Sub-Acute Interstitial Pneumonia - First Clinical Indicator of Underlying Immune Compromise Due to HIV Infection
Background: The significant number of late presenters of human immunodeficiency virus (HIV) infection remains a serious public health problem. Late presenters [CD4 cell count below 350 cells/ mm3 or with an acquired immune deficiency syndrome (AIDS)-defining event regardless of the CD4 cell count] are associated with a significant risk not only for AIDSdefining conditions but also for non AIDS-defining diseases which aggravate the prognosis of patients. Lymphoid interstitial pneumonitis (LIP) is one of these conditions described more often after the onset of HIV epidemic. LIP is a benign polyclonal lymphoproliferative disorder of the lung with not well characterized clinical and radiographic findings. Case presentation: We report the uncommon case of LIP as an initial presentation of HIV. The findings of computed tomography indicated the diagnosis of HIV-associated LIP, although this condition is mainly described in a normal range of CD4 cell count. Conclusion: It is important to recognize HIV as one of the risk factors for LIP with antiretroviral therapy resulting in rapid improvement of HIV-associated LIP. This case presentation highlights the importance of timely diagnosis and initiation of antiretroviral therapy. The increase of CD4 cell count and viral suppression may improve the symptoms of LIP.
Introduction
Lymphoid interstitial pneumonia (LIP) is a rare benign polyclonal lymphoproliferative disorder of the lung parenchyma due to infiltration of the interstitium and alveolar spaces by lymphocytes, plasma cells, and other lymphoreticular elements [1]. It was originally described by LIEBOW and CARRINGTON [2]. It is seen more commonly among HIV infected patients, especially in black African and Afro-Caribbean [3]. The occurrence of pulmonary abnormalities is not unusual in patients with acquired immunodeficiency syndrome (AIDS). The causes could not only be infectious diseases and malignancies but rather, there are a number of non-infectious and non-malignant disorders which are clinically and radiographically similar [4]. In HIV- associated LIP a possible mechanism is the HIV induced proliferation of bronchus-associated lymphoid tissue (BALT) [5]. Additionally, LIP is associated with autoimmune disorders such as Sjogren’s syndrome, systemic lupus erythematosus (SLE), Hashimoto’s disease and autoimmune haemolytic anaemia [6, 7]. However, the aetiology of LIP
remains unknown. The clinical and radiographic features are not well characterized. Thus, the differential diagnosis from infectious diseases such as pneumocystis jiroveci pneumonia could be difficult. High resolution computed tomography and transbronchial biopsy are basic tools for diagnosis [1].
Case Presentation
A fifty five year-old male presented with progressive cough and dyspnea for a month. He had been treated one month prior with levofloxacin when a chest x-ray revealed bilateral lower lobe infiltrates. Social history noted former tobacco abuse (20 pack years) and no illicit drug use. He denied having any environmental, social or occupational risk factors for HIV. On examination, he was afebrile, tachypneic (22 breaths/min), tachycardic (102 beats/min), hypoxic (85% on room air), clubbing was seen and chest examination revealing bilateral basilar rales. Laboratory values revealed a white cell count of 5.64×109/L with a normal differential. Thoracic computed tomography showed diffuse bilateral ground glass opacities (Figures 1 & 2) with septal thickening and non-specific ill-defined nodules. The patient was placed on oxygen therapy, started on empiric antibiotic therapy and bronchodilators. Bronchoscopy with bronchoalveolar lavage was performed. Bacterial, fungal, viral, and mycobacterial cultures were negative, Cytological analysis revealed no evidence of pneumocystis or malignancy. Histopathologic examination showed lymphocytic infiltration of the bronchial wall and the interstitium suggestive of LIP. HIV antibody testing returned positive with a CD4 count of 127cells/ μL. Patient was started on antiretroviral therapy (300mg Tenofovir, 300mg Lamivudine and 100mg Dolutegravir) along with corticosteroids (prednisone 0.5 mg/kg) leading to rapid improvement in symptoms and discharged the patient in a stable condition.
