Communicating Neuroanatomical Fibers in Health and Diseases
Background: Combining neuroanatomical fiber information with other types of neuroimaging and genetic data can lead to a more comprehensive understanding of brain function and pathology. Variations in the branching patterns of the brachial plexus and the division of the sciatic nerve into the tibial and common fibular nerves has been documented in numerous studies, although not extensively in Ethiopia. The brachial plexus is formed by the ventral roots of spinal nerves from C5 to T1. Meanwhile, the sciatic nerve, which originates from the sacral plexus divides into the tibial and common fibular nerves at various points along its pathway. Given the significant implications of neural variations for enhancing medico legal practices, understanding these variations is crucial for making accurate diagnosis. Consequently, study examined different neuroantomical variants in Ethiopia. Objectives: To examine variations in the neural system connection and their clinical implications in the Ethiopian population and provide mechanistic insights into how different brain regions communicate and disruptions in these communications can lead to cognitive and behavioral symptoms. Methods and Materials: This research was carried out in a randomly selected medical institutions between January 2015 and February 2016. Preserved and carefully maintained human bodies were dissected by medical students, adhering to the protocols outlined in Grant’s Dissection Principles and Cunningham’s Manual of Practical Anatomy. The dissections took place in anatomy laboratory, with a specific focus on detecting any anatomical variations, particularly in the neural system of the human body. Results: In this study, we observed communication between the musculocutaneous nerve and the median nerve occurred in 6.3% of the sampled cases. Moreover, communication between the radial nerve and the ulnar nerve was found in 2.1% of the cases. Furthermore, variations in the pelvic division of the sciatic nerve were noted in 6.3% of the sampled cases from Ethiopia. Conclusion: We discovered a nerve responsible for communication within a specific part of the human body. Recognizing such communicating nerve fibers and their pathways is essential for clinicians to effectively diagnose sensorimotor symptoms. This understanding is also vital for neurologists, surgeons, and orthopedists in handling cases of nerve entrapment syndromes, carrying out post-traumatic assessments and undertaking exploratory procedures.
Abbreviations
MCN: Musculocutaneous Nerve; MN: Median Nerve; RN: Radial Nerve; UN: Ulnar Nerve; SCN: Sciatic Nerve; CN: Communicating Nerve; DTI: Diffusion Tensor Imaging.
Background
The brachial plexus is formed by the union of ventral roots of spinal nerves (C5-T1) unless it is pre-or post-fixed. Normally, the two upper roots unite together and give rise to upper trunk. The C7 root continuous to become the middle trunk and the two lower roots C8 and T1 becomes the lower trunk. Each trunk splits into anterior and posterior divisions. The divisions reunite to form three cords lying in two anatomical planes; the anterior plane includes lateral and medial cords whereas the posterior plane consists of the posterior cord. Musculocutaneous (MCN) arises as terminal branch of lateral cords of brachial plexus, after supplying the coracobrachialis muscle, it pierce the muscle and runs down between biceps brachii and brachialis muscle supplying all muscles of the anterior compartment of the arm. Finally, MCN appears superficial lateral to the tendon of biceps bachii and becomes lateral cutaneous nerve of the forearm [1]. Median nerve (MN) originates with two roots, lateral root from lateral cord (C5, C6 and C7) and medial root from medial cods (C8 and T1). It runs at first lateral to the upper half of the brachial artery, then crosses the artery nearly at the middle of the arm and comes medial to the brachial artery in the lower half of the arm. In its course within the arm it communicates with MCN at various distances [2]. For instance, communications between fibers of terminal branches of brachial plexus such as communicating fibers of MCN with MN with differing patterns or types [2, 3]. Several studies report variants of brachial plexus and its terminal branches in different populations other than Ethiopia [4].
