Pattern of Breast Lesions in Ovu Inland, Delta State, South Southern Nigeria
Background: The breast is a site of various pathological changes, encompassing both benign and malignant lesions. Early detection and management of these lesions are essential for improving patient prognosis. Aim: While studies on breast lesions have been conducted in various parts of Nigeria, data on this subject are scarce in the studied area. Therefore, this study investigated the patterns of breast lesions in Ovu Inland, Delta State, South-South Nigeria. Materials and Methods: This study was a retrospective histopathological review of 71 breast lesions. Descriptive statistics were used to illustrate the prevalence of breast lesions, while a Chi-square test assessed the association between breast lesions, age, and laterality. Results: Benign lesions (86.2%) were more common than malignant ones (13.8%) in the studied population. Neoplastic benign fibroadenoma (36.6%) and malignant invasive ductal carcinoma (5.6%) were the most common benign and malignant lesions, respectively. The third decade of life recorded the highest incidence of breast lesions (31%). Right breast lesions (45.1%) were more frequent than left breast lesions (35.2%). No significant association was found between breast lesions, age, and laterality (p= 0.254; 0.364). Conclusion: Neoplastic benign fibroadenoma peaked in the second and third decades, while neoplastic malignant invasive carcinoma was more common in the fourth decade.
Introduction
The human breast is a modified apocrine gland covered by skin and subcutaneous tissue [1]. It rests on the pectoralis major muscle and consists of ducts, lobules, luminal and myoepithelial cells, as well as interlobular and intralobular stroma. These components are sources of both benign and malignant lesions [2, 3]. However, most breast lesions are benign and encompass a heterogeneous array of disorders, including developmental abnormalities, epithelial and stromal proliferations, neoplasms, and inflammatory lesions [4, 5, 6, 7, 8, 9]. Several factors contributing to benign breast lesions have been documented [10, 11]. According to Richard and Robert [10], observations in women who used estrogen or anti-estrogen drugs suggest that hormonal factors play a role in the development of benign lesions. This was supported by an earlier study, which noted an increase in these lesions among postmenopausal women who had received estrogen, with or without progestins, for over eight years [11]. Other risk factors include family history, mutations in the BRCA1 or BRCA2 genes [12, 13], and loss of heterozygosity caused by DNA deletions [14]. These lesions are often multifocal, with each focal region showing loss of heterozygosity at different DNA sites [10]. The BRCA1 and BRCA2 genes regulate the cell cycle, and mutations in these genes have also been established as risk factors for malignant breast lesions [12]. While benign lesions encompass a variety of histopathological types, only a few have significant premalignant potential [15]. The most important of these are atypical ductal hyperplasia, lobular hyperplasia, and carcinoma in situ [16]. Diagnosis of these lesions presents varying degrees of cancer risk [16]. It is estimated that proliferative breast lesions may become invasive in the same breast within an average period of 11 years [17]. Therefore, distinguishing benign from malignant lesions is crucial for appropriate treatment. The “triple test” used to evaluate breast lesions includes physical examination, radiology, and cytopathology [18]. Although studies on breast lesions have been conducted in various parts of Nigeria [4, 5, 6, 8, 12], there is limited data from the studied area. This study aimed to investigate patterns of breast lesions in Ovu Inland, Delta State, South-South Nigeria.
Methodology
This study was a retrospective histopathological review of 71 breast lesions diagnosed at a pathology laboratory in Ovu Inland, Delta State, Nigeria. Biopsy samples were initially fixed in 10% formal saline and processed using a tissue processor. Embedded sections were stained with Hematoxylin and Eosin (H&E) for histopathological evaluation. One of the authors, a histopathologist, reviewed the slides, and breast lesions were classified into inflammatory, proliferative, neoplastic, and other categories. A Chi-square test was used to determine the association between breast lesions, age, and breast laterality. Ethical approval was obtained from the Faculty of Basic Medical Sciences, Delta State University.
Results
Table 1 showed a total of 71 breast lesions observed, of which 1.4% each were degenerative changes, dysplastic squamous tissue, epithelial cyst, fibroma, galactocele, and gynecomastia. A total of 1.4%, 4.2%, 1.4%, and 2.8% were observed for inflammatory fat necrosis, granulomatous mastitis, intralobular mastitis, and periductal mastitis, respectively. Further findings showed that neoplastic benign fibroadenoma and tubular adenoma accounted for 36.6% and 5.6% of the breast lesions.
