in improving treatment options for ischaemic stroke requires the continuous exploration of new treatments options that may lead to a viable clinical application [3]. However, cardiovascular disease and stroke remain the leading causes of long-term disability globally and is noted to have total direct and indirect cost of about 315 billion USD in 2010 with now more-than-double the annual cost estimate in Nigeria, West Africa. In Nigeria, ‘stroke epidemics’, a neurologicalemergency ofconcern was reported as constituting a major clinico-epidemiologic burden to conscientious neurological emergency physicians, neurologists and neurosurgeons at both public and private health institutions with streaks the young and the elderly in both genders.
There are multiple risk factors for strokes which can be divided into modifiable and non-modifiable categories with many of the causes of hemorrhagic and ischemic strokes overlapping. The non-modifiable risk factors of each of the variants include age, sex, race, and genetics. The risk increases with age with the risk higher in males at a younger age, but the risk of death is higher on the overall in women; and the risk significantly greater in African Americans, and slightly higher in Hispanics and Native Americans as well compared to the Whites. Modifiable risk factors include hypertension, smoking, obesity, alcohol consumption, hyperlipidemia, physical and psychological stress, diabetes, however the cardiac causes such as cardiomyopathy, heart failure, and atrial fibrillation, are risk factors for ischemic (cardio-embolic) stroke but not hemorrhagic stroke.
Acute ischemic stroke (AIS) is the fourth leading cause of death and the leading cause of adult disability in the USA. However, the most recent reports by World Health Organization (WHO) in the past few decades ranks stroke to be the third leading cause of death globally hence, making it a neurological emergency of concern to conscientious neurological emergency physicians, neurologists and neurosurgeons both locally and globally [4]. AIS most commonly occurs when a blood vessel is obstructed leading to irreversible brain injury and subsequent focal neurologic deficits. The pathophysiology of AIS is both simple and complex. Simple in that the initiating event is the occlusion of an intracranial or neck blood vessel that in most cases impairs blood flow to a portion of the brain, leading to infarction of brain tissue in the part of the brain supplied by that blood vessel. The vessel occlusion can occur in relationship to a local vessel occlusion typically in patients with intracranial atherosclerosis, artery to artery embolization typically from an internal carotid artery (ICA) plaque, or secondary to embolization of a clot from the heart to a brain vessel as exemplified by atrial fibrillation [5].
Transient iscahemic attack (TIA) is a sudden, focal neurologic deficit that lasts for less than 24 hours. It is presumed to be of vascular origin, and is confined to an area of the brain or eye perfused by a specific artery. Typical symptoms include hemiparesis, hemiparesthesia, dysarthria, dysphasia, diplopia, circumoral numbness, imbalance, and monocular blindness. TIAs are often referred to as mini- strokes, warning strokes, or transient strokes because they resolve quickly. Factors associated with an increased risk of stroke after a TIA include advanced age, diabetes mellitus, symptoms for more than 10 minutes, weakness, and impaired speech [6]. The World Health Organization (WHO) reports that due to stroke’s high mortality, and high disability, it has continued to pose the greatest threat to human health globally especially in the last decade. It was anticipated that as the world’s population ages, the prevalence of stroke in emerging nations will overtake other diseases as the leading cause of adult premature death and disability [7]. Animal models of cerebral ischaemia has made a significant contribution to our understanding of the pathophysiology of stroke and the creation of novel treatments [8].
Plant materials as sources of medical compounds continue to play a dominant role in the maintenance of human health since antiquity. Over 50% of all modern chemical drugs are of natural plant product origin; essential in drug development programs of the pharmaceutical industry [9]. In recent years, there has been a phenomenal rise in the interest of scientific community to explore the pharmacological actions or to confirm the veracity of claims made about herbs in various official books of herbal medicine. Despite the current preoccupation with synthetic chemistry as a vehicle to discover and manufacture drugs, the contribution of plants to disease treatment and prevention is still enormous.
A large number of people still turn to the use of plant products for treating various ailments and diseases particular in the rural areas. Flavonoids are antioxidant phytochemical compounds, consisting of flavones, flavanone, flavanols, flavonols, and flavanonols, which make up a large group of plant secondary metabolites. In spite of the heterogenous nature of the continent and a deluge of information on the composition and biological activity of many plant substances, there has been little effort devoted to the development of chemotherapeutic and prophylactic agents from these plants, therefore the evaluation of the constituents, pharmacological properties, detailed screening of bioactive substances for chemotherapeutic purposes are urgently warranted [10].