Another neural variant reported in the lower limb was the pelvic division of sciatic nerve (SCN). SCN is a broadest, thickest and the largest nerve of human body, arising from sacral plexus [5]. It is formed in the pelvis by joining anterior rami of L4 - S3 spinal nerve roots. It is almost 2 cm wide at its origin near the sacral plexus [6]. Normally, it emerges through the greater sciatic foramen, leaves pelvis and enters into gluteal region by passing below piriformis as a single nerve encompassed by a single epineurium. It divides subsequently into two terminal nerves: tibial and fibular nerves usually at superior angle of popliteal fossa [7]. Several reports indicated variants in the course and distribution of SCN. The main variations were the relationship of the nerve to piriformis and unusual of division of the nerve at different sites [7]. Reports indicate its high division while still in the pelvis into its terminal branches that leave pelvis in a number of ways. Patel, et al. [8], classified them into different types in relations to piriformis. High pelvic division of sciatic nerve is usually unilateral or bilateral, which will have clinical implications in piriformis syndrome, popliteal block anesthesia and understanding the etiologies of sciatica [6]. Nevertheless, reports are scanty in Ethiopia. Advances in neuroimaging, such as diffusion tensor imaging (DTI) and tractography, allow for more detailed and accurate mapping of neural fibers. This helps in understanding the brain’s structural connectivity in ways that were previously not possible.
Methods and Materials
This study was conducted in six randomly chosen Ethiopian medical institutions; Jimma, Addis Ababa, Wollega Universities as well as Bethel, Africa and Sante Medical Colleges. It was carried out from January 2015 to February 2016. The small sample size would also be explained due to lack of many unclaimed human bodies, distances for implementation of this work and advanced nature of the study. It was an experimental study based on human bodies in governmental and private medical schools in the country. It was conducted after an ethical approval by institutions involved (ProtocolDAERC-0024/2014). Carefully preserved and controlled bodies were dissected for undergraduate medical students in accordance with guidelines of Grant’s dissection principle and Cunningham’s manual of practical Anatomy. Immature, injured, distorted and claimed bodies were excluded from the study. In all cases, critical observation, careful dissection and imaging were pursued in a total of 24 unclaimed bodies that will be 48 for identification of structures in both sides of both gender and all regions of human body. Accordingly, the superficial and deep fascia was removed so as to expose the bones, muscles and neurovascular bundles. These structures were carefully handled in the laboratories and seen for the presence of any neuroantomical variations with special focus on the specified regions of human body. Findings of the present investigation were indicated in result sections.
Statistical Analysis
Results of the study were analyzed using one way ANOVA. Confidence interval (95%) was considered as statically significant source of neural variations in our sampled population.
Results and Observations
Communicating fibers of the musculocutaneous and median nerve as well as between radial nerve and the ulnar nerve in the arm
Table 1 shows summary of variants in neural system. Our findings show communicating fibers of MCN with MN
in the arm at proportion of 6.3%. The communications were bilateral in 4.2% of the population, whereas 2.1% of the cases were unilateral. MCN arising as the terminal branch of lateral cord pierce into coracobrachialis and appears superficially (Figures 1a-1d). MCN, after giving communicating fiber to MN in the upper part of the arm (Figure 1a and 1b), pieces the biceps brachii and runs between biceps brachii and brachialis supplying those muscles. In other communicating branches, the MCN pierce the coracobrachialis and runs down under cover of biceps brachii after giving the communicating fibers that communicate with MN near the insertion of coracobrachialis.
| Number of Bodies | Gender | Variations Bilateral**/ Unilateral+ | Observations | No. of Cases/ Bodies | Distributions | Percentage | |
|---|---|---|---|---|---|---|---|
| M | F | ||||||
| 24 | 20 | 4 | Communications of MCN and MN | **+ | Mar-48 | 0.063 | 6.30% |
| 24 | 20 | 4 | Communication of RN and UN | + | Jan-48 | 0.021 | 2.10% |
| 24 | 20 | 4 | Pelvic division of Sciatic nerve | **+ | Mar-48 | 0.063 | 6.30% |
Table 1: Neuroanatomical Variations and their Frequencies. • **: Bilateral; +: Unilateral; M: Male F: Female

Figure 1a: Image showing communicating fibers between the musculocutaneous and median nerve in the arm. MN: median nerve; MCN: musculocutaneous nerve; CN: communicating nerve; BA: brachial artery; BB: biceps brachii muscle.
Figure 1b: Image showing communicating fibers between the musculocutaneous and median nerve in the arm. MN: median nerve; MCN: musculocutaneous nerve; CN: communicating nerve; BA: brachial artery; BB: biceps brachii muscle.