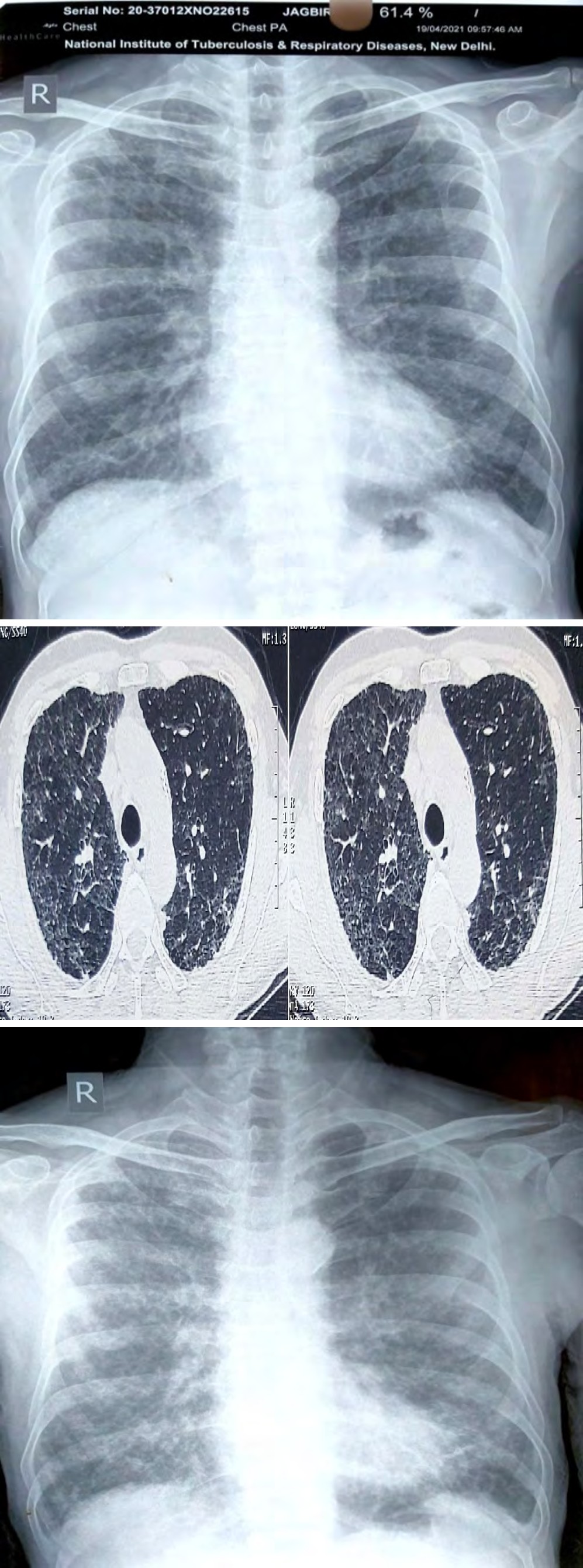
Figure 1a: Chest radiograph showing extensive bilateral interstitial infiltrates on admission.
Figure1b: Chest readiograph showing improvement after 8 weeks of treatment.
Discussion
Lymphocytic interstitial pneumonitis may be an uncommon condition, but the increased frequency in HIV infected patients indicates the need to take this diagnosis into consideration. The prevalence is higher in HIV infected young women, particularly of African race [8, 9]. Recognizing potential presentations of patients with HIV, as evidenced by this case, can prove to be quite challenging especially early on in the course. HIV-associated LIP is relatively uncommon, occurring in less than 5% of adult necropsy case series [10, 11]. The most common symptoms of LIP include progressive exertional dyspnea of several weeks duration and nonproductive cough. Patients may also present commonly with fever, weight loss, and fatigue [10]. Clubbing is commonly seen in the pediatric population [12] and has been described sporadically in the adult population, even in the absence of bronchiectasis [13]. A mean time from initial presentation to diagnosis can exceed 15 months [14].
The natural history of LIP is not well known, causing difficulties in the treatment. The therapeutic approach is even more difficult in HIV infected patients. Glucocorticoids have been used in various doses and duration in the past. According to the describing results improvement was seen in some cases but in a number of them the withdrawal or dose reduction led to aggravation [6, 15]. The response with antiretroviral therapy is significant probably due to viral suppression and increase of CD4 cell count [16]. Clinical and radiological improvement has been documented only using ART, although some have been improved without ART [16]. Clinical and radiological improvement has been estimated 3.5 and 6-8 months after beginning ART respectively [17].
Based on the patient’s living conditions reported at that time, his occupational exposure, history of smoking, and the clinical similarities between his presentation and other common causes of dyspnea (especially those linked with his occupational and social risk factors), it was most likely considered that the patient had a lower respiratory tract infection overlapping an already diseased lung. After fifteen day course in the hospital, the patient was discharged on prednisone, trimethoprim-sulfamethoxazole (after it was determined the patient had a CD4 count of 127 cells/μL) and ART (300mg Tenofovir, 300mg Lamivudine and 100mg Dolutegravir).
HIV-associated LIP should be included in the differential diagnosis of patients presenting with chronic cough and dyspnea who have risk factors for HIV. Implementation of these measures in the future may help physicians diagnosing HIV earlier in its course and lead to decreased patient morbidity through faster recognition and treatment of LIP.
Conclusion
LIP is uncommon in adults with HIV and rarely a presenting feature of HIV. Current treatment recommendations include antiretroviral therapy and or corticosteroids, although the scientific evidence to back these recommendations is sparse. HIV testing should be offered to all patients presenting with a new diagnosis of LIP.
References
-
Van Zyl Smit RN, Naidoo J, Wainwright H, Said-Hartley Q, Davids M, et al. (2015) HIV associated lymphocytic interstitial pneumonia: a clinical, histological and radiographic study from an HIV endemic resource-poor setting. BMC Pulm Med 15: 38.
-
Liebow A, Carrington CB (1969) The interstitial pneumonias. 1st (Edn.), In: Simon M, Potchen EJ, LeMay M (Eds.), Frontiers of Pulmonary Radiology, New York, Grune & Stratton, pp: 102-141.
-
Das S, Miller RF (2003) Lymphocytic interstitial pneumonitis in HIV infected adults. Sex Transm Infect 79(2): 88-93.
-
Conces DJ, Tarver RD (1991) Noninfectious and nonmalignant pulmonary disease in AIDS. J Thorac Imaging 6(4): 53-59.
-
Ho DD, Pomerantz RJ, Kaplan JC (1987) Pathogenesis of infection with human immunodeficiency virus. N Engl J Med 317(5): 278-286.
-
Itescu S, Brancato LJ, Buxbaum J, Gregersen PK, Rizk CC, et al. (1993) A diffuse infiltrative CD8 lymphocytic syndrome in human immunodeficiency virus (HIV) infection: a host immune response associated with HLA- DR 5. Ann Intern Med 112(1): 3-10.
-
Daniel G, Lary Y (2013) Lymphocytic interstitial pneumonia as a manifestation of SLE and secondary Sjogren’s syndrome. BMJ Case Rep 2013: bcr2013009598.
-
Cha SI, Fessler MB, Cool CD, Schwarz MI, Brown KK (2006) Lymphoid interstitial pneumonia: clinical features, associations and prognosis. Eur Respir J 28(2): 364-369.
-
Griffiths MH, Miller RF, Semple SJ (1995) Interstitial pneumonitis in patients infected with the human immunodeficiency virus. Thorax 50(11): 1141-1146.
-
Das S, Miller RF (2003) Lymphocytic interstitial pneumonitis in HIV infected adults. Sexually Transmitted Infections 79(2): 88-93.
-
Marchevsky A, Rosen MJ, Chrystal G, Kleinerman J (1985) Pulmonary complications of the acquired immunodeficiency syndrome: a clinicopathologic study of 70 cases. Human Pathology 16(7): 659-670.
-
Amorosa JK, Miller RW, Laraya Cuasay L, Gaur S, Marone R, et al. (1992) Bronchiectasis in children with lymphocytic interstitial pneumonia and acquired immune deficiency syndrome: plain film and CT observations. Pediatric Radiology 22(8): 603-606.
-
Scarborough M, Lishman S, Shaw P, Fakoya A, Miller RF (2000) Lymphocytic interstitial pneumonitis in an HIVinfected adult: response to antiretroviral therapy. International Journal of STD and AIDS 11(2): 119-122.
-
Koss MN, Hochholzer L, Langloss JM (1987) Lymphoid interstitial pneumonia: clinicopathological and immunopathological findings in 18 cases. Pathology 19(2): 178-185.
-
Lin R, Gruber P, Saunders R, Perla EN (1988) Lymphocytic interstitial pneumonitis in adult HIV infection. N Y State J Med 88(5): 273-276.
-
Innes A, Huang L, Nishimura S (2004) Resolution of lymphocytic interstitial pneumonitis in an HIV infected adult after treatment with HAART. Sex Transm Infect 80(5): 417-418.
-
Dufour V, Wislez M, Bergot E, Mayaud C, Cadranel J (2003) Improvement of symptomatic human immunodeficiency virus-related lymphoid interstitial pneumonia in patients receiving highly active antiretroviral therapy. Clin Infect Dis 36(10): e127-e130.
- Epidemiological and Clinical Aspects of Intestinal Parasitoses Among Students in the City of Bocaranga, Central African Republic
- Artificial Intelligence Empowers Global Infectious Disease Prevention and Control: Opportunities and Challenges
- Factors that Affect the Incidence of Babesia and Blood Donor Testing in Select States: A Regression Analysis
- Neuro-TB: The Battle between Tuberculosis and the Nervous System
- The Biological and Health Implications of Cat Fleas (Ctenocephalides felis): Assessing Zoonotic Risks and Hygiene Strategies
- Biostatistical Analysis of Medicinal Plants for Treating Schizophrenia