We also reported 12.7% and 1.4% neoplastic malignant invasive ductal carcinoma and lobular carcinoma lesions, respectively. Pregnancy-like changes and unremarkable tissue each accounted for 1.4% of the breast lesions. Proliferative duct ectasia and fibrocystic change had 14.1% and 1.4%, respectively. Comparing benign and malignant lesions, we observed that 13.8% were malignant while 86.2% were benign.
Table 2 illustrates the frequency of age groups observed from this study. The highest percentages were found within the 3rd, 4th and 5th decades. The least age observed for breast lesions were individuals with unspecified age Table 3 shows that participants with lesions in the second decade had 1.4% each for inflammatory fat necrosis, proliferative ductal hyperplasia, proliferative duct ectasia, neoplastic benign lesions, galactocele, and degenerative changes. Neoplastic benign fibroadenoma (12.7%) was also observed in this decade. Findings also indicate that the third decade had the highest number of lesions (31%) in the population studied. Further findings revealed that the fourth and fifth decades recorded 5.6% each for proliferative fibrocystic changes and neoplastic malignant invasive ductal carcinoma as the most predominant lesions. A total of 1.4% each for neoplastic malignant lobular carcinoma, inflammatory periductal mastitis, and fat necrosis was observed in participants within the sixth decade. The sixth and seventh decades recorded 2.8% and 4.2%, respectively, for proliferative fibrocystic changes and neoplastic malignant invasive ductal carcinoma as the common lesions. The Chi-square test showed no significant association between breast lesions and age.
Findings from Table 4 show that 45.1% of breast lesions were observed on the right side, while 35.2% were on the left side. The Chi-square test indicated no significant association between breast lesions and the side on which they occurred.
