Myopericarditis Associated to mRNA Vaccine in Adolescents: Report of Two Cases
Myopericarditis related to mRNA SARS CoV2 vaccines in adolescents is a rare side effect and currently reported after the second dose of Pfizer-BioNTech dose. Here we describe two cases without severity signs or complications after inpatient follow-up and ambulatory treatment. Although treatment is still controversial a good prognosis and non-sequela after injury is expected. A correct approach and suspect diagnosis of myocarditis in children must be excluded after compatible symptoms and recent COVID-19 vaccination and discarding other potential infections.
Introduction
Novel coronavirus SARS Cov2 cause the current COVID-19 pandemic and promotes an emergent vaccines production with different technologies. The mRNA vaccines (Pfizer-BioNTech/Moderna) are now authorized and applied for children and adolescents with rare severe side effects reported. Two different syndromes have been reported after COVID-19 vaccination, including myocarditis such as pericarditis. Myocarditis has been reported mostly in young patients after the second vaccination dose, and in turn, pericarditis has been reported in older patients both after the first and second doses [1]. This inflammatory complication is not COVID-19 vaccine specific process, since historically myopericarditis events have been reported in the literature despite the introduction of new technologies in the development of vaccines, among the most common are measles and anthrax [2].
Case 1
A Brazilian male of 14 years old without underlying diseases; refer application of second dose of mRNA vaccine (Pfizer BioNTech). Symptoms start 48 hours after vaccination with frontotemporal headache, precordial pain that arise with postural changes, fever (102.2 °F) and dyspnea. At urgency room was hemodynamically stable. Laboratories excluded infectious etiologies. At EKG an incomplete right bundle branch block was detected and echocardiogram findings suggestive of pericardial effusion and myocarditis, serum high levels of I troponin and creatin kinase; it was excluded COVID-19 by PCR-RNA, request IgG-N protein antibodies no detected and IgG anti-Spike detected due to previous vaccination (patient receiving first dose at 06.01.2021). Cardiac MRI with Gadolinium was performed finding inflammatory process of myocardial and pericardium tissue without coronary involvement (Figure 1,2). Treatment was given with SNAID therapy (ketorolac) and steroid at immunosuppressive and anti-inflammatory dosage (methyl prednisone) for 72 hours. The evolution has been successful, with remission of fever and precordial pain. The patient has
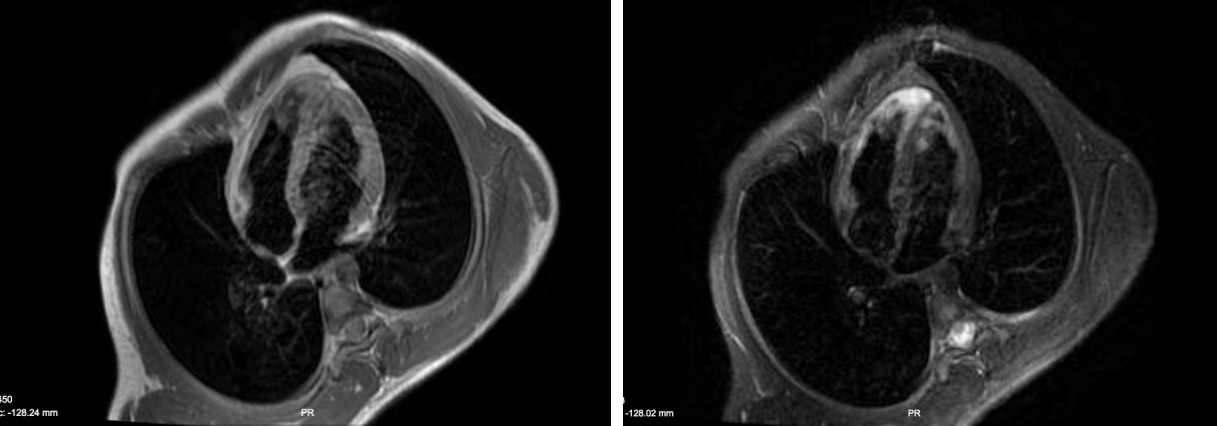
ambulatory treatment with a daily dose of acetylsalicylic acid 100 mg per 4 weeks, after therapy no symptoms were reported in follow-up, he returned to his country. This is the first myopericarditis attributed to mRNA vaccines reported in our center.
Figure 1 and 2: A 14-year-old boy post vaccine application of mRNA Pfizer BioNTech with clinical signs and myocardial laboratories diagnostic Myopericarditis. Cardiac MRI is performed with Gadolinium: Inflammatory process with coaptation of contrast at epicardium and myocardial edema.
Case 2
A Mexican male of 18 years old develop after 5 days of 2nd dose of mRNA vaccine (Pfizer BioNTech) the follow symptoms: fever, precordial pain and fatigue, at physical exam he shown diaphoresis and pallor, hemodynamically stable. Laboratories founding with leukocytosis (15,600 cel/ ml) and thrombocytopenia (45,000 count), acute COVID-19 or other infections were excluded, renal and hepatic function revealed adequate levels to age, elevated D Dimer and I Troponin was elevated. Thoracic X ray without anormal findings, alteration of EKG was reported with ST elevation, no echocardiogram or MRI was realized but clinic diagnostic was made. SNAID (Ketoprofen)100 mg every 8 hours and acetylsalicylic acid 100 mg per 4 weeks was administrated as treatment with no side effects or complications, the patient doesn´t require hospitalization.