Ginkgo tree with the botanical name Ginkgo biloba, also known as the Maiden Hair tree, is a deciduous gymnosperm (family: Ginkgoaceae), native to China. Gingko biloba is a herb that can be found in other parts of the world. Ginkgos are large trees, normally reaching a height of 20 to 35 meters, usually deeply rooted and resistant to wind and snow damage. Ginkgo’s fan-shaped leaves make it one of the most easily recognizable landscape trees. The leaves with the fruits and seeds extracts have been used as herbal medicines in China, Japan, Korea, and other parts of the world. The tree, Ginkgo biloba, has long been believed to have medicinal properties and its extracts are among the most widely- sold herbal supplements in the world.
G. biloba extract prepared from Ginkgo biloba leaves, is defined as a complex mixture containing 24% Ginkgo flavone glycoside (quercetin, kaemferol, and isorhamnetin) and 6% terpene lactones (ginkgolides and bilobalides). It has been used as a therapeutic agent in some cardiovascular and neurological disorders .The chemical nature of Ginkgo biloba leaves extract containing both flavonoid and ginkgolide constituents, is responsible for its remarkable antioxidant, reactive oxygen, and nitrogen species gardens and is now valued in many parts of the world as a fungus- and insect- resistant ornamental tree. In the plant kingdom Ginkgoaceae, there is just one living species, Ginkgo biloba. In Nigeria, while the Igbos still call it ‘Ginkgo’ for short, the fruit is commonly called ‘Obi Gbogbonse’, and ‘Bishiya’ among the Hausas.
Gingko biloba, especially its leaves- are rich sources of compounds responsible with antioxidant activity. It contains high levels of flavonoids and terpenoids, which are compounds known for their strong antioxidant effects via the free radical-scavenging activity by ameliorating or neutralizing damaging effects of the free radicals. Also, some main compounds responsible for this kind of activity include kaempferol, quercetin and isorhamnetin. These flavonoids can scavenge and destroy free radicals, especially peroxide, hydrogen peroxide, hydroxyl and singlet oxygen radicals, which are connected to diseases such as atherogenesis, inflammation, etc. Ginkgo’s antioxidant content lends credence to its health-related benefits. For this reason, the naturally-occurring antioxidants in Gingko may be effective agent for different basic medical and clinical applications, hence a need for its consideration and exploration in advancing stroke research works. The aim was then to evaluate neuroprotective effects of GBE, apromising natural product of Gingko biloba leaf with high ginkglolides and flavonoids constituents, on hippocampus and cerebrum of Wistar rat with acute ischaemia induced by the bilateral common carotid artery occlusion (BCCAO).
Research Methods and Materials
Thirty adult male Wistar rats were randomly assigned to 5 study groups (n=6) and acclimatized in clean cages for a week. Group A, received Normal saline, Group B received GBE only, Group C had BCCAO only, Group D received GBE presurgery, and Group E received GBE postsurgery. The safe oral GBE daily dose of 100 mg/kg/day was administered for 14 days. 2 rats shared 1 capsule per day at average weight of 200 grams. Giloba, the soft gel capsule used, was manufactured by Mega Life Sciences Nigeria Ltd.: NAFDAC Reg. No. A7-0404L. After adequate anaesthesia at 80-100mg/ kg of intraperitoneal Ketamine, BCCAO was performed with 3/o silk suture ligation. Reperfusion was allowed after 30 minutes. Analgesia and antibiotic prophylaxis were with intramuscular paracetamol injection and topical penicillin cream. Neurobehavioral changes in spatial exploration was assessed using Y-Maze toolkit. On day 21, from onset of acclimatization, the rats were sacrificed by gentle cervical dislocation under mild anaesthesia and the whole brain harvested for histomorphological studies. The study was carried out in the Animal House, Department of Anatomy, Faculty of Basic Medical Sciences in line with the University of Ibadan Animal Care and Use Research Ethics Committee (ACUREC) guidelines.
