Epidemiological and Clinical Characteristics of Imported Schistosomiasis in a Tertiary Teaching Spanish Hospital, 2015-2022
Background: Schistosomiasis is a parasitic disease greatly present in tropical and subtropical areas, and frequently diagnosed in travelers and migrants. Methods: This report summarizes epidemiological and clinical data from retrospective cases of imported schistosomiasis diagnosed from January 2015 to May 2022 in a national referral center for tropical diseases in Madrid, Spain. Results: From a total of 9,929 patients attended in our clinic in the study period there were 477 schistosomiasis diagnosis (4,4%). Time elapsed from travel to diagnosis was 120 days (IQR 26-680). Most cases (28.1%) were diagnosed in immigrants from endemic areas, followed by 24.5% of travelers. In up to 34.5% of cases the diagnosis was a result of screening in asymptomatic subjects, 17% presented fever and 15% diarrhea. Almost all cases were diagnosed by serology and eggs in urine or feces were identified in only 11 patients (2.2%). Conclusions: Imported schistosomiasis is a chronic and asymptomatic disease that can be diagnosed in most patients by serology. It is important to advice travelers to avoid freshwater baths in endemic areas and get screened if they have been exposed to the parasite.
Introduction
Schistosomiasis the second most prevalent parasite disease, after malaria, with nearly 240 million people affected by this neglected tropical disease [1]. Although its transmission has been classically reported in 78 tropical and subtropical countries, mostly in sub-saharian Africa [2, 3], in the last years European autochthonous cases have been described, evidencing the capacity of this parasite to spread to new areas [4, 5, 6]. In regions where schistosomiasis causes significant disease, mass drug administration of praziquantel is the current main strategy for disease control. Depending on disease prevalence, this antiparasite drug is supplied to school-aged children (5-14 years of age) or to the entire community, usually as a yearly dose [7].
The two major forms of schistosomiasis, intestinal and urogenital, are caused by 5 main species of blood flukes. S. mansoni, S. haematobium, S. guineensis (previously called S. intercalatum), S. japonicum and S. mekongi causes predominantly gastrointestinal disease whereas S. haematobium is most frequently implicated in urogenital disorders (Table 1). An intermediate host, an aquatic snail, is needed to complete the life cycle in freshwater: under appropriate conditions the eggs hatch and release miracidia, which swim and penetrate the snail. In the snail, miracidias develop into cercariaes, the trematode infective stage for humans. People become infected when larval forms penetrate the skin during contact with infested water and then develop into the adult worms [2]. The adult forms live in the blood vessels, where the females release eggs. Some of these eggs leave the body in the feces or urine, depending on the species, and continue the parasite’s life cycle. Others become trapped in body tissues, where they cause an immune reaction and progressive organ damage. Transmission occurs when people infected with schistosomiasis contaminate freshwater sources with eggs of the parasite, contained in their excreta, which then hatch in the water (Figure 1).
| Species | Geographic Distribution | |
|---|---|---|
| Intestinal schistosomiasis | Schistosoma mansoni | Africa, the Middle East, the Caribbean, Brazil, Venezuela and Suriname. |
| Intestinal schistosomiasis | Schistosoma japonicum | China, Indonesia y Philippines |
| Intestinal schistosomiasis | Schistosoma mekongi | Various districts of Cambodia and the Lao Democratic Republic |
| Intestinal schistosomiasis | Schistosoma guineensis and related Schistosoma intercalatum | Rainforest areas of Central Africa |
| Urogenital schistosomiasis | Schistosoma haematobium | Africa, the Middle East and Corsica (France). |
Table 1: Species and Distribution of Schistosomiasis.
![Figure 1: Global distribution of countries where human schistosomiasis is transmitted [8].](/fulltextimages/9959/fig_1.png)
In non-endemic areas, most of schistosomiasis diagnosis comes from imported cases [9]. Lack of awareness of this disease frequently results in late diagnosis [10]. Schistosomiasis in this context is often asymptomatic, and diagnosis is often made through specific screening based on travel risk factors. Nevertheless, there is a potentially serious acute presentation almost exclusively in non-immune visitors to endemic areas, known as Katayama fever, caused by a systemic hypersensitivity reaction that may occur weeks after the initial infection, especially by S. mansoni and S. japonicum. Despite being asymptomatic in most cases in early stages, schistosomiasis can lead to future complications depending on the Schistosoma species including bladder tumors [11], portal hypertension or neuroschistosomiasis [12]. Therefore, it is important to perform appropriate testing if the patient has been exposed to freshwater in endemic areas or if a traveler presents with haematuria [11].
