Variations in the Drainage Pattern of Testicular and Renal Veins, and Bilateral Duplication of Renal Arteries with Prehilar Divisions
The dissection of a 76-year-old male donor with a consent for research and publication, revealed variations of the renal and testicular vasculature where the right testicular vein joined a right accessory renal vein to form a common trunk that opened into the right renal vein. The left renal vein descended obliquely to the left ventral to the pair of left renal arteries, under crossed the prehilar branches of the arteries dorsally as it approaches the left kidney and entered the hilum posterior to the arterial branches. Both kidneys were supplied by two renal arteries (superior and inferior). The left superior renal artery followed the course of the left renal vein, crossed inferiorly ventral to the inferior renal artery, and then the last part of the left renal vein to enter the lower corner of the hilum of the left kidney. The bilaterally duplicated renal arteries broke up into anterior and posterior prehilar (early) divisions that entered the respective kidney. The co-occurrence of such multiple and complex a variation is of nephron-urological importance and can complicate nephro-surgeries, interventional radiologic procedures and the management of abdominal aortic aneurysm.
Introduction
The renal arteries carry about 20% of the cardiac output to the kidneys [1], some of which also goes to the suprarenal glands, renal pelvis and upper ureter. Near the hilum of each kidney the renal artery, renal vein and the renal pelvis are arranged from ventral to dorsal as vein-artery-pelvis; collectively forming the renal pedicle [2]. The renal arteries are known to be end arteries and their damage, obstruction or accidental ligation can cause renal ischemia and infarction. Each of the renal arteries enters the respective kidney through the hilum and divides into 5 segmental branches [3].
The veins also confluence to form the right and left renal veins that exit through the renal hilum and drain into the inferior vena cava. Despite this long-known description of renal vasculature, their extensive variability in origin, number, and course and division pattern is widely documented [4, 5, 6, 7]. As related to number, there are many case reports that noted frequent encounters of unilateral and bilateral renal artery duplications [8, 9] and the presence of accessory renal [10, 11, 12].
Though the renal veins drain venous blood from each kidney into the inferior vena cava, the left renal vein additionally drains the left suprarenal gland and the gonads (testis or ovary) via the left suprarenal and left gonadal (Testicular or ovarian) veins [13]. Alike the arteries, the testicular veins that drain the testis and epididymis, and renal veins that drain the kidneys, also show a wide range of variation, which occurs as variation in number, course, communication and termination pattern. There are many previous publications that described frequent variations in the drainage pattern of the right testicular vein that included its termination in the right renal vein or into the right accessory renal vein instead of draining into the inferior vena cava [14, 15, 16, 17]. Such variations of the testicular veins are believed to be potential risk factors for varicocele, which is frequently associated with male subfertility or infertility [18]. Similarly, variations of the renal veins also occur as differences in numbers, course and formation pattern. These include tripling of the right renal veins [19], presence of accessory (double) renal vein [20, 21] and retroaortic course of the left renal vein [22, 23]. These variations, particularly the retroaortic renal vein, can present with various clinical signs and symptoms [23, 24] and can be a cause of unintended injury to the vein during surgical procedures in the lumbar region [24].
It is well accepted that variations of the testicular and renal vasculature are of huge practical importance and the awareness about such variations is of tremendous benefit to the patient and the satisfaction of the Doctor as well. Therefore, this current case report presents a 76-year- old male donor with a variation of the drainage of the right testicular vein together with unilateral and bilateral variations of renal vasculature which are relevant to clinical practice.
Material and Methods
The dissection of the retroperitoneal space of a 76-year- old male donor, who consented for research and publication, incidentally revealed multiple variations including the right testicular vein and renal vasculature of both sides (Figures 1 & 2). The variant vessels were carefully dissected, cleaned and the veins and arteries were painted blue and red respectively for identification and photographs were taken for illustrations (Figures 1 & 2). The pairs of renal arteries on each side were designated and labelled as superior and inferior renal arteries for descriptive purpose (Figure 2), and other structures relevant to this report were also labelled (Figures 1 & 2).