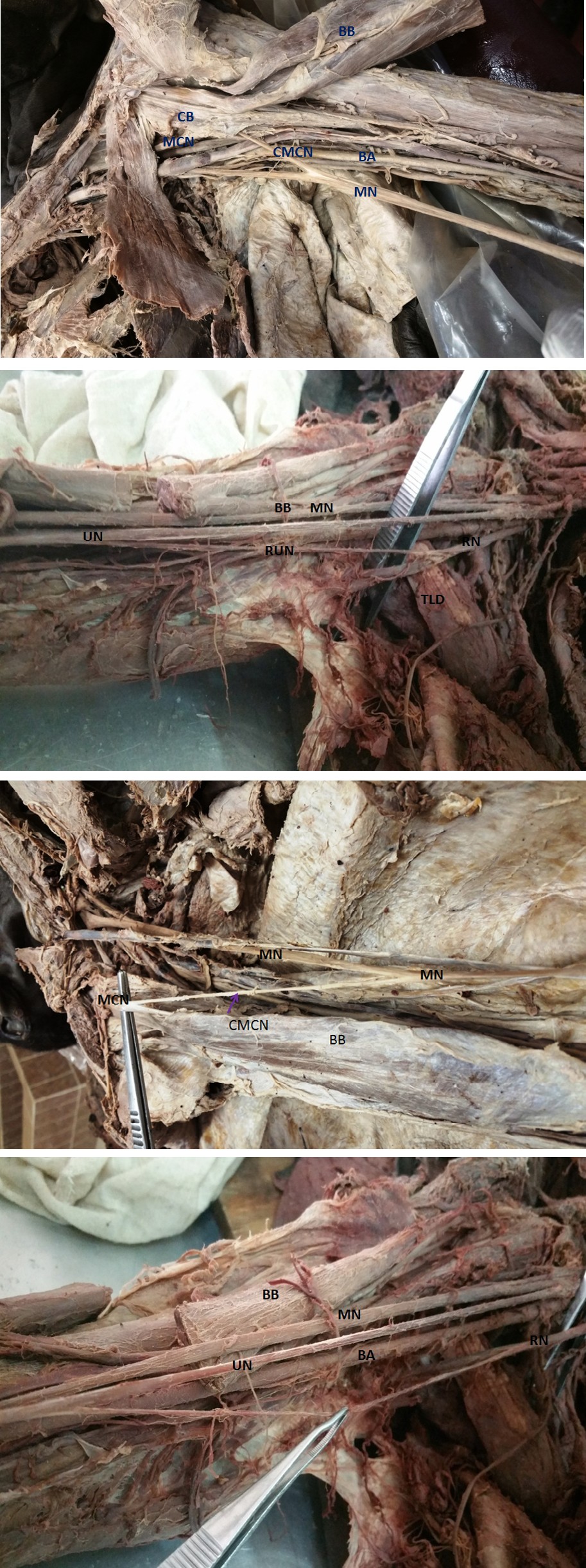
Figure 1c: Image showing communicating fibers of MCN and MN (left arm). CB: Coracobrachialis; MCN: Musculocutaneous nerve; CMCN: Communicating branch of musculocutaneous nerve; MN: Median nerve; BA: Brachial artery; BB: Biceps brachii.
Figure 1d: Image showing communicating fibers of MCN and MN (right arm).
CB: Coracobrachialis; MCN: Musculocutaneous nerve; CMCN: Communicating branch of musculocutaneous nerve; MN: Median nerve; BA: Brachial artery; BB: Biceps brachii.
MN originating from two roots, lateral and medial roots, runs down medial to MCN and lateral to the upper half of the brachial artery into the arm. So it was investigated that the MN receives the communication fibers near the middle of the arm from MCN as in shown (Figures 1a and 1b). The communicating branch, originating from MCN, runs obliquely from lateral to medial where it joins the MN and may considered to be the third root of the MN.
Finding of the present study also show communication between radial nerve (RN) and ulnar nerve (UN). RN originates as the larger of the terminal branches of posterior cord. Leaves the axilla at lower border of teres major and enters into triangular interval. In the axilla it gives communicating branch that runs down into the arm to join the UN near the middle of the arm (Figures 1e & 1f).