Table 5 shows unilateral and bilateral breast lesions among the respective age groups in the studied population. Findings indicated that neoplastic benign fibroadenoma and tubular adenoma occurred bilaterally in individuals aged 21- 30 years. Proliferative fibrocystic changes were also observed bilaterally in individuals aged 31-40, 41-50, and 51-60 years. Further findings revealed that neoplastic malignant ductal carcinoma occurred bilaterally in individuals aged 41-50 and 61-70 years. Breast lesions that occurred unilaterally include inflammatory chronic mastitis and intralobular mastitis, observed in individuals aged 31-40. Proliferative ductal hyperplasia, duct ectasia, galactocele, and epithelial cyst occurred unilaterally in individuals aged 11-20 years.
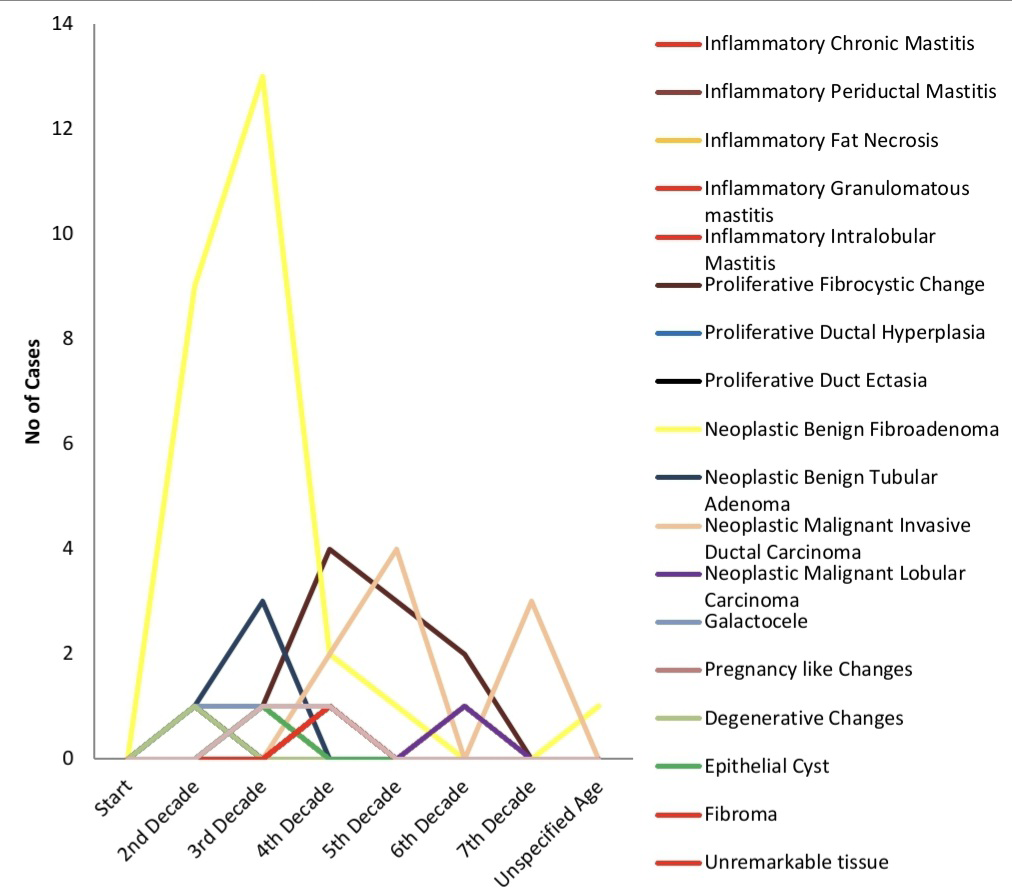
Figure 1 illustrates the occurrence of breast lesions across different decades. A peak was observed in the 2nd and 3rd decades for neoplastic benign fibroadenoma, compared to the 4th decade, where neoplastic malignant invasive carcinoma was predominant. There was a decline in the occurrence of neoplastic malignant invasive carcinoma in the 6th decade.
| Pattern of Breast Lesions | Frequency | Percent |
|---|---|---|
| Degenerative Changes | 1 | 1.4 |
| Dysplastic Squamous Tissue | 1 | 1.4 |
| Epithelial Cyst | 1 | 1.4 |
| Fibroma | 1 | 1.4 |
| Galactocele | 3 | 4.2 |
| Gynaecomastia | 2 | 2.8 |
| Inflammatory Chronic Mastitis | 1 | 1.4 |
| Inflammatory Fat Necrosis | 3 | 4.2 |
| Inflammatory Granulomatous mastitis | 1 | 1.4 |
| Inflammatory Intralobular Mastitis | 1 | 1.4 |
| Inflammatory Periductal Mastitis | 2 | 2.8 |
| Neoplastic Benign Fibroadenoma | 26 | 36.6 |
| Neoplastic Benign Tubular Adenoma | 4 | 5.6 |
| Neoplastic Malignant Invasive Ductal Carcinoma | 9 | 12.7 |
| Neoplastic Malignant Lobular Carcinoma | 1 | 1.4 |
| Pregnancy like Changes | 1 | 1.4 |
| Proliferative Duct Ectasia | 1 | 1.4 |
| Proliferative Ductal Hyperplasia | 1 | 1.4 |
| Proliferative Fibrocystic Change | 10 | 14.1 |
| Unremarkable tissue | 1 | 1.4 |
| Total | 71 | 100 |
Table 1: Distribution of breast lesion patterns in the studied population.
| Age Groups | Frequency | Percent |
|---|---|---|
| 11-20years | 15 | 21.1 |
| 21-30years | 22 | 31 |
| 31-40years | 17 | 23.9 |
| 41-50years | 8 | 11.3 |
| 51-60years | 5 | 7 |
| 61-70years | 3 | 4.2 |
| Unspecified age | 1 | 1.4 |
| Total | 71 | 100 |
Table 2: Age distribution in the studied population.