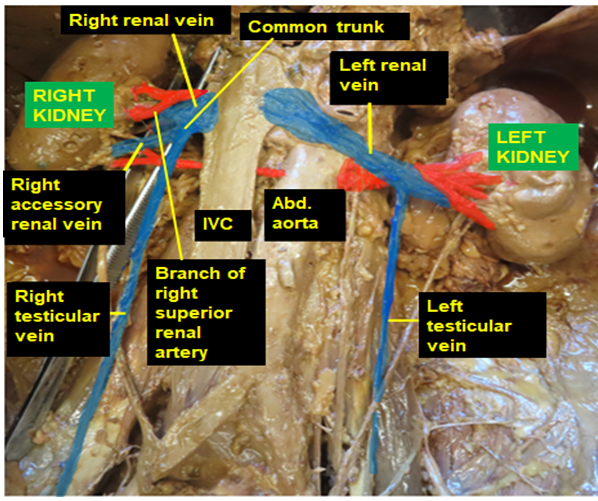
Figure 1: A photographic illustration of the retroperitoneal cavity showing the right testicular vein joining the right accessory renal vein to form a common trunk that opened into the right renal vein and a branch of the right superior renal artery crossing ventral to the right renal vein to enter the hilum. It also illustrates the left renal vein descending ventral to the left renal arteries and then turning around the arteries to enter the hilum dorsal to the arteries.
Case Report
• During the dissection of the retroperitoneum, the following uncommon variations of the right testicular vein and renal vasculature of both sides were observed.
Testicular and Renal Veins
- The right testicular vein ascended on the ventral surface of the psoas major muscle as usual and then joined a right accessory renal vein of similar caliber that exited the right kidney at the lower corner of the renal hilum to form a short common trunk that opened into the right renal vein (Figure 1).
- The right renal vein received the common trunk formed by the right accessory renal vein and the right testicular vein (Figure 1).
- The left renal vein descended to the left ventral to the renal arteries as usual and then twisted around the prehilar divisions of left renal arteries to enter the hilum of the left kidney dorsal to the renal artery branches (Figure 1).
Renal Arteries
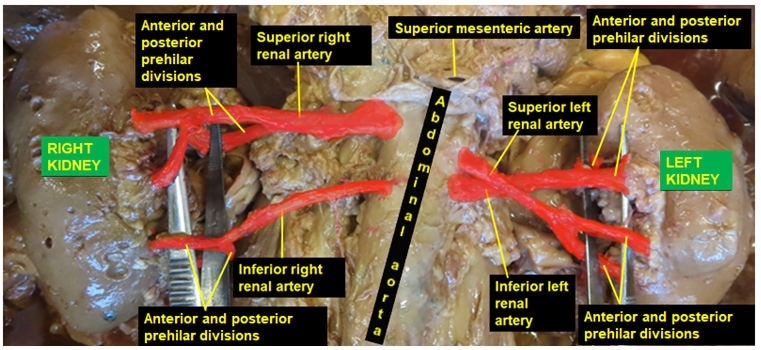
Bilateral pairs of renal arteries (superior and inferior) were found to arise from the abdominal aorta just inferior to the origin of the superior mesenteric artery (Figure 2). Both right and left pairs of renal arteries were hilar (entered the kidney through hilum) but with anterior and posterior prehilar (early) divisions (Figure 2).
- Right pair of renal arteries: on the right side a larger superior renal artery arose from the abdominal aorta at a higher level (at about the level of L1 - L2) than the other three renal arteries, while a much smaller right inferior renal artery, which can be considered as accessory renal artery, arose at the level of L2 (Figure 2). These two right renal arteries ran to the right dorsal to the inferior vena cava and the right renal vein, and divided into anterior and posterior prehilar divisions that entered the right kidney near the inferior and superior corners of the renal hilum (Figure 2). One of the branches of the anterior division of the right superior renal artery crossed inferiorly ventral to the right renal vein and entered the hilum (Figure 1).
- Left pair of renal arteries: the two left renal arteries (also superior and inferior), with a relatively equal size, originated from the left side of the abdominal aorta very close to one another (Figure 2). The left superior renal artery originated at a level half-way between the right superior and inferior renal arteries, while the left inferior renal arteries arose at the same level with the right inferior renal artery (Figure 2). Then, the left superior renal artery crossed ventral to the left inferior renal artery. At first it descended between the renal vein and the left inferior renal artery following the course of the left renal vein, then crossed inferiorly ventral to the left renal vein as it approaches the left renal hilum and divided into anterior and posterior prehilar divisions that entered the inferior corner of the hilum of the left kidney (Figures 1 & 2). The left inferior renal artery ascended slightly to the left by undercrossing the left superior renal artery and similarly divided into anterior and posterior prehilar division that entered the superior corner of the hilum (Figure 2).
