Covid-19 and Health Care Workers in Burkina Faso: Characteristics and Perceptions of their Management
Background: Health workers, engaged in the front line of the response to this pandemic, have inevitably been exposed to great risks of infection. Thus, in Burkina Faso, as in most countries, health workers have been infected. Objective: To study the characteristics and perceptions of their care management Methods: It was a descriptive cross-sectional study of health workers with COVID-19 from March to August 2020. All health workers with PCR-confirmed COVID-19 who consented to participate in the study were included. Results: Of the 62 health workers identified, the sex ratio was 0.82. The median age was 40.5 years with interquartile ranges of 36 and 52. Doctors (54.8%) and nurses (25.8%) were the most represented and 60% worked in university hospitals. Fiftyone health workers (82.3%) recalled having been infected, 41 (80.4%) of them in the course of their work. Thirty-three agents (53.2%) were hospitalised. Almost all health workers were symptomatic, frequently stigmatised in 61.3% of cases by their neighbors (60.5%) and their colleagues on duty (47.3%). The evolution was favorable for all health workers and psychosocial care was necessary for 22% of them. Conclusion: As health emergencies are becoming more and more frequent, health workers are vulnerable and it is crucial to put in place, all the necessary conditions to enable them to provide care without risk.
Introduction
Starting in China, COVID 19 quickly spread to other countries worldwide. By the end of January 2020, the WHO declared it an International Public Health Emergency. To date, more than two hundred million cases have been recorded worldwide, including about five million deaths. [1]. In Burkina Faso until October 8, 2021 the country’s toll was 14,403 confirmed cases with 195 deaths [2].
In response to this pandemic, health workers are on the front line. This situation inevitably exposes them to great risks of infection by SARS-CoV-2 especially during the exercise of their profession. [3]. Indeed, they are 3.4 times more likely to contract SARS-CoV-19 than people living in the general community [4]. Prolonged time spent with a patient is a risk factor for transmission of the infection [5, 6]. The modes of contamination of health care workers are diverse, among caregivers, during the care of a COVID-19 patient in the health care setting as well as at home; they can also be family and or community based [7, 8, 9]. The protection of health care workers is therefore a key element to be integrated into the management of patients in order to avoid their contamination [10].
According to WHO, COVID-19 has exposed health workers and their families to levels of risk never before seen. It is estimated that they constitute about 14% of COVID-19 cases reported to WHO and in some countries, and this proportion can be as high as 35%. In Europe, cases of COVID-19 in health workers have been described since the beginning of the epidemic [11, 12]. In Africa, infection of health workers represents 5% of positive cases. Burkina Faso has not been left behind [2, 13]; Thus, healthcare workers have been contaminated, and in this study, we would describe their characteristics and their perceptions of the management in the central region, which was the epicentre of this pandemic in our country.
Methods
Type, setting and period of the study
This was a descriptive cross-sectional study of health workers affected by COVID-19 between March 9, 2020 and August 31, 2020 in the Centre region of Burkina Faso. Inclusion criteria: The following were included in our study: -Any health worker who had COVID-19, residing in the Centre region and whose test was confirmed by PCR. -Any health worker who gave consent to participate in the study. -Health workers who had COVID-19 and could not be reached by telephone were not included in this study. Data collection technique and tools: Data were collected from several sources: from the District Health Information Software (DHIS) version 2 platform, from the Ministry of Health , from patient medical records and hospitalisation registers, from mobile team data for health workers cared for at home and using a questionnaire on their perceptions of care, during the interview of the health worker by an investigator.
Collected variables
We used qualitative and quantitative variables. Thus, the following variables were studied: Socio-demographic and professional data: age, sex, professional status, marital status, patient’s origin, place of care, health facility -Data on prevention and response to COVID-19 at the health facility level: triage service, training of agents on COVID-19 and the use of PPE, availability of PPE and hydro-alcoholic solutions. Clinical data: co-morbidities, symptoms leading to diagnosis, general signs and vitals on admission, persistent symptoms or symptoms that appeared after virological cure. -Therapeutic data: treatment received during the illness -Psychological data: stigmatisation, appreciation of care, experience of the disease.