| Pattern of Breast Lesions | Age group | |||||||
|---|---|---|---|---|---|---|---|---|
| 11_20 | 21-30 | 31-40 | 41-50 | 51-60 | 61- 70 | Unspecified Age | Chi- square | |
| Inflammatory Chronic Mastitis | 1 (1.4) | |||||||
| Inflammatory Periductal Mastitis | 1(1.4) | 1(1.4) | ||||||
| Inflammatory Fat Necrosis | 1(1.4) | 1(1.4) | 1(1.4) | |||||
| Inflammatory Granulomatous mastitis | 1(1.4) | |||||||
| Inflammatory Intralobular Mastitis | 1(1.4) | |||||||
| Proliferative Fibrocystic Change | 1(1.4) | 4 (5.6) | 3(4.2) | 2 (2.8) | 0.254 | |||
| Proliferative Ductal Hyperplasia | 1(1.4) | |||||||
| Proliferative Duct Ectasia | 1(1.4) | |||||||
| Neoplastic Benign Fibroadenoma | 9 (12.7) | 13 (18.3) | 2 (2.8) | 1(1.4) | 1(1.4) | |||
| Neoplastic Benign Tubular Adenoma | 1(1.4) | 3 (4.2) | ||||||
| Neoplastic Malignant Invasive Ductal Carcinoma | 2 (2.8) | 4 (5.6) | 3 (4.2) | |||||
| Neoplastic Malignant Lobular Carcinoma; | 1(1.4) | |||||||
| Galactocele | 1(1.4) | 1(1.4) | 1(1.4) | |||||
| Pregnancy like Changes | 1(1.4) | |||||||
| Degenerative Changes | 1(1.4) | |||||||
| Epithelial Cyst | 1(1.4) | |||||||
| Fibroma’ | 1(1.4) | |||||||
| Unremarkable tissue | 1(1.4) | |||||||
| Dysplastic Squamous Tissue | 1(1.4) | |||||||
| Gynaecomastia | 1(1.4) | 1(1.4) | ||||||
| Total | 15 (21.1) | 22(31.0) | 17 (23.9) | 8 (11.3) | 5 (7.0) | 3 (4.2) | 1 (1.4) |
Table 3: Chi-square test of association between Pattern of breast lesions and Age group in the studied population.
| Pattern of Breast Lesions | Right | Left | Unspecified Side | Chi-square |
|---|---|---|---|---|
| Inflammatory Chronic Mastitis | 1 (1.4) | |||
| Inflammatory Periductal Mastitis | 2 (2.8) | |||
| Inflammatory Fat Necrosis | 2 (2.8) | 1 (1.4) | ||
| Inflammatory Granulomatous mastitis | 1 (1.4) | |||
| Inflammatory Intralobular Mastitis | 1 (1.4) | |||
| Proliferative Fibrocystic Change | 5 (7.0) | 5 (7.0) | 0.364 | |
| Proliferative Ductal Hyperplasia | 1 (1.4) | |||
| Proliferative Duct Ectasia | 1 (1.4) | |||
| Neoplastic Benign Fibroadenoma | 10 (14.1) | 11 (15.5) | 5 (7.0) | |
| Neoplastic Benign Tubular Adenoma | 2 (2.8) | 1 (1.4) | 1 (1.4) | |
| Neoplastic Malignant Invasive Ductal Carcinoma | 2 (2.8) | 3 (4.2) | 4 (5.6) | |
| Neoplastic Malignant Lobular Carcinoma | 1 (1.4) | |||
| Galactocele | 2 (2.8) | 1 (1.4) | ||
| Pregnancy like Changes | 1 (1.4) | |||
| Degenerative Changes | 1 (1.4) | |||
| Epithelial Cyst | 1 (1.4) | |||
| Fibroma | 1 (1.4) | |||
| Unremarkable tissue | 1 (1.4) | |||
| Dysplastic Squamous Tissue | 1 (1.4) | |||
| Gynaecomastia | 2 (2.8) | |||
| Total | 32 (45.1) | 25 (35.2) | 14 (19.7) |
Table 4: Chi-square test of association between Pattern of breast lesions and laterality in the studied population.