Discussion
Previous publications have generally shown that in 70% of individuals a single renal artery supplies each kidney and this artery can show variable division patterns before entering the renal hilum (prehilar divisions) [1]. Classically, the renal vasculature and the renal pelvis form a surgically important bundle, the renal pedicle, in which these structures are arranged from ventral to dorsal as vein, artery and renal pelvis. But the study conducted by Trivedi, et al. [2] on 100 cadaveric kidneys, showed that this arrangement near the renal hilum is greatly variable. According to these authors, the classic arrangement (vein-artery-pelvis) was seen only in 27 kidneys, while in 23 kidneys the anterior division of the renal artery is the most ventral structure, in 42 kidneys the posterior division of the renal artery is the most dorsal, and in 5 kidneys the anterior and posterior divisions of the renal arteries were the most ventral and dorsal structures respectively. In the present case all the prehilar divisions of the left renal artery were the most ventral on the left side while the anterior prehilar division of the right superior renal artery is the most ventral on the right side. According to Moinuddin Z, et al. [3], in the majority of the case, the renal arteries divide into five branches near the renal hilum. These branches further divide into anterior and posterior segmental arteries that do not freely anastomose with each other leaving Brodel’s bloodless (avascular plane of Brodel) between them on the posterolateral aspect of each kidney (a very important plane in nephro-surgery. Moreover, the renal arteries vary not only in their division pattern but also in their origin, number, and course. A study on CT-angiogram of 100 living kidney donors found variations in renal artery configuration in 50% of the cases [4], while another study on 400 patients that underwent abdominal CT examination showed only 32.25% had renal arterial variation [5]. A higher prevalence of different renal arterial variations up to 75% was also reported by Garcia-Barrios A, et al. [6]. Sirikonda, et al. [7], in their study done on 100 kidneys of 50 formalin fixed cadavers, found 4 early divisions, 4 double renal arteries and 1 cases of accessory renal artery, which were either right or left unilateral and concluded that the three commonly observed variations are double renal arteries, early divisions and the presence of accessory renal artery. There are also case reports that relate to unilateral and bilateral renal artery duplications. Tessema [8] reported two cases of renal artery duplications with prehilar divisions in male and female donors. In the male donor a left unilateral duplication of the renal artery where the most superior and smaller of the two was considered as accessory and polar left renal artery and the inferior and larger one with prehilar division was considered as the main renal artery. In the female donor bilaterally, duplicated renal arteries of comparable caliber that had prehilar divisions were reported as superior and inferior renal arteries. Bilateral renal artery duplication with prehilar divisions in a male donor with complete aberrance of the major visceral branches of the abdominal aorta was also document [9]. According to this report, the right inferior (accessory) renal artery was pre-caval and crossed to the right dorsal to the right testicular vein, while on the left side a smaller left superior renal artery that arose by a common trunk with the larger left inferior renal artery, crossed inferiorly ventral to the left inferior renal artery, similar to the current case report, to enter the inferior corner of the left renal hilum but showed no prehilar divisions. Despite the bilateral duplication and the similarity in the course of the left superior renal artery, the present report is deferent in that the two right renal arteries were retrocaval and the left renal arteries have separate origins from the abdominal aorta. According to a study conducted on 240 kidneys from 120 kidney donors, renal vascular variation is found in 59 of them, which were significantly more common in males [10]. The most frequently observed arterial variation was accessory renal artery [10, 11]. The higher prevalence of accessory renal artery was also affirmed by the study of Mohammad S, et al. [12]. A unilateral doubling, tripling and quadrupling of renal veins as well as double and triple renal arteries in cadavers were also well documented [13].