Data processing and analysis The data were entered and processed on a microcomputer using Word and Excel 2016 software and then analyzed with Epi info 7.2.0.1 software in its French version. Quantitative variables were expressed as mean ± standard deviation and qualitative variables were expressed as proportion.
Ethical and deontological aspects For the realisation of our study, we obtained a favourable opinion of the national ethics committee for health science and research by deliberation N°2020-9-214. The anonymity and confidentiality of the information collected were preserved.
Results
Socio-epidemiological characteristics
From March 9 to August 31, 2020, the country recorded 1375 confirmed cases of COVID-19, including 122 health workers. In the central region, there were 1046 confirmed cases of COVID-19, including 81 (8%) health workers. Sixty- two of them (76.5%) accepted to participate in the study.
According to the month, the maximum contamination was in March and April (85.5%) in 40.5% and 45% respectively. The median age was 40.5 years with interquartile ranges of 36 and 52 and the sex ratio was 0.82. Doctors represented 54.8% of the study population, followed by paramedical staff (35.5%), mainly nurses. Among the health workers, 37 (60%) worked in university hospital centre, mainly 2 at the Yalgado Ouédraogo University Hospital (25.60%) and 13 at the Tengandgo University Hospital (15.85%). At the beginning of the pandemic, only one building at the Tengandgo University Hospital was involved in the care.
According to the location of the health workers, 77.5% were working in other departments of the University Hospital and in other department’s health structures in the city. The rest of the health workers were involved in the management of COVID-19, either at the care sites or in the administrative services of the COVID-19 response. The socio-demographic characteristics of the health workers are shown in Table 1.
| Characteristics | Workforce (N=62) | Percentage |
|---|---|---|
| Age group (years) | ||
| Under 30 | 5 | 8,1 |
| 30-40 | 24 | 38,7 |
| 40-50 | 15 | 24,2 |
| 50-60 | 15 | 24,2 |
| More than 60 | 3 | 4,8 |
| Sex | ||
| M | 28 | 45.2 |
| F | 34 | 54.8 |
| Residence | ||
| Ouagadougou | 58 | 93,5 |
| Others | 3 | 6 ;5 |
| Marital status | ||
| Married | 53 | 85 ;5 |
| Single / Widowed | 9 | 14.5 |
| Profession | ||
| physician | 34 | 54,8 |
| Nurse * | 22 | 35,5 |
| Administrative staff ** | 5 | 8,1 |
| Nursing assistant | 1 | 1,6 |
| Health worker exercise site | ||
| University Hospital Centre *** | 37 | 59,6 |
| Medical centre with surgical unit | 10 | 16,1 |
| Medical centre | 7 | 11,4 |
| Health and Social Promotion Centre | 3 | 4,8 |
| Administrative services **** | 5 | 8 ,1 |
| Sites of care for health workers | ||
| Health centre | 33 | 53,2 |
| Princess Sarah Clinic | 18 | 54,5 |
| UHC-T | 14 | 42,5 |
| Pissy Centre | 1 | 3 |
| Home | 29 | 46,8 |
Table 1: Socio-demographic characteristics of health care workers. Nurse* : State nurse (17), Midwife/Maieutician (3), Biomedical
Table 1: Socio-demographic characteristics of health care workers. Nurse* : State nurse (17), Midwife/Maieutician (3), Biomedical Technologist (1) Administrative staff : operations and response center for health emergencies (2 doctor), Armed Forces Health Service (1 doctor) ; Pharmacy (2) University Hospital Centre (UHC)* : UHC-Yalgado Ouedraogo (19), UHC-Tengandgo (13), UHC-Bogodogo (3), UHC-Charles De Gaule (2), Pharmacy (2), Administrative services **** : operations and response center for health emergencies, (2), Armed Forces Health Service (1), Pharmacy (2)
Circumstances of infection of health workers
COVID-19 prevention and response mechanisms at the health facility level: Prior to their infection, health workers reported having received training in the use of personal protective equipment (PPE) in 18.3% of cases, having PPE in their health facilities (48.4%), having hydro-alcoholic solutions (21.4%) and having a patient triage service (24%).