| Type of lesion | Side/Age of Lesion | Total | |||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Right | Left | Unspecified Side | |||||||||||||||||||||
| 11- 20 | 21- 30 | 31- 40 | 41- 50 | 51- 60 | 61- 70 | U | Total | 11- 20 | 21- 30 | 31- 40 | 41- 50 | 51- 60 | 61- 70 | U | Total | 11- 20 | 21- 30 | 31- 40 | 41- 50 | 51- 60 | 61- 70 | ||
| Inflammatory | |||||||||||||||||||||||
| Chronic Mastitis | 1 | 1 | 1 | ||||||||||||||||||||
| Periductal Mastitis | 1 | 1 | 2 | 2 | |||||||||||||||||||
| Fat Necrosis | 1 | 1 | 2 | 1 | 1 | 3 | |||||||||||||||||
| Granulo- matous mastitis | 1 | 1 | 1 | ||||||||||||||||||||
| Intralobular Mastitis | 1 | 1 | 1 | ||||||||||||||||||||
| Proliferative | |||||||||||||||||||||||
| Fibrocystic Change | 3 | 1 | 1 | 5 | 1 | 1 | 2 | 1 | 5 | 10 | |||||||||||||
| Ductal Hyperplasia | 1 | 1 | 1 | ||||||||||||||||||||
| Duct Ectasia | 1 | 1 | 1 | ||||||||||||||||||||
| Neoplastic | |||||||||||||||||||||||
| Benign | |||||||||||||||||||||||
| Fibroa- denoma | 4 | 4 | 1 | 1 | 10 | 3 | 8 | 11 | 2 | 1 | 1 | 1 | 26 | ||||||||||
| Tubular Adenoma | 2 | 2 | 1 | 1 | 1 | 4 | |||||||||||||||||
| Malignant | |||||||||||||||||||||||
| IDC | 1 | 1 | 2 | 1 | 1 | 2 | 1 | 9 | |||||||||||||||
| Lobular Ca | 1 | 1 | 1 | 1 | 3 | 1 | |||||||||||||||||
| Others | |||||||||||||||||||||||
| Galactocele | 1 | 1 | 2 | 1 | 3 | ||||||||||||||||||
| Pregnancy like Changes | 1 | 1 | |||||||||||||||||||||
| Degenerative Changes | 1 | 1 | |||||||||||||||||||||
| Epithelial Cyst | 1 | 1 | 1 | ||||||||||||||||||||
| Fibroma | 1 | 1 | |||||||||||||||||||||
| Un- remarkable tissue | 1 | 1 | 1 | ||||||||||||||||||||
| Dysplastic Squamous Tissue | 1 | ||||||||||||||||||||||
| Gynae- comastia | 1 | 1 | 2 | 1 | |||||||||||||||||||
| Total | 8 | 9 | 7 | 2 | 3 | 1 | 1 | 32 | 3 | 12 | 6 | 3 | 1 | 1 | 26 | 4 | 1 | 5 | 3 | 1 | 71 |
Table 5: Laterality and age of lesions in the studied population.
Discussion
Findings from this study showed that benign breast lesions occurred more frequently than malignant tumors. This is consistent with studies conducted in Zaria, Enugu, Kano, Benin, and Ibadan, Nigeria [4, 5, 6, 7, 8]. Similar studies from other parts of Africa and the world, such as Kenya, Ethiopia, Jamaica, and India, also align with our findings [18, 19, 20, 21]. Among benign lesions, neoplastic benign fibroadenoma was the most prevalent in the studied population, consistent with previous studies [4, 5, 8, 18, 19, 20, 21, 22, 23, 24, 25, 26]. The etiology, epidemiology, and pathophysiology of fibroadenoma could explain its predominance across various populations. Fibroadenomas are described as painless, non-cancerous tumors [27], typically occurring in women of reproductive age and are prone to atrophy after menopause. Therefore, they are less commonly observed in post-menopausal women [27]. These tumors arise from stromal, epithelial, and connective tissues, which are functionally important in the breast. They contain receptors for estrogen and progesterone, leading to increased proliferation during pregnancy due to the excessive secretion of female reproductive hormones, which further stimulates connective tissue proliferation in the breast [27]. In this study, fibroadenoma was followed by proliferative fibrocystic changes in the studied population. This finding is consistent with Ezike, et al. [25] and Akinapally, et al. [21], who found that fibrocystic changes were the second most common benign breast disease (BBD) observed in Abuja, Nigeria, and Telangana, India, accounting for 29.3% and 21.8% of their studied populations, respectively. However, this differs from the study by Begum, et al. [28], which found that lactating adenoma was the second most common BBD. These differences may result from variations in the genetic makeup of different populations. Neoplastic malignant invasive ductal carcinoma was the most prevalent malignant breast lesion, a finding that aligns with previous studies [4, 8, 12, 21, 26]. Invasive ductal carcinoma is the major type of breast cancer, characterized by the infiltration and malignant proliferation of neoplastic cells within breast tissue [29].