Clinical presentation may have some differences between migrants and travelers. Migrants often consult in late stages probably related to the lack of awareness of the potential risk symptomless of disease and difficulty to medical access. In the other hand, travelers present with acute symptoms or presence of eosinophilia and therefore consult earlier after the exposure [9]. Additionally, there are reports of autochthonous cases of schistosomiasis in non- endemic countries such as Spain and France (Corsica), where the vector is established [4, 5]. Early diagnosis and treatment of infected patients in areas where the intermediate host is present is also crucial to avoid local transmission. Although the aim of World Health Organization (WHO) is to stop or diminish transmission in endemic areas, diagnosis test and treatment are not homogenous and well-established in non- endemic countries [13].
Materials and Methods
Study Population and Data Collection
With the aim of presenting demographic, clinical, and geographic features of imported schistosomiasis in a non- endemic area, we performed a retrospective observational study of schistosomiasis cases attended in the referral tropical Unit in Hospital La Paz- Carlos III in Madrid, Spain from January 2015 to May 2022. We included all cases over 18 years old with a positive microbiologic test for schistosomiasis. Clinical and epidemiological data were collected from medical records and included age, sex, country of birth, visited country, length of last travel, time elapsed between arrival and consultation, clinical symptoms, and diagnosis method. The diagnosis of schistosomiasis during the whole period of the study was carried out by enzyme- linked immunosorbent assay (ELISA), ELISA/NovaTec®. In this test, the cut-off for a positive result is set on 1.
Purpose of travel was divided in 6 different categories: tourist (those who travel for leisure), workers (if the purpose of the travel was to undertake some business), volunteers (travelers who have participated in any cooperation program abroad), expatriates (people who reside abroad), immigrant (those who came to Spain and have never returned to their countries of origin) and visiting friends and relatives or VFR ( those people born in endemic countries that return to visit their family and relatives to their country of birth). As they are two very different populations, we have separated patients in two different groups: population native from schistosoma endemic countries (immigrants and VFR) and patients natives from non-endemic countries (tourist, expatriates, volunteers and workers).
Screening Strategy
Patients arriving from schistosomiasis-endemic areas (sub-Saharan Africa, southeast Asia and some Latin American regions) were tested for schistosomiasis at clinicians’ discretion, irrespective of symptoms. If a positive serology result was found, stool, urine or tissular biopsy depending on clinical presentation were asked to rule out the presence of parasite ova in digestive or urinary tract. A positive serology for Schistosoma was considered as a probable case although we cannot assert an acute or chronic disease or a cross- reaction with other helminths. The presence of eggs in bodily fluids confirmed the diagnosis. Serology in travelers is a very helpful tool of screening and diagnosis while in immigrants cannot differentiate an old or chronic infection from a recent one or due to presumed cross-reactions with other helminths [14]. Additional blood smear, serologic or Polymerase Chain Reaction (PCR) in biologic samples testing could also be asked depending on the visited area, origin of patient or activities during travel, to rule out other concomitant diseases.
Statistical Analysis
Data were transferred in Excel (Microsoft, Redmond, CA) for data analysis. All data were analyzed with R (version 4.4.4, R Core Team (2020), Viena, Austria). Categorical data were presented as absolute numbers and proportions, and continuous variables were expressed as medians and interquartile ranges. The Bonferroni adjustment was used to test the significance of the variables, so that all variables with a p-value of less than 0.008 were considered significant. The study protocol was approved by the ethical institutional review board of the hospital.
Results
Complete database include a total of 9,929 adult patients attended at our clinic from January 2015 to May 2022: 2,929(29.49%) were tourist, 905(9.11%) volunteers, 1,064(10.71%) workers, 2,832(28.52%) immigrants, 1,493(15.03%) VFR and 239(2.40%) expatriates. There
were 467(4.70%) patients attended that had never traveled abroad. During the study time period there were 477(4.5 %) diagnosis of schistosomiasis. Cases were distributed by year as follows: 6.75% in 2015, 3.54% in 2016, 4.99% in 2017, 3.70% in 2018, 3.95% in 2019, 6.68% in 2020, 5.52% in 2021 and 5.04% in 2022. Of the 477 total diagnosis of schistosomiasis, 215(45.1%) involved patients from endemic areas (EC), and 262 (54.9%) patients from no-endemic countries (NEC). Within the 2,929 tourists registered in the database, there were 117(3.99%) with a schistosoma probable diagnosis. Prevalence of schistosomiasis among other groups was 33.89% in VFR (n=1493), 7.18% in volunteers (n=905), 5.92% in workers (n=1064), 7.11% in expatriates (=239) and 4.73% in immigrants (n=2832) (Figure 2).