Concept of infection and site of contamination: Fifty-one health workers (82.3%) stated that they had been in contact with a case of COVID-19, 41 of whom (80.4%) had come into contact with the disease in the course of their work and 9.8% of whom had come into contact with it through an infected family member or contamination in the community. Thus, health workers were probably infected in 87.8% of cases during care in health facilities, in 7.4% of cases during staff on the COVID-19 response and in 4.8% of cases during home care of a COVID-19 case. Table 2 presents the circumstances of contamination of health workers Clinical characteristics: Thirty-three health workers (53.2%) were hospitalised and 29 others (46.8%) managed at home. Co-morbidities were frequent in 25 of them (40.3%), the main ones being arterial hypertension, obesity and diabetes in 40%, 28% and 24% of cases respectively. In 98.5% of cases, the health workers were symptomatic and the main signs were asthenia, headache, fever, cough and ageusia in 66.1%, 61.3%, 54.8% and 50% respectively. In 2.5% of the cases, the health workers had consciousness disorders such as obnubilation. After the virological cure, some signs persisted in the health workers, such as asthenia (27%), cough (16.2%) and rhinitis (8.1%). On the other hand, new signs appeared in some of them, such as asthenia (16.2%), chest pain (13.5%), stress (13.5%), headache (10.8%), myalgia/arthralgia (10.8%) and depression (8.1%) were the most frequent. The clinical characteristics of the health workers are presented in Table 3.
Therapeutic management: In 77.4% of cases, the combination of azithromycin and hydroxychloroquine was administered.
Evolution : In the presence of certain signs, a specialised consultation was necessary for 9 health workers (14.5%), most frequently in pneumology (55.5%), and in 22.2% each in cardiology, neurology and pneumology. Two (3.2%) health workers required respiratory assistance and no deaths were noted.
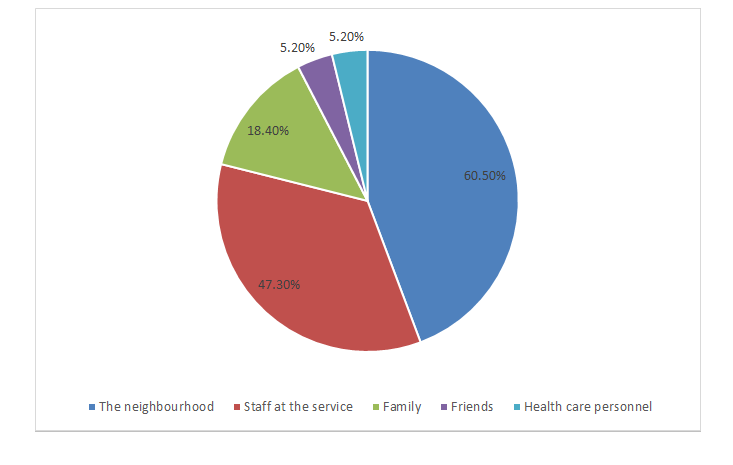
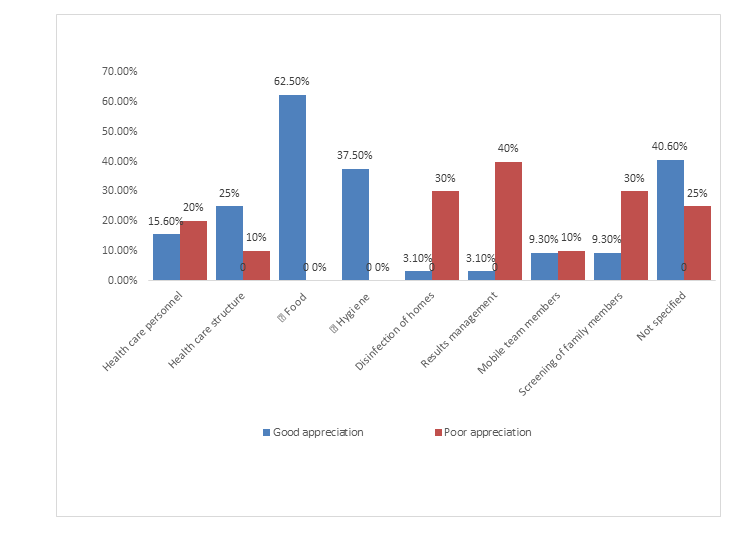
Psychological experience and appreciation of the care : Health workers reported being stigmatized in 61.3% of cases, most frequently by their neighbors (60.5%), their colleagues (47.3%) and their families (18.4%) represented on figure 1. About the quality of care, 51.6% of health workers were satisfied. On the other hand, 32.3% of them were dissatisfied with their management, the main elements of dissatisfaction being communication in the management of their results (40%) and the screening of their family members (30%) as well as the health care personnel in 20% of cases. The assessment of health workers on the quality of their care, is shown in Figure 1on figure 2.