Relevant Illustrative Diagrams (Figures 1-6)

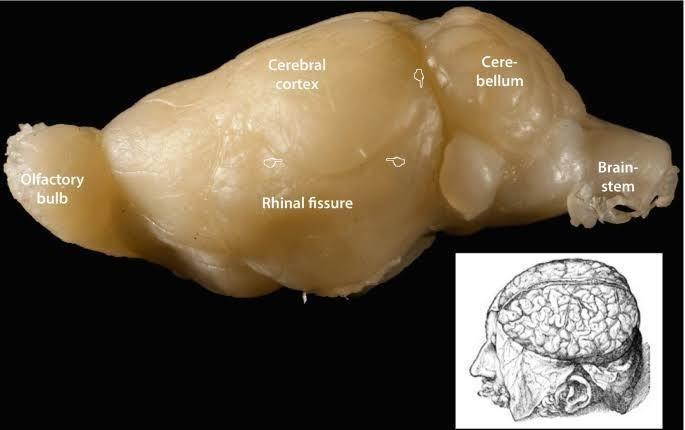
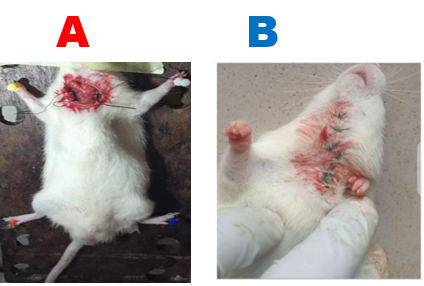

Figure 5(a): Intraop and immediate post-op status: Bilateral Common Carotid Artery Occlusion.

Figure 5(b): After full recovery from anaesthesia.

Results (Table 1) (Figures 7a, 7b)
| Group | Initial body weight (g) | Final body weight (g) | Weight gain/ loss (g) | % Weight gain/loss (%) |
|---|---|---|---|---|
| Control | 197 | 209.75 | 12.75 | 6.47 |
| GBE Only | 206 | 220.5 | 14.5 | 7.04d |
| BCCAO only | 197.5 | 181.5 | -16 | -8.1ab |
| GBE+BCCAO | 194 | 200.75 | 6.75 | 3.48bc |
| BCCAO+GBE | 201.25 | 193.25 | -8 | -3.98bc |
Table 1: Percentage body weight, body weight change in gram of the control and treated groups.
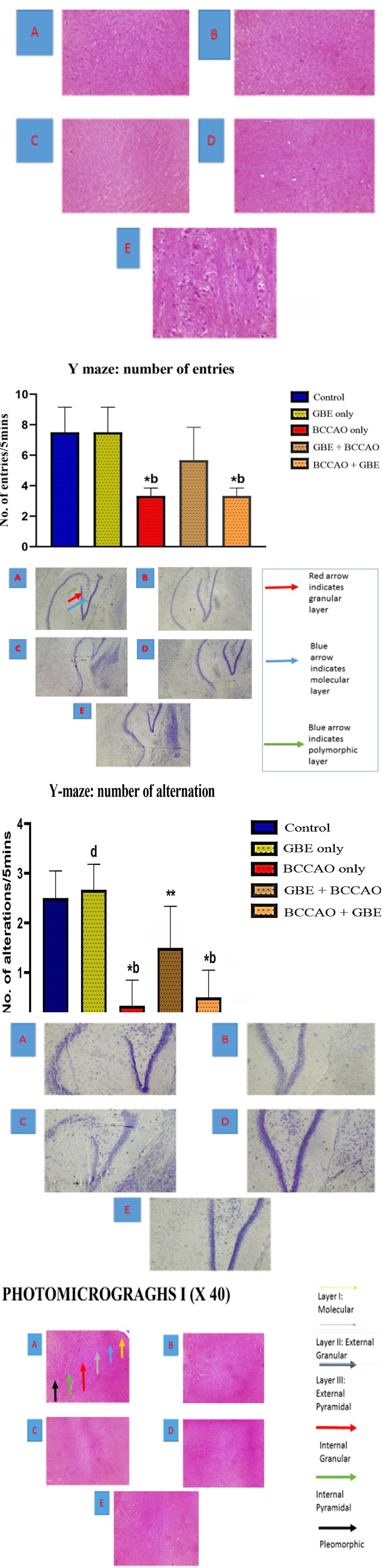
Figure 7(a): Y maze – number of entries.
Figure 7(b): Y maze- number of alterations.