Discussion
Classically, both myocarditis-pericarditis are defined as acute inflammatory processes that can originate from many predisposing conditions such as infections, autoimmune diseases, rheumatic fever, uremia, cancer, as reactions to drugs or after surgeries. Up to a third have no identifiable causes and are considered idiopathic [3]. The exact incidence and prevalence have not been established; however, it is estimated at 17 per 100,000 people, representing 0.1% of total hospital admissions [4].
Some cases have been reported after COVID-19 vaccination, with reports predominantly after the use of RNA vaccines (BNT162b2 mRNA-Pfizer-BioNTech and the mRNA- 1273-Moderna). According to the FDA [5], the estimated risk rate so far for myocarditis after the administration of the vaccine for COVID-19 is 1.2 and 10.4 per million after the administration of the first and second doses, respectively, for patients between 16 and 39 years of age old. In these patient reports [6] almost all presented chest pain, usually 2 to 3 days after vaccination preceded by fever and myalgias. Most patients are young, male, and without a history of COVID-19 infection or comorbidities. Most with sufficient spike antibody levels to indicate immunization. All cases with elevated cardiac troponins (with a maximum peak 3 days after vaccination), also with abnormalities in the electrocardiogram (ECG) with ST elevation in most cases, few patients with some with changes in the ejection fraction in the echocardiogram as we shown in these two cases. The cardiac magnetic resonance imaging study has also been an element that has been used to corroborate the diagnosis, in almost all patients with anomalies that suggest myocarditis or myocardial edema. The C-Reactive Protein is elevated in almost all cases, as well as the natriuretic B peptic or the pro-B N-terminal peptic. Most of the patients have also reported improvement in symptoms and signs, as well as in the normalization of markers after medical management.
Standardized management of post vaccine myopericarditis has not yet been reported, and it is still unclear whether management with intravenous immunoglobulin and / or corticosteroids (in the absence of criteria for systemic multi-inflammatory syndrome) is necessary in all cases [7]. Since no cardiac biopsy was performed due to the stability of the patients, the pathophysiology of myocarditis in these patients remains indeterminate. In some studies, the use of ibuprofen or a non-steroidal anti-inflammatory drug (NSAID) such as ibuprofen has been suggested; it appears to exert a beneficial response and may represent a good initial management. The role of corticosteroids and intravenous immunoglobulin remains uncertain, but these agents may reduce the immune response produced by the vaccine and may play a role in patients who do not respond first-line to NSAIDs [8]. Centers for Disease Prevention continues to recommend COVID-19 vaccination for people over 12 years of age as the risk of more serious complications related to the infection is greater than the complications that can occur after vaccination [9]. It is necessary to continue with the collaborative registries of myocarditis related to the vaccination of COVID-19 that include the demographic registries, the clinical presentation and the behavior of biomarkers, as well as imaging studies to validate recommendations due to emergency use of mRNA vaccines nowadays.
Conclusion
mRNA SARS CoV2 vaccine could cause myopericarditis in adolescents as a brief side effect, the clinical evolution apparently is not affected by use of steroids or NSAID´s, there was no hemodynamic repercussion and ambulatory management was possible. For the novel pandemic of SARS CoV2 development of new technologies on vaccination are tools in control of the disease. Myocarditis is a possible related side effect or mRNA vaccine with no fatal or severity outcomes in adolescents so the experience and report of side effects are important to take appropriate recommendations in this population.
References
-
Diaz G, Parsons G, Gering S, Audrey RM, Ian VH, et al. (2021) Myocarditis and Pericarditis After Vaccination for COVID-19. JAMA 326(12): 1210-1212.
-
Su J, McNeil M, Welsh K, Marquez P, Carmen Ng, et al. (2021) Myopericarditis after vaccination, Vaccine Adverse Event Reporting System (VAERS), 1990-2018. Vaccine 39(5): 839-845.
-
Cartaya Blanco C, Bandler Parekh J (2010) Pericarditis. Pediatrics in Review 31(2): 83-84.
-
Manda Y, Baradhi K (2021) Myopericarditis. In: StatPearls. Treasure Island: Stat Pearls Publishing.
-
Tom Shimabukuro (2021) Vaccine and related biological products advixory comitee (VRBPAC). Meeting Presentation; FDA.
-
Bozkurt B, Kamat K, Hotez P (2021) Myocarditis with COVID-19 mRNA Vaccines. Circulation 144(6): 471-484.
-
Marshall M, Ferguson ID, Lewis P, Preeti Jaggi, Christina Gagliardo, et al. (2021) Symptomatic acute myocarditis in seven adolescents following Pfizer-BioNTech COVID-19 vaccination. Pediatrics 148(3): e2021052478.
-
Das BB, Kohli U, Ramachandran P, Nguyen HH, Gerald G, et al. (2021) Myopericarditis following mRNA COVID-19 Vaccination in Adolescents 12 through 18 Years of Age. J Pediatr 238: 26-32.e1.
-
Centers for Disease Control and Prevention CDC (2021) Vaccines & Immunizations. Myocarditis and Pericarditis Considerations.
- Epidemiological and Clinical Aspects of Intestinal Parasitoses Among Students in the City of Bocaranga, Central African Republic
- Artificial Intelligence Empowers Global Infectious Disease Prevention and Control: Opportunities and Challenges
- Factors that Affect the Incidence of Babesia and Blood Donor Testing in Select States: A Regression Analysis
- Neuro-TB: The Battle between Tuberculosis and the Nervous System
- The Biological and Health Implications of Cat Fleas (Ctenocephalides felis): Assessing Zoonotic Risks and Hygiene Strategies
- Biostatistical Analysis of Medicinal Plants for Treating Schizophrenia