The third decade of life recorded the highest number of lesions in the studied population, a finding that differs from Mayun, et al. study in Gombe, Nigeria [12], where the fourth decade showed predominance. We also found that neoplastic benign fibroadenoma was most common in the second and third decades, which is consistent with Yerakly and Tadele’s study in Ethiopia [19]. It has been documented that fibroadenoma typically occurs in women between 14 and 35 years of age [27]. The fourth decade had proliferative fibrocystic changes as the most frequent breast lesion, differing from Yerakly and Tadele [19], who found more cases of this lesion in the third decade. Our study showed no association between breast lesions and age. Neoplastic malignant ductal carcinoma was most prevalent in the fifth and seventh decades, consistent with Bhatnagar, et al. [30], who found ductal carcinoma in women aged 41-50, and Bukhari [31], who noted that this cancer is typically detected in women in their fourth to sixth decades of life. However, this differs from Josephine, et al. [18], who observed this lesion in women aged 20-34. Breast lesions occurred more frequently on the right side than on the left in our studied population, a finding that differs from Yerakly and Tadele’s [19] study of Ethiopian women, where lesions were more common on the left side. We also found no association between breast lesions and laterality in the studied population.
We investigated both bilateral and unilateral breast lesions, observing that neoplastic benign fibroadenoma and tubular adenoma occurred bilaterally in the second decade, while proliferative fibrocystic changes were seen in the fourth to sixth decades. Malignant invasive ductal carcinoma also occurred bilaterally in the fourth and sixth decade. Other breast lesions occurred unilaterally across different age groups. Additionally, no association was found between age and breast lesions in the studied population.
Conclusion
Benign breast lesions were more prevalent than malignant ones in the studied population. A peak in the second and third decades was observed for neoplastic benign fibroadenoma, while neoplastic malignant invasive carcinoma was more common in the fourth decade. There was no association between breast lesions, age, and laterality.
References
-
Weidner N, Cote RJ, Suster S, Weiss LW (2009) Modern surgical pathology. 2nd Ed. Saunders Elsevier, Philadelphia.
-
Goldblum JR, Lamps LW, Mckenney JK, Myers JL (2018) Rosai and Ackerman’s surgical pathology. 11th(Edn.), Elsevier, Cambridge University, England, pp: 2306.
-
Kumar VR, Abbas AK, Aster JC (2025) Robbins & Cotran pathologic basis of disease. 9th(Edn.), Elsevier, pp: 1408.
-
Yusufu LMD, Odigie VI, Mohammed A (2003) Breast masses in Zaria, Nigeria. Ann Afr Med 2: 13-16.
-
Anyikam A, Nzegwu MA, Ozumba BC, Okoye I, Olusina DB (2008) Benign breast lesions in Eastern Nigeria. Saudi Med J 29: 241-244.
-
Ochicha O, Edino ST, Mohammed AZ, Amin SN (2002) Benign breast lesions in Kano. Nig J Surg Res 4: 1-5.
-
Otu AA (1990) Benign breast tumors in an African population. J R Col Surg Edin 35: 373-375.
-
Irabor DO, Okolo CA (2008) An audit of 149 consecutive breast biopsies in Ibadan, Nigeria. Pak J Med Sci 24: 257- 262.
-
Tavassoli FA, Devilee P (2003) World Health Organization histological classification of tumours of the breast in pathology and genetics of tumours of the breast and female genital organs. IARC, France.
-
Richard JS, Robert M (2005) Benign Breast Disorders. N Engl J Med 353: 275-285.
-
Rohan TE, Miller AB (1999) Hormone replacement therapy and risk of benign proliferative epithelial disorders of the breast. Eur J Cancer Prev 8: 123-130.
-
Mayun AA, Pindiga UH, Babayo UD (2008) Pattern of histopathological diagnosis of breast lesions in Gombe, Nigeria. Nigerian Journal of Medicine 17(2): 159-162.
-
Hoogerbrugge N, Bult P, Widt-Levert LMD, et al. (2003) High prevalence of premalignant lesions in prophylactically removed breasts from women at hereditary risk for breast cancer. J Clin Oncol 21: 41-45.
-
O’Connell P, Pekkel V, Fuqua SAW, Osborne CK, Clark GM, et al. (1998) Analysis of loss of heterozygosity in 399 premalignant breast lesions at 15 genetic loci. J Natl Cancer Inst 90: 697-703.