Regarding the right testicular veins, the most common variation is its drainage into the right renal vein rather than the inferior vena cave. Gopal K, et al. [14] in their study of 25 cadavers found four variations in the drainage of the right testicular veins: one drained at the junction of the accessory renal vein and inferior vena cava, two drained into the right renal vein and one into the left renal vein. Bilateral variations of the testicular veins with the right one opening into the right renal vein and double left testicular veins both of which opened into the left renal vein was also reported by Ogut E, et al. [15]. In another report a right testicular vein draining into a right accessory renal vein by arching over a right accessory renal artery was also documented [16]. Other study noted a tripling of the right testicular veins (medial, middle and lateral) with the medial testicular vein draining into the right renal vein [17]. However, the observation in the present case differs from those previously published data in that the right testicular vein and right accessory renal veins of comparable size joined together to form a common stem that drained in the right renal vein. Regardless of the number course or drainage pattern, such variations may play a role in the pathogenesis and pathophysiology of male fertility disorders [18]. The variability of renal veins in number, course and branching pattern were also well recognized. Those variation include unilateral tripling [19], accessory renal vein [20, 21] and retroaortic course [22, 23]. These variations particularly the retroaortic renal vein can present with flank pain, hematuria, thrombosis, varicocele and pelvic congestion due to nutcracker syndrome and can also result in renal congestion, renal infarction and bacterial colonization and renal abscess formation [23, 24]. Such a retroaortic renal vein is also vulnerable to injury during orthopedic and surgical procedures in the lumbar region including malignant lumbar lymph node removal [24].
Even though there is a wide range of testicular and renovascular variation, the present case is different from all previous publications for the following reasons:
- The right testicular and accessory renal veins formed a common trunk that joined the right renal vein
- The left renal vein descended ventral to the two left renal arteries at first and, close to the left renal hilum, it turned around the renal arteries inferiorly and dorsally to enter the renal hilum posterior to the arteries.
- The renal arteries are bilaterally duplicated with right superior renal artery having the highest origin from the abdominal aorta and one of its prehilar branches crossed ventral to the right renal vein.
- The left superior and inferior renal arteries originated close to one another but separately from the abdominal aorta, intercrossed before dividing into their anterior and posterior prehilar divisions. The divisions entered the corners of the renal hilum opposite to their origin from the abdominal aorta Therefore, the authors of this case report believe that the various and unique twists and crossovers of the renal vessels, can possibly impact free arterial blood flow and venous return, which could probably be associated with renal ischemia and congestion. On the other hand, the presence of double renal arteries can have an advantage, i.e., since the individual renal arteries are considered to be end arteries, the presence of more than one artery, can theoretically be protective of renal ischemia and infarction in case one of the arteries is occluded or damaged.
Conclusion
The co-occurrence of such multiple and complex variations is of nephron-urological importance and can lead to misinterpretation of radiological images, misdiagnosis of associated diseases and can complicate nephro-urologic surgeries including renal transplantation surgery and live kidney donation procedures, interventional radiologic procedures and the management of abdominal aortic aneurysm. Therefore, by considering the advantages and disadvantages of having duplicated renal arteries in particular, a careful pre-procedural evaluation of renal vasculature would be important to avoid unintended consequences which are of tremendous benefit to the patient and the professional satisfaction of the Doctor as well.
Acknowledgment
We are thankful to the donor and his families for their invaluable donation and consent for education, research and publication. We would also like to express our gratitude to the department of biomedical sciences for the encouragement and uninterrupted support. Similarly, we are also grateful to Denelle Kees and John Opland for their immense assistance during the dissection of this cadaver in the gross anatomy lab.
References
-
Doni Rpk, Janaki CS, Vijayaraghavan V, Kothandaraman U, Teli C, et al. (2013) Bilateral variations of renal vasculature: A case report. Int J Res Health Sci 2(3): 678- 681.
-
Trivedi S, Athavale S, Kotgiriwar S (2011) Normal and variant anatomy of renal hilar structures and their clinical significance. Int J Morphol 29(4): 1379-1383.
-
Moinuddin Z, Dhanda R (2015) Anatomy of the kidney and ureter. Anaesthesia and intensive care medicine 16(6): 247-252.
-
Aremu A, Igbokwe M, Olatise O, Lawal A, Maduadi K (2021) Anatomical variations of the renal artery: A computerized tomographic angiogram study in living kidney donors at Nigerian Kidney transplant center. Afri Health Sci 21(3): 1155-1162.
-
Chhetri PK, Basnet P, Adhikari A (2021) Anatomical variation of renal artery in patients undergoing computerized tomography of abdomen: A hospital- based cross-sectional study. J Lumbini Med Coll 9(2).