Figure 1e: Image showing the communicating fibers between the ulnar and radial nerves.
MN: median nerve; RN: radial nerve; UN: ulnar nerve; RUN: radiulnar nerve; CB: communicating branch; TLD: latissimus dorsi; BB: biceps bachii muscles.
Figure 1f: Image showing the communicating fibers between the ulnar and radial nerves. MN: median nerve; RN: radial nerve; UN: ulnar nerve; RUN: radiulnar nerve; BB: biceps bachii The UN originate as the terminal branch of medial cord in the axilla it runs down into the arm medial to the third part of axillary artery in the axilla and brachial artery in the arm. Near the middle of the medial aspect of the arm, UN receives the communicating branch from the radial nerve. This is the rare variations where anterior division of the brachial plexus communicates with posterior division. So this communicating nerve thought to connect the anterior plane of the arm with the posterior plane. This communication investigated in 2.1% of the cases.
Variation in Pelvic Division of Sciatic Nerve
High pelvic divisions of sciatic nerves were observed only in one body. That means two gluteal regions have got high pelvic division of sciatic nerves, about 0.063 of the sampled cases and 6.3% of the population (Table 1). In this study, the sciatic nerves bilaterally separate into common fibular nerve and tibial nerve in the pelvis. The common fibular nerves leave the pelvis into gluteal region through greater sciatic foramen pierces into the piriformis. Whereas the tibial nerve leaves the pelvis into gluteal region through greater sciatic foramen below piriformis. Both nerves independently descend down to posterior thigh (Figures 2a- (left) and Figure 2b (right), Figures 2c and 2d.

Figure 2a: Image showing the pelvic division of the fibers of left sciatic nerve. P: Piriformis; IGN: Inferior gluteal nerve; CFN: common fibular nerve; TN: Tibial nerve; DF: Quadratus femoris
Figure 2b: Image showing the pelvic division of the fibers of right sciatic nerve. P: Piriformis; CFN: common fibular nerve; TN: Tibial nerve; DF: Quadratus femoris
Figure2c: Image showing the pelvic division of right sciatic nerve. P: Piriformis; CFN: common fibular nerve; TN: Tibial nerve; DF: Quadratus femoris.
Figure 2d: Image showing the pelvic division of left sciatic nerve. P: Piriformis; SN: Sciatic Nerve; DF: Quadratus femoris.
Discussion
Variations in the formation and branching patterns of brachial plexus embrace an important anatomical as well as clinical scenario. Previous studies have revealed frequent variations in the brachial plexus nerves. Our results strongly support these earlier findings from Europe, Asia, and Africa. Research has documented communication between peripheral branches of the brachial plexus, with incidence rates varying from 5% to 63.5%. Moreover, it has been observed that high divisions of the spinal nerves in the pelvis can occur either bilaterally or unilaterally, with the other nerve maintaining its normal trajectory Neuroanatomical variation of these nerves in the axilla or in the arm is required as there has been an increasing frequency of surgeries performed in these areas of the body [9]. Studies show common variations of nerves of brachial plexus [10]. Our findings are consistent with the previous reports made in Europe, Asia and Africa [2, 4, 11]. Various authors showed communication between the MN and MCN with an incidence ranges from 5% to 63.5% [4]. They also show communicating fibers of MCN and MN usually run downward and medially after their origin [11]. Anastomotic branches arising from the median nerve and then joining the MCN were rare [2]. Our results in Ethiopians is in line with the investigations of Kumar, et al. [2] in Indians.
Ushakothandaraman and Lokanadham [12] pointed that the communications between MN and MCN can be explained five different types suggesting correspondence of similar origins among this population. In type I, there is no communication between the MN and the MCN; in type 2, the fibres of the medial root of the MN pass through the MCN nerve and join the MN in the middle of the arm, whereas in type 3, the lateral root fibres of the MN pass along the MCN and after some distance, leave it to form the lateral root of the MN. In type 4, the MCN fibres join the lateral root of the MN and after some distance the MCN arises from the MN. In type 5, the MCN is absent and the entire fibres of the MCN pass through the lateral root and fibres to the muscles supplied by MCN branch out directly from the MN.
Bergman, et al. [13] reported possible communication of fibers between RN and UN in the arm which agrees with our results in Ethiopia, where the communicating branch arises from RN, and then run down obliquely to join the UN. However, a percentage value for the communications between radial and ulnar nerves on the arm or forearm is missing in the literature [14]. Leis and Well [15] reported the communication of superficial branch of radial nerve with dorsal cutaneous branch of UN on the dorsal surface of the hand and RN provided 16% cutaneous innervation to the dorsum of the hand. They also indicated that the type communicating branch most likely sensorial. However; our finding indicate as it is most probably both sensorial and motor as the communication is in the arm and the distribution of the UN is in the forearm and hand.
Another neural system finding was division of SN in the pelvis, where the common peroneal nerve passed between the two heads of the piriformis and the tibial nerve followed the normal course as described in several findings. Mustafa, et al. [16] indicated the existence of many variations in SN division especially higher divisions. It was indicated that there are different types of high divisions of SN within pelvis either bilateral or unilateral in which case the other one is remain in the normal course. Beaton and Anson [17] classified variations of the piriformis and SN into six different types of higher divisions which were observed in different studies of different researchers. These includes: Type 1: Undivided nerve below undivided muscle; Type 2: Divisions of nerve between and below undivided muscle; Type 3: Divisions above and below undivided muscle; Type
4: Undivided nerve passed between heads of the piriformis; Type 5: Divisions between and above heads; Type 6: Undivided nerve above undivided muscle [17]. However, the present result is somehow different from Beaton and Anson [17] classifications in which the divided nerve between and below divided piriformis muscle. The reported incidence of SN division before its exit in the gluteal region varies from 4% to 20.9% across different studies.
In our Ethiopian case, the incidence of SN division was within the range of different studies which is about 6.3%. This high pelvic division results in sciatica, nerve injury during deep intramuscular injections, piriformis syndrome, failed SN block in anesthesia and injury during posterior hip operations [5, 6]. Indeed, linking the structural connectivity of neural fibers to clinical outcomes, researchers can better understand how disruptions in specific neural pathways contribute to neurological and psychiatric conditions, such as stroke, Alzheimer’s disease, or Schizophrenia [18, 19]. Insights into neuroanatomical fibers can lead to more personalized approaches to diagnosis and Treatment [20]. For example, understanding the specific pathways affected in a patient with epilepsy might lead to more targeted surgical interventions.
Conclusion
Our study unveiled the existence of a communicating nerve (CN) responsible for facilitating communication within a specific part of the human body, both in health and disease. Understanding of communicating neuroanatomical fibers and their clinical implications is relevant in its focus on understanding and mapping the connections between different areas of the brain and how these connections influence both normal brain function and various neurological disorders. This approach often involves advanced imaging techniques and computational methods to visualize and analyze neural pathways. Meanwhile, looking at nervous system variants will help clinicians to make proper diagnosis of sensorimotor symptoms. For instance, communications of MCN and MN may be of considerable significance to neurologists, surgeons and orthopaedicians when dealing with patients of nerve entrapment syndromes, posttraumatic evaluations and exploratory interventions. Variants of higher division of the sciatic nerve and the its course are of paramount importance in surgical manipulation, rehabilitation, anesthesia and flap dissections.
References
-
Lokanadham S, Devi VS (2012) Anatomical variation- Communication between musculocutaneous nerve and median nerve. Folia Med (Plovdiv) 3(1): 1436-1438.
-
Kumar N, Guru A, Souza MRD, Patil J, Nayak SB (2013) Incidences and Clinical Implications of Communications between Musculocutaneous Nerve and Median Nerve in the Arm-A Cadaveric Study. West Indian Med J 62(8): 744 -747.
-
Thomas HR, Potu BK, Bhat KMR, Margaret B, Madhav V, et al. (2010) Variation in the termination of musculocutaneous nerve. International Journal of Anatomical Variations 3: 78-79.
-
Uyarolu FG, Kayallu G, Ertürk M (2008) Anastomotic branch from the median nerve to the musculocutaneous nerve: A case report. International journal of experimental and Clinical Anatomy 2: 63-66.
-
Saritha S, Kumar PM, Supriya G (2012) Anatomical variations in the bifurcation of the sciatic verve, A Cadaveric Study and its Clinical Implications. Anatomy and physiology2(5): 1-4.
-
Shastrakar R, Nakhate M, Sawant VG (2015) Study of variation in the high division of sciatic nerve and its relationship with the piriformis muscle. Medico Research Chronicles. 2 (3): 359-365.
-
Shewale AD, Karambelkar RR, Umarji BN (2013) Study of variations in the divisions, course and termination of the sciatic nerve. JKIMSU 2(1): 62-28.
-
Patel S, Shah M, Vora R, Zalawadia A, Rathod SP (2011) A variation in the high division of the sciatic nerve and its relation with piriformis muscle. National Journal of Medical Research 1(2): 27- 30.
-
Chauhan R, Roy TS (2002) Communication between the median and musculocutaneous nerve- A case report. Journal of Anatomical Society of India 51(1): 72-75.
-
Remya K, Krishnamurthy A, Kavitha K (2011) Communication between the musculocutaneous and median nerve: Occurrence on both sides. Nitte University Journal of Health Sciences 4: 55-56.
-
Sachdeva K, Singla RK (2011) Communication between median and musculocutaneous nerve. Journal of Morphological Sciences 28(4): 246-249.
-
Ushakothandaraman, Lokanadham S (2014) Types of Communications between Musculocutaneous nerve and median nerve. Journal of Clinical and Biomedical Sciences 4(2): 300.
-
Bergman RA, Afifi AK, Miyauchi R (2009) Radial nerve. Illustrated Encyclopedia of Human Anatomic Variation: Opus III: Nervous System: Plexuses.
-
Loukas M, Louis RG, Wartmann CT, Tubbs RS, Turan- Ozdemir S, et al. (2008) The clinical anatomy of the communications between the radial and ulnar nerves on the dorsal surface of the hand. Surgical and Radiological Anatomy 30: 85-90.
-
Leis AA, Wells KJ (2008) Radial nerve cutaneous innervation to the ulnar dorsum of the hand. Clin Neuropysiol 119: 662-666.
-
Mustafa G, Cihan Y, nar A, Süleyman T, Sait N (2009) Variations in the high division of the sciatic nerve and relationship between the sciatic nerve and the piriformis. Turkish Neurosurgery 19(2): 139-144.
-
Beaton LE, Anson BJ (1937) The relation of the sciatic nerve and its subdivisions to the piriformis muscle. Anatomy Research 70: 1-5.
-
Rushmore, R. J., Bouix, S., Kubicki, M., Rathi, Y., Yeterian, E. H., & Makris, N. (2020). How Human Is Human Connectional Neuroanatomy?. Frontiers in neuroanatomy, 14, 18.
-
Schwabl, C., Hörmann, R., Strolz, C. J., Drakonaki, E., Zimmermann, R., & Klauser, A. S. (2023). Anatomical Variants of the Upper Limb Nerves: Clinical and Preoperative Relevance. Seminars in musculoskeletal radiology, 27(2), 129–135.
-
Chu, M., Jiang, D., Liu, L., Nie, B., Rosa-Neto, P., Chen, K., & Wu, L. (2023). Clinical relevance of disrupted topological organization of anatomical connectivity in behavioral variant frontotemporal dementia. Neurobiology of aging, 124, 29–38.
- Pattern of Breast Lesions in Ovu Inland, Delta State, South Southern Nigeria
- Morphometric Analysis of the Human Femur: Exploring Platymetric and Robusticity Indices Among the Nigerian Population
- Anatomical Variation of Arteria Lusoria: Clinical Implications for Dysphagia Lusoria and Surgical Risk
- Morphometric Study of the Vertebral Body and Pedicle of Typical Cervical Vertebrae Using Radiological Image
- Epigenetic Mechanisms Driving Human Evolutionary Changes
- Neuroprotective Effects of Ginkgo Biloba Extract on Bilateral Common Carotid Artery Ischaemic Stroke Induced in Wistar Rat