-
Tarek TA, Abdul RS, Rajan C (2009) Histopathological Patterns of Female Breast Lesions at a Secondary Level Care Centre in Saudi Arabia. Asian Pacific Journal of Cancer Prevention 10: 1011-1016.
-
Arpino G, Laucirica R, Elledge RM (2005) Premalignant and in situ breast disease: biology and clinical implications. Ann Intern Med 143: 446-457.
-
Dupont WD, Page DL (1987) Breast cancer risk associated with proliferative disease, age at first birth and family history of breast cancer. Am J Epidemiol 125(5): 769- 778.
-
Josephine NR, Lucy M, Marshal M, Elijah S, Emily R (2023) Cytomorphological patterns of breast lesions among women with palpable breast lumps attending select teaching and referral hospitals in Kenya: a descriptive cross-sectional study. Pan African Medical Journal 44(171): 1-10.
-
Yerakly F, Tadele AK (2022) Histopathologic Patterns of Breast Lesions in Hawassa University Comprehensive Specialized Hospital, Sidama Region, Ethiopia: A Six-Year Retrospective Study. Clin Oncol 7: 1895.
-
Shirley SE, Mitchell DI, Soares DP, James M, Escoffery CT, et al. (2008) Clinicopathologic features of breast disease in Jamaica: findings of the Jamaican Breast Disease Study, 2000-2002. West Indian Med J 57(2): 90-94.
-
Akinapally M, Mohd IA, Swathi S, Rajarikam NC (2023) Spectrum of histopathological patterns of breast lesions in a tertiary care hospital. Asian J of Med Sci 14(2): 151- 156.
-
Alamri, A, Alsareii, S, Al-Wadei H, Al-Qahtani A, Sultan S, et al. (2020) Epidemiological Pattern of Breast Diseases among Females in the South-Western Region, Saudi Arabia. Int J of Clinical Med 11: 257-269.
-
Chandanwale SS, Gupta K, Dharwadkar AA, Pal S, Buch AC, et al. (2014) Pattern of palpable breast lesions on fine needle aspiration: A retrospective analysis of 902 cases. J Midlife Health 5(4): 186-191.
-
Olu-Eddo AN, Ugiagbe EE (2011) Benign breast lesions in an African population: A 25-year histopathological review of 1864 cases. Niger Med J 52(4): 211-216.
-
Ezike KN, Raphael S, Okwudire-Ejeh IA, Okonkwo DI (2020) Breast lesions in a district hospital: Demographic and histopathologic characteristics. Ann Trop Pathol 11(2): 113-118.
-
Nwafor CC, Keshinro SO (2015) The pathology of breast biopsies in a sample of Nigerian Patients: Review and analysis. Annals of African surgery 12(2): 89-94.
-
Ajmal M, Khan M, Fossen KV (2023) Breast Fibroadenoma. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing.
-
Begum Z, Tengli MB, Mahantappa S, Farheen, Lateef A (2017) Histomorphological study of various patterns in breast lesions, including carcinoma breast. Indian J Pathol Oncol 4(2): 301-307.
-
Wendie B, Jessica L (2019) Diagnostic Imaging: Breast. 3rd(Edn.), Google Books.
-
Bhatnagar R, Kaushik A (2019) Cytomorphological Spectrum of Breast Lesion in Kumaon Region. JMSCR 7(4): 865-869.
-
Bukhari MH, Arshad M, Jamal S, Niazi S, Bashir S, et al. (2011) Use of fine-needle aspiration in the evaluation of breast lumps. Patholog Res Int, Wiley.
- Morphometric Analysis of the Human Femur: Exploring Platymetric and Robusticity Indices Among the Nigerian Population
- Anatomical Variation of Arteria Lusoria: Clinical Implications for Dysphagia Lusoria and Surgical Risk
- Morphometric Study of the Vertebral Body and Pedicle of Typical Cervical Vertebrae Using Radiological Image
- Epigenetic Mechanisms Driving Human Evolutionary Changes
- Neuroprotective Effects of Ginkgo Biloba Extract on Bilateral Common Carotid Artery Ischaemic Stroke Induced in Wistar Rat
- Communicating Neuroanatomical Fibers in Health and Diseases