Plates
Plates 1-5 are as follows:
Plate 1: Photomicrograghs I (X 40).
Plate 2: Photomicrograghs I (X 100).
Plate 3: Photomicrograghs II (X 40).
Plate 4: Photomicrograghs II (X 100).

Plate 5: Photomicrograghs II (X 400).
Discussion
Differences in Organ-to-body Weight Ratio of the Rats
The assessment of the organ- to-body weight ratio of rats in the BCCAO showed a significant increase when compared with rats in the control and GBE only groups. This may be possible indication of tissues inflammation as earlier reported by Rossi, et al. [11]. However, animal strain, age, sex, as well as environmental settings have all been reported to have an impact on animal’s organ weight [12]. In accordance to contemporary toxicity findings from Inyang et al., oral administration of GBE did not result in acute toxicity in rat at dose up to 100mg/kg body weight. In addition, result also showed significant decrease in mean body weight difference of animals in BCCAO only and BCCAO+ GBE groups when compared with other groups. This weight loss could be due to ischaemic injury which generally led to body weakness, reduced food, and water intake in the animals.
Histopathology Report of Plates
Haematoxylin & Eosin Histology Slides
Group A (Control Group): Here there are 6 distinct cellular layers of the cerebral cortex (layers I-VI) which include molecular layer (I), outer granular layer (II), outer pyramidal layer (III, inner granular layer (IV), inner pyramidal layer (V) and pleomorphic layer (VI). The pyramidal and granular cells appear normal.
Group B (Extract Only Group): The pyramidal cells and granular cells here also appear normal similar to those found in the control group.
Group C (Ischaemia Only Group): Abundance of neurons with pyknotic (shrunken) acidophilic (eosinophilic) cytoplasm and deeply stained nuclei and perineuronal vacuolations were seen indicative of ongoing neuronal injury and/or necrosis. The cerebral cortical layers are indistinct. The central zone of ischemia shows abundance of fibres with few surrounding small blood vessels.
Group D (Extract Before Ischaemia Group): Lesser number of pyknotic pyramidal and granular cells. Few small neurons are present with pale perinuclear halo of cytoplasm and deeply stained central nuclei were also seen.
Group E (Extract After Ischemia Group): Shows a few pyknotic neurons with darkly stained shrunken (pyknotic) nuclei. Some vacuoles are also present.
Cresyl Violet Histology Slides
Group A: Shows the 3 distinct layers of dentate gyrus: molecular, granular, and polymorphic layer. The granular layer comprises multiple regular rows of granular cells that appear tightly elliptical cells with basophilic cytoplasm.
Group B: Also this shows the 3 layers of dentate gyrus: molecular, granular, and polymorphic layer.
The granular layer is formed of multiple regular rows of granular cells that appear tightly elliptical cells with basophilic cytoplasm.
Group C: This has many pyknotic granular cells, vacuolations, congested blood vessels, with degenerated neurons with spindle-shaped cells.
Group D: The neuronal cells are less scattered with more neuronal cells in contact. There is increased thickness of pyramidal cell layer in the dentate gyrus of the hypocampus with decreased pyknotic neurons with shrunken and irregular nuclei.
Group E: Few distinct granular cells exist but some pyknotic neurons are still present. Normal neurons with vacuolations and scanty spindle-shaped cells are observed.
Conclusion
This study ascertains that the Ginkgo biloba extract (GBE) shows a prophylactic neuroprotective effect against oxidative stress and neuronal damage induced by bilateral common carotid artery occlusion in adult Wistar rats. In addition, the extract offers neurocognitive (spatial memory) enhancement in the rats, hence a potential memory booster in cognitive science and stroke medicine. Results reveal that the prophylactic effect of GBE when administered prior to cerebral ischaemic injury is more pronounced than when administered after trauma thereby substantiating its ameliorating potential in ischaemic stroke research. Premised on the findings of this stroke research, a further research using advanced technologies is being proposed to explore the effect of specific active component of Gingko biloba extract e.g. GBE 761 on bilateral middle cerebral artery occlusion (BMCAO) which serves to provide deeper insight into the neuroprotection of the leaf extract in stroke preventive and therapeutic medicine that is potentially translatable to clinical neurology.