| Information | Work force | Percentage |
|---|---|---|
| Preventive measures | ||
| Training in the use of PPE(n=60) | ||
| Yes | 11 | 18.3 |
| No | 49 | 81,7 |
| Training on COVID-19 (n=58) | ||
| yes | 9 | 14,5 |
| No | 49 | 85,5 |
| Availability of hydroalcoholic solutions (n=57) | ||
| Yes | 30 | 52,6 |
| No | 21 | 36,8 |
| Sometimes | 6 | 10,6 |
| Availability of PPE (n=56) | ||
| Yes | 12 | 21,4 |
| No | 33 | 59 |
| Sometimes | 11 | 19,6 |
| Existence of a triage service (n=54) | ||
| Yes | 13 | 24 |
| No | 41 | 76 |
| Notion of SARS-CoV-2 infection (N=62) | ||
| Yes | 51 | 82.3 |
| Did not remember | 10 | 16.1 |
| No | 1 | 1.6 |
| Contamination site (n=51) | ||
| Working environment | 41 | 80,4% |
| Community | 10 | 16,6% |
Table 2: Preventive measures and contamination framework for health workers
| Symptoms | At diagnosis (N=62) n (%) | Persistent signs (n=37) n (%) | New signs after virological cure (n=37) |
|---|---|---|---|
| Asthenia | 41 (66.1) | 10 (27.0) | 6 (16.2) |
| Headache | 38 (61,3) | 1 (2.7) | 4 (10.8) |
| Fever | 34 (54,8) | 0 | 2 (2.27) |
| Myalgias/Arthralgias | 27 (43,5) | 2 (5.8) | 4 (10.8) |
| Anorexia | 5 (8,0) | 0 | 0 |
| Chills | 4 (6,5) | 0 | 0 |
| Cough | 32 (51,6) | 6 (16.2) | 0 |
| Agueusia | 31 (50) | 2 (5.4) | 1 (2.7) |
| Anosmia | 28 (45,2) | 2 (5.4) | 2(5.4) |
| Sleep disorders | 19 (30,6) | 0 | 0 |
| Digestive disorders | 15 (24,2) | 0 | 2(5.4) |
| Chest pain | 13 (21) | 2 (5.4) | 5 (13.5) |
| Dysphonia | 9 (14,5) | 0 | 0 |
| Dizziness | 6 (9,7) | 1 (2.7) | 1(2.7) |
| Palpitations | 5 (8,1) | 0 | 1 (2.7) |
| Abdominal pain | 3 (4,8) | 0 | 2 (5.4) |
| Odynophagy | 2 (3.2) | 0 | 0 |
| Skin rash * | 2 (3.2) | 0 | 2 (5.4) |
| Rhinorrhea | 30 (48.4) | 3 (8.1) | 2 (5.4) |
| Dyspnea | 6 (9.7) | 0 | 0 |
| Conjunctivitis | 2 (3.2) | 0 | 0 |
| Stress | 0 | 0 | 5 (13.5) |
| Depression | 0 | 0 | 3 (8.1) |
| Neurological disorders** | 0 | 0 | 2 (5.4) |
Table 3: Clinical characteristics. Skin rash * : Pruritus (1), Papule (1) Neurological disorders **: Paresthesia (1), Amnesia (1)
Discussion
The proportion of infected health workers was low (7.8%) over the 6 months of the study, compared to other studies in China (4.4%), the United States (16%) and Spain (20.6%) [14, 15, 7]; however, the study periods were shorter than ours by about one month! At the beginning of the epidemic in our country, screening was done based on clinical suspicion or a notion of contact, which would explain the low frequency observed. During the pandemic period, health workers are considered as contacts. They should benefit from epidemiological surveillance and regular screening tests, which would allow us to have the true prevalence of the infection and prevent the risk of nosocomial transmission to patients and between co-workers. This is how we could guarantee the safety of health workers to ensure the safety of patients [1]. The disease spread rapidly, explaining the high number of patients visiting health centre due to the fear of this new disease during the first months (March and April) of the pandemic in our country. On the other hand, the contamination of health workers could be explained by the non-availability of a triage service at the level of health facilities at the beginning of the epidemic and the inadequacy of the means of prevention of COVID-19 made available to them. In fact, high rates of absence of infection prevention and control measures in their health facilities in terms of (triage service, availability of PPE, hydroalcoholic gel and training in PPE use) were observed by the health workers. In Ouagadougou, the main case management site was a single building at the Tengandogo University Hospital for managing COVID cases. However, most of health workers (85%) came from other health facilities (other university hospitals, medical centre with surgical units, public/private health and social promotion centre). The study also showed that in at least 80% of the cases, the health workers had been in contact with COVID cases, and 80% of the cases, at their workplace. A US study by the CDC Response Team of health workers with COVID-19 found that 55% reported contact at work and 27% in the community [15].