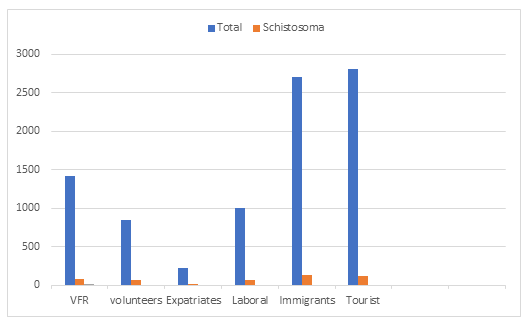
Figure 2: Total Schistosoma diagnosis according to type of travel group (from January 2015 to May 2022). The median age of the cases was 39 years old (IQR 31-47) and 242 (50.7%) were females. Most patients (260; 54.50%) were born in an European country (mostly Spain) and 116 (24.31%) were native from an African country. Additional data of patients diagnosed with schistosomiasis, according to type of travel, is presented in Table 2.
- Overall
- Volunteer Expatriate
- Workers
- Tourist
- Immigrant
- VFR p3 n
- 477
- 65
- 17
- 63
- 117
- 134
- 81
- 13.60%
- 3.60%
- 13.20%
- 24.50%
- 28.10%
- 17%
- Age [IQR]
- 39
- 34[29.40]
- 34[42.67]
- 40[34.44]
- 39[32.46]
- 37[29.49]
- 41[34.49]
- <0.001
- Sex (%)
- Men
- 239(49.3)
- 17(26.2)
- 9(52.9)
- 40(63.5)
- 50(50.4)
- 73(54.5)
- 37(45.7)
- 0.001
- Woman 242(50.7)
- 48(73.8)
- 8(47.1)
- 23(36.5)
- 58(49.6
- 61(45.5)
- 44(54.3)
- Travel length
- 28
- 85
- 1464
- 30
- 20
- -
- 30
- <0.001
- [IQR]a
- [2,116]
- [25,243]
- [148,2,052]
- [10,154]
- [11,31]
- [21,91]
- Time to diagnosis
- [IQR]b
- 120
- 84
- 415
- 58.5
- 122
- 214
- 129.5
- 0.17
- [26,680]
- [29,360]
- [18, 1,115] [13.2,376.7] [24, 1,078] [64, 1,561] [28.5,646.7]
Table 2: Demographic data of patients diagnosed of schistosomiasis 2015-2022 (n= 477).
We could identify 455 cases with a known country of probable or last exposition. All identified cases were imported, without any suspected autochthonous case. Schistosomiasis was most likely acquired in Africa (256 cases, 56.3%), especially in Equatorial Guinea (57 cases), Mali (19 cases) and Kenya (18 cases). Bolivia was the second country in frequency of schistosoma diagnosis, with 29 cases. Table 3 presents last travel destination prior to schistosoma diagnosis.
| Place of infection | N (%a) | Travel purpose | |||||
|---|---|---|---|---|---|---|---|
| NEC EC | |||||||
| Volunteers | Tourist | Workers | Expatriates | Immigrants | VFR | ||
| Africa | 256 (56.3%) | ||||||
| Equatorial Guinea | 57 | 1 | 1 | 8 | 4 | 20 | 23 |
| Mali | 19 | 4 | 3 | 7 | 5 | ||
| Kenya | 18 | 7 | 3 | 6 | 1 | 1 | |
| Senegal | 14 | 1 | 3 | 4 | 5 | 1 | |
| Angola | 13 | 2 | 6 | 1 | 1 | 3 | |
| Nigeria | 13 | 1 | 1 | 7 | 4 | ||
| Cameroon | 12 | 4 | 1 | 1 | 3 | 3 | |
| Mozambique | 12 | 3 | 5 | 2 | 2 | ||
| Guinea Conakry | 10 | 6 | 4 | ||||
| Uganda | 10 | 3 | 4 | 2 | 1 | ||
| America/ Caribbean region | 134 (29.5 %) | ||||||
| Bolivia | 29 | 1 | 1 | 1 | 18 | 8 | |
| Ecuador | 19 | 3 | 1 | 13 | 2 | ||
| Brazil | 17 | 1 | 5 | 5 | 4 | 2 | |
| Dominican Republic | 11 | 1 | 1 | 3 | 4 | ||
| Peru | 10 | 2 | 1 | 1 | 5 | 1 | |
| Venezuela | 10 | 2 | 1 | 1 | 5 | 1 | |
| Asia | 65 (14.3%) | ||||||
| Philippines | 16 | 1 | 6 | 1 | 5 | 3 | |
| Thailand | 11 | 11 |
Table 3: Last Travel destination according to type of travel in patients diagnosed of schistosomiasis 2015-2022. Only counties wi
Most patients (312; 65.4%) reported clinical symptoms at consultation, mainly fever (16.6). No case was diagnosed with acute schistosomiasis. Imported diseases screening was the most frequent reason for seek medical attention in EC and in NEC patients was diarrhea. Fever was the second reason for consultation in both groups. Other reported symptoms, according to type of travel, are represented in Table 4.
| NEC | EC | |||||||
|---|---|---|---|---|---|---|---|---|
| Total n (%a) | Volunteer n (%) | Expