Neurosyphilis Presenting as Failure to Thrive
Neurosyphilis occurs when the nervous system is affected by the Treponema Pallidum bacterial species. Medical literature describes two clinical stages: early and late. Early can be asymptomatic or show signs of meningitis and meningoencephalitis. Conversely, late presents as parenchymal, vascular abnormalities, tabes dorsalis or syphilitic gumma. Although neurosyphilis is now uncommon, knowledge of key physical exam findings is crucial to its consideration and subsequent diagnosis and management.
Introduction
Syphilis is caused by a gram-negative spirochete Treponema pallidum [1, 2]. Syphilis is typically characterized by stages of primary, secondary, tertiary and latent [1, 2]. Neurologic symptoms can occur at any stage. Subtypes exhibiting neurologic symptoms include syphilitic meningitis, meningovascular syphilis and parenchymal neurosyphilis [1, 2]. Overall, the incidence of syphilis has been rising since 2000 especially in homosexual men [1, 2]. With the popularization of antibiotics, neurosyphilis is rare and primarily occurs during secondary syphilis in HIV patients with estimated 9.3% risk of symptomatic early neurosyphilis [3]. Risk factors include HIV, high risk sexual behavior, and recreational drug use [1, 2]. There is an annual 3.6% HIV incidence in men with primary or secondary syphilis with the highest cases reported in New York City [4].
Case Presentation
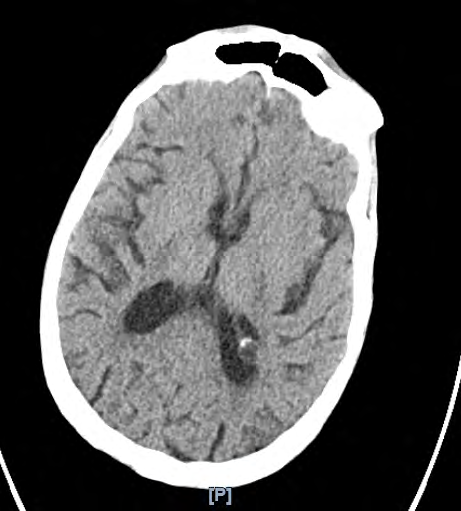
thrive, anorexia, and cachexia. History revealed progressive generalized weakness leading to inability to ambulate, gradual vision loss in one eye and adamant refusal to establish care with a primary medical doctor. He was lethargic with altered mental status. Notable vital signs of temperature of 88.7 and body mass index of 11.2. Physical exam revealed temporal wasting, zygomatic prominence, diffuse muscle atrophy, constricted left pupil with poor vision that was unresponsive to light or accommodation, responsive only to voice, no other gross cranial nerve deficit, generalized bilateral weakness, deep tendon reflexes +2 bilaterally in upper and lower extremities, bladder distention and urinary retention with 580mL. Laboratory findings significant for hypoglycemia, acute kidney injury and pancytopenia. CT imaging of the head on admission was significant for central volume loss (see Figure 1 below). MRI brain showed acute infarctions in the left basal ganglia and left frontal lobe. Lumbar puncture was considered and ultimately deferred due to pancytopenia and high risk of bleeding. This prompted further discussion which divulged an extensive history of high risk sexual behavior with multiple partners of both sexes. Subsequent workup revealed positive HIV with CD4 10, positive RPR and FTA-ABS. Patient was treated with intravenous ceftriaxone for two weeks. Symptoms mildly improved and he was transferred to long-term acute care facility for escalation of care.
Discussion
Neurosyphilis occurs when the nervous system is affected by the Treponema Pallidum bacterial species [5]. Medical literature describes two clinical stages: early and late [5]. Early can be asymptomatic or show signs of meningitis and meningoencephalitis [5]. Conversely, late presents as parenchymal, vascular abnormalities, tabes dorsalis or syphilitic gumma [5]. In 2006, a retrospective study of 81 neurosyphilis cases found 85% presenting with atypical symptoms and that neuropsychiatric symptoms were most common [6]. Consideration of cerebrospinal fluid (CSF) testing is emphasized for diagnosis [7]. VDRL is highly specific [7], whereas FTA-ABS is highly sensitive, ruling out syphilis when there is low suspicion. CSF analysis can yield hypercellularity, hyperproteinorachia [5]. The CDC recommends a variety of penicillin regimens with ceftriaxone used alternatively [7]. Post treatment monitoring is advised with periodic non-treponemal testing and CSF analysis [7]. Although neurosyphilis is now uncommon, knowledge of key physical exam findings is crucial to its consideration and subsequent diagnosis and management [8, 9].
References
-
Liang SY, Reno HEL (2015) Infectious Disease/CDC Update. Update on Emerging Infections: News From the Centers for Disease Control and Prevention. Ann Emerg Med 66(5): 527-528.
-
Cohen SE, Klausner JD, Engelman J, Philip S (2013) Syphilis in the modern era: an update for physicians. Infect Dis Clin North Am 27(4): 705-722.
-
Berger JR, Dean D (2014) Neurosyphilis. Handb Clin Neurol 121: 1461-1472.
-
Pathela P, Braunstein SL, Blank S, Shepard C, Schillinger JA (2015) The High Risk of an HIV Diagnosis Following a Diagnosis of Syphilis: A Population-level Analysis of New York City Men. Clin Infect Dis 61(2): 281-287.
-
Mejdoubi A, Khoulali M, Raouzi N, Nasri S, Mebrouk Y, et al. (2020) Neurosyphilis revealed by compressive cervical spine syphilitic gumma: a case report. Spinal Cord Series and Cases.
-
Mitsonis C, Kararizou E, Dimopoulos N, Triantafyllou N, Kapaki E, et al. (2008) Incidence and clinical presentation of neurosyphilis: A retrospective study of 81 cases. Int J Neurosci 18(9): 1251-1257.
-
Ha T, Tadi P, Dubensky L (2020) Neurosyphilis. StatPearls.
-
Kalichman SC, Pellowski J, Turner C (2011) Prevalence of sexually transmitted co-infections in people living with HIV/AIDS: systematic review with implications for using HIV treatments for prevention. Sex Transm Infect 87(3): 183-190.
-
Solomon MM, Mayer KH, Glidden DV, Liu AY, McMahan VM, et al. (2014) Syphilis predicts HIV incidence among men and transgender women who have sex with men in a preexposure prophylaxis trial. Clin Infect Dis an Off Publ Infect Dis Soc Am 59(7): 1020-1026.
- Epidemiological and Clinical Aspects of Intestinal Parasitoses Among Students in the City of Bocaranga, Central African Republic
- Artificial Intelligence Empowers Global Infectious Disease Prevention and Control: Opportunities and Challenges
- Factors that Affect the Incidence of Babesia and Blood Donor Testing in Select States: A Regression Analysis
- Neuro-TB: The Battle between Tuberculosis and the Nervous System
- The Biological and Health Implications of Cat Fleas (Ctenocephalides felis): Assessing Zoonotic Risks and Hygiene Strategies
- Biostatistical Analysis of Medicinal Plants for Treating Schizophrenia