-
Garcia-Barrios A, Cisneros-Gimeno AI, Celma-Pitarch A, whyte-Orozco J (2023) Anatomical study about the variations in renal vasculature. Fol Morphol.
-
Sirikonda P, Mariya, Sugavasi R, Katikireddi RS (2023) Variations in renal arteries- A cadaveric study in Telangana, India. Int J Anat Radiol Surg 12(3): AO01- AO04.
-
Tessema CB (2022) Duplication of renal arteries with unusual extra renal division patterns and positional relationship to hilar structures. Int J Anat Var 15(4): 166-168.
-
Tessema CB (2022) Complete aberrance of all major visceral branches of the abdominal aorta. Int J Anat Var 15(10): 225-228.
-
Gebremeskal A, Afework M, Wondmagegn H, Bekele M (2021) Renal vascular variation among kidney donors presented at national kidney transplantation center, Addis Ababa, Ethiopia. Translational Research in Anatomy 25: 100145.
-
Hekimoglu A, Ergun O (2022) Evaluation of renal vascular variations with computed tomography. African Journal of Urology 28: 21.
-
Mohammed S, Elhag A, El-Mardi A (2022) Evaluation of renal artery anatomical variations using multi-detector computerized tomographic scan in Sudan. Open Journal of Radiology 12(4): 229-238.
-
Hassan SS, El-Shaarawy EA, Johnson JC, Youakim MF, Ettarh R (2017) Incidence of variation in human cadaveric renal vessels. Folia Morphol 76(3): 394-407.
-
Gopal K, Sing O, Anurag (2017) Abnormal pattern of renal and Gonadal veins and their developmental correlations. Int J Anat Res 5(3.2): 4295-4298.
-
Ogut E, Baut C (2022) Anatomic variation type III right testicular venous drainage: a case report. Basic Clin Health Sci 6(1): 314-317.
-
Singh R, Jaiswal A, Shamal SN, Sing SP (2011) Variation in the origin of the testicular arteries and drainage of right testicular vein. Int J Morphol 29(2): 614-616.
-
Nayak SB, Vasudeva SK (2020) Triple right testicular veins and their variant termination and communications. Heliyon 6(9): e05014.
-
Tessema CB (2022) Three unusual variations of the testicular vasculature in a single cadaver: case report and short review of pathophysiologic correlations with varicocele. Int J Anat Var 15(6): 182 -184.
-
Fernandes RMP, Conte FHP, Favorito LA, Abidu- Figueiredo M, Babinski MA (2005) Triple right renal vein: An uncommon variation. Int J Morphol 23(3): 231- 233.
-
Karadeniz AG, Korkmaz HAA, Cavusoglu IG (2019) A very rare renal venous anomaly: Accessory polar left renal vein. Turk J Thorac Cardiovasc Surg 27(2): 241-244.
-
Hostiuc S, Rusu MC, Negoi I, Dorobantu B, Grigoriu M (2019) Anatomic variants of renal vein: A meta-analysis of prevalence. Scientific reports 9: 10802.
-
Sabouri S, Hosseini A, Shivaei SS (2015) Retro-aortic inverted left renal vein: A rare anomaly found in a renal donor. Iran J Radiol 12(2): e113774.
-
Rampersad F, Chan A, Diljohan J (2019) Retroaortic left renal vein draining into common iliac vein: a rare variant and its clinical implication. BMJ Case Rep 12(5): e230004.
-
Anjamrooz SH, Azari H, Abedinzaseh M (2012) Abnormal pattern of renal veins. Anat Cell Biol 45(1): 57-61.
- Pattern of Breast Lesions in Ovu Inland, Delta State, South Southern Nigeria
- Morphometric Analysis of the Human Femur: Exploring Platymetric and Robusticity Indices Among the Nigerian Population
- Anatomical Variation of Arteria Lusoria: Clinical Implications for Dysphagia Lusoria and Surgical Risk
- Morphometric Study of the Vertebral Body and Pedicle of Typical Cervical Vertebrae Using Radiological Image
- Epigenetic Mechanisms Driving Human Evolutionary Changes
- Neuroprotective Effects of Ginkgo Biloba Extract on Bilateral Common Carotid Artery Ischaemic Stroke Induced in Wistar Rat