Acknowledgements
My profound gratitude goes to God Almighty; my Marker, my Sustainer, ‘The Strength of the Weak’ who in his infinite mercy kept me, and supplied all my needs throughout the period of this research, making my dream a reality. I wish to express my fervent thanks and regards to my supervisor, Prof. O. Owoeye for being a mentor, a teacher and a father to me in the course of this research. Through his thorough and diligent supervision, I have acquired immense practical knowledge and skill in clinically-oriented neuroscience research. I am also grateful to all teachers of Anatomy who did not relent in instruction and direction of the study. Moreover, the contributions of the entire staff and head of the Department of Anatomy are highly appreciated. My profound gratitude also goes to my parents, Mr and Mrs Idowu E.O, for their support morally, and motivation wise and also for their prayers for me every day throughout the period of this research. My gratitude also goes to my siblings, Idowu Omowunmi Olufunke, Idowu Oluwakemi Abosede, Idowu Elizabeth Oluwayemisi and my extended relations. Your moral support throughout my postgraduate program is well appreciated. I wish to appreciate Mr Osuntade, Mrs Adunola, Mrs Ogunsola and Mr Olubanke for their immense assistance throughout this research. I appreciate my friends and colleagues who in one way or the other contributed to the success of this research, I am deeply grateful and God bless you all.
Declaration
No personal or financial conflict of interests exists.
References
-
Woranan K, Jintanaporn W, Terdthai T, Supaporn M, Panakaporn W, et al. (2013) Cerebroprotective effect of Moringaoleifera against focal ischaemia stroke induced by middle cerebral artery occlusion. Oxid Med Cell Longev 2013: 951415.
-
Charisma DS, Angela HS (2024) Cerebral ischaemia. In: Statpearls. Treasure Island (FL): Statpearls publishing.
-
Ren C, Yan Z, Wei D, Xuwen G, Checn X, et al. (2009) Limb remote ischaemic postconditioning protects against focal ischemia in rats. Brain Res 1288: 88-94.
-
E.O Idowu, Owoeye O (2024) Anatomy in Health and Disease: Exploring the Potentials of Microscropy and Anthropometry. ASN UI 2024; 20th Annual Scientific Conference and General meeting (October 7-9, 2024); University of Ibadan, Ibadan, Nigeria.
-
Luciana C, Joseph T, Marc F (2017) Acute Ischemic Stroke Therapy Overview. Cir Res 120(3): 541-558.
-
Gregory WA, Louis RC, Donald E, Pierre BF, Mohr JP, et al. (2002) Transient ischemic attack -Proposal for a new definition. N Engl J Med 347(21): 1713-1716.
-
Rong M, Qian X, Yong L, Zhuoping C, Mihong R, et al. (2020) Animal models of cerebral ischemia: A review. Biomed Pharmacother 131: 110686.
-
Boyko M, Kuts R, Gruenbaum BF, Tsente P, Grinshpun J, et al. (2019) An Alternative Model of Laser- Induced Stroke in the Motor Cortex of Rats. Biol proced Online 21: 9.
-
Burton GW, Hughes L, Ingold KU (1983) Antioxidant activity of phenols related to vitamin E. Are there chain- breaking antioxidants better than. alpha.-tocopherol? Journal of the American Chemical Society 105(18): 5950-5951.
-
Farombi EO (2004) African indigenous plants with chemotherapeutic potentials and biotechnology approach to the production of bioactive prophylactic agents. African Journal of Biotechnology 2(2): 662-667.
-
Rossi A, Serraino I, Dugo P, Paola RD, Mondello L, et al. (2003) Protective effects of anthocyanins from blackberry in rat model of acute lung inflammation. Free Radic Res 37(8): 891-900.
-
Ying P, Yunen L, Xiaodong X (2013) Change trends of organ weight background data in Sprague Dawley rats at different ages. J Toxicol Pathol 26(1): 29-34.
- Pattern of Breast Lesions in Ovu Inland, Delta State, South Southern Nigeria
- Morphometric Analysis of the Human Femur: Exploring Platymetric and Robusticity Indices Among the Nigerian Population
- Anatomical Variation of Arteria Lusoria: Clinical Implications for Dysphagia Lusoria and Surgical Risk
- Morphometric Study of the Vertebral Body and Pedicle of Typical Cervical Vertebrae Using Radiological Image
- Epigenetic Mechanisms Driving Human Evolutionary Changes
- Communicating Neuroanatomical Fibers in Health and Diseases