In developed countries, the frequency of contamination at work is reduced due to their highly structured working conditions for the prevention and control of infection and their state of preparedness for the pandemic response. In our context, the non-availability of triage services at the health facility level would explain this high rate of contamination of health workers, as they were in direct contact with suspected cases who came for treatment in their facility. Without prior training on COVID-19 and the availability of personal protective equipment and hydroalcoholic solutions, they were exposed to the virus! The setting up of triage services, the training of agents in PPE use, and the availability of hydroalcoholic gel came much later in the health facilities. Preparation for pandemic response is imperative, but preparation for case management in the health care setting is even more so to ensure not only the safe management of patients but also the safety of staff! This should be continuous training in order to make health workers more efficient in the response because more and more we will be confronted with emerging pandemics. Among the health workers, we noted that there were administrative staffs in 4.8% of the cases; this is probably due to the daily debriefing sessions between the health workers and the other agents of the pandemic response who were non-health workers. This situation reminds us of the importance of promoting teleworking to reduce the risk of contamination of response teams during epidemics. Another type of contamination was found: community contamination; health workers live in community but also in family, in this canal they can be contaminated. Indeed, 16.4% of them declared having been contaminated either by a member of their family or through contact with a close relative. This frequency is doubled in the American study [15]. In addition to the stress of the risk of their contamination, they also have to worry about the risk of transmitting the disease to their family members.
In this study, doctors (54.8%) and nurses (25.8%) were in majority; medical students represented 4.8% of the sample. In France, Greffe et al [11] found proportions of 31%, 24% and 32% respectively among doctors, students and nurses affected by COVID-19. In our context, they are the ones who spend the most time with patients during consultations and care. The orderlies in the transplant study accounted for 17% of infections. This staff in charge of patient hygiene, feeding, and taking medication, did not exist in our work context. Thus, at the sites where COVID-19 cases were managed, patients in isolation were left alone and it was the doctors and nurses who had to carry out these tasks, thus increasing the time of contact with them and the risk of contamination. This caregiver profession would gain to be promoted in our country, in order to take care of hospitalised patients in an efficient way in general, but especially in periods of an epidemic, when the patient is without an attendant and isolated from his family. The proportion of medical students in the Greffe study represented 24% of the cases i.e. about 6 times that found in our study [11]. Some students became infected during their internship outside the sites dedicated to managing of COVID-19 cases. At the beginning of the pandemic at the management sites, there was reluctance on the part of those in charge to involve medical students at the end of their training; subsequently, they were involved, and they committed themselves to treating cases of COVID-19 and worked alongside senior staff with a sign of courage that commands admiration.
The signs found in health workers were the same as those described by other authors on health workers, or in the general population. The evolution was favorable for all the health workers in our study; but this was not same case in the study of Wu in China where he had 5 deaths out of 1668 cases [16].
In 77.4% of the cases, the health workers were treated with Azithromycin associated with hydroxychloroquine, as recommended by the country’s health authorities at the time. The recommendations were that the treatment should be administered and monitored in a hospital, but many health workers were treated at home.
After the virological cure, some signs such as asthenia (27%), cough (16.2%) and rhinitis (8.1%) persisted in 60% of health workers. The disproportionate inflammatory phenomenon that caused the infection would explain this long COVID-19 [17]. New symptoms also appeared in some, dominated by asthenia (16.2%), chest pain (13.5%), headache (10.8%), stress (13.5%) and depression (8.1%), which are probably late manifestations of the disease or other organ damage. This situation motivated a specialised consultation for 14.5% of the health workers in the departments of pneumology, cardiology, neurology and psychology respectively in 55.5%, 22.2%, 22.2% and 22.2% of the cases. The follow-up of patients cured of COVID-19 remains necessary to understand the disease and relieve the victims. The scientific uncertainties about this new highly contagious disease, which has caused thousands of deaths in some countries, were the cause of the observed stress and depression. This situation motivated the psychosocial care of health workers. There is a need to systematically integrate psychosocial care into the response, not only for patients but also for health workers under a lot of stress daily. With these new emerging diseases, the implications of which we do not know, tribute must be paid to these health care workers in a situation of very high risk of infection transmission.
Stigmatisation is very important during health emergencies. In our study, 38 health workers (61.3%) reported experiencing stigmatizing attitudes more frequently from their neighbours, from their co-workers who were not in the care sites and even from their own families for some. In Hawaii, Professor Guo reported that many nurses wanted to resign; some reported feelings of rejection from the community [18]. Strengthening communication would allow them to work without prejudice.
When asked to assess their care, twenty health workers (32.3%) were not satisfied. The dissatisfaction concerned the disinfection of their homes, the screening of family members who were contacts, the management of their results and the indiscretion of the management teams who arrived at their homes by ambulance, subject to stigmatisation by the neighbours. Indeed, during this crisis, there were delays in executing of certain tasks due to logistical difficulties and numerous shortcomings observed in the management of cases. The management of this pandemic has exposed our health system and challenges us to learn from this pandemic and to be better prepared for future pandemics with a well- structured response.
Conclusion
Health care workers are vulnerable because they are particularly exposed during epidemics. The sources of contamination in the health care environment are remarkably diverse and frequent. With the emergence of pandemic diseases, it would be appropriate to strengthen the mechanisms and arrangements for responding to pandemics in our country, as they will become increasingly frequent. A multidisciplinary approach including preventive, clinical and occupational medicine would ensure that health care workers are adequately taken care of in their primary mission, which is to save lives while remaining alive.
Ethical considerations
The study was submitted to the national ethics committee for health science research in the vulnerability and COVID -19 section, with a favorable opinion by deliberation n ° 2020-7-136.
- Conflicts of interest The authors, declare that they have no competing interest.
- Acknowledgements We thank the ministry of health, all health workers who agreed to participate in the study, all the healthcare workers at COVID-19 centre who contributed to collecting data in Ouagadougou and to the COVID-19 management response team in Burkina Faso. We thank and all those who took part in the study.
- Funding :The study did not receive funding
References
-
WHO-2019-nCoV-Surveillance_Case_Definition-2020.1- fre.pdf.
-
(2021) Ministère de la santé du Burkina Faso.
-
Folgueira MD, Munoz-Ruiperez C, Alonso-Lopez MA, et al. (2020) SARS-CoV-2 infection in health care workers in a large public hospital in Madrid, Spain, during March 2020. Preprint. medRxiv.
-
Nguyen LH, Drew DA, Joshi AD, Guo CG, Ma W, et al. (2020) Risk of COVID-19 among frontline healthcare workers and the general community: a prospective cohort study. medRxixv. 6
-
Ran L, Chen X, Wang Y, Wu W, Zhang L, et al. (2020) Risk Factors of Healthcare Workers with Corona Virus Disease 2019: A Retrospective Cohort Study in a Designated Hospital of Wuhan in China. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 71(16): 2218-2221.
-
Wang J, ZhouM, Liu F (2020) Reasons for healthcare workers becoming infectedwith novel coronavirus disease 2019 (COVID-19) in China. Letter to the Editor J Hosp Infect. 105(1): 100-101.
-
European Centre for Disease and Prévention Control (2020) Coronavirus disease 2019 (COVID-19) in the EU/ EEA and the UK. ninth update.
-
WHO (2020) Report of the WHO-China joint mission on coronavirus disease 2019 (COVID-19).
-
Wang D, Hu B, Hu C, Zhu F, Liu X, et al. (2020) Clinical characteristics of 138 hospitalised patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China. JAMA 323: 1061-1069.
-
Schwartz J, King CC, Yen MY (2020) Protecting health care workers during the COVID-19 coronavirus outbreak - lessons from Taiwan’s SARS response. Clin Infect Dis.
-
Greffe S, Espinasse F, Duran C, Labrune S, Sirol M, et al. (2020) Évaluation par RT-PCR du portage nasopharyngé du SARS-Cov-2 chez les personnels de santé symptomatiques suspects de COVID-19 dans un CHU de la banlieue parisienne. Rev Médecine Interne 41(8): 510-516.
-
Maltezou HC, Dedoukou X, Tseroni M, Tsonou E, Raftopoulos V, et al. (2020) SARS-CoV-2 infection in healthcare personnel with high-risk occupational exposure: evaluation of seven-day exclusion from work policy. Clinical Infectious Diseases.
-
Nadia Chahed (2020) Coronavirus en Afrique : quels sont les pays impactés?
-
Mingkun Zhan (2020) Death from Covid-19 of 23 Health Care Workers in China National Health Commission of the People’s Republic of China. Transcript of the press conference of the China-WHO Joint Expert Investigation Team on Covid-19. N Engl J Med.
-
CDC US (2020) Characteristics of Health Care Personnel with COVID-19 — United States FA, Morb Mortal Wkly Rep MMWR 69(15): 477-481.
-
Wu Z, McGoogan J (2020) Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72,314 cases from the Chinese center for disease control and prevention. JAMA 323(13): 1239-1242.
-
Burrell CJ, Howard CR, Murphy FA (2017) Coronaviruses. In: Fenner and White’s Medical Virology [Internet]. Elsevier. pp. 437‑446.
-
Guo Leon, Franciesco Violante (2020) Managing the COVID-19 outbreak for healthcare workers: Situation in Taiwan and Italy, March 20, 2020, Archives of Occupational and Environmental Diseases 81(3): 222- 223.
- Epidemiological and Clinical Aspects of Intestinal Parasitoses Among Students in the City of Bocaranga, Central African Republic
- Artificial Intelligence Empowers Global Infectious Disease Prevention and Control: Opportunities and Challenges
- Factors that Affect the Incidence of Babesia and Blood Donor Testing in Select States: A Regression Analysis
- Neuro-TB: The Battle between Tuberculosis and the Nervous System
- The Biological and Health Implications of Cat Fleas (Ctenocephalides felis): Assessing Zoonotic Risks and Hygiene Strategies
- Biostatistical Analysis of Medicinal Plants for Treating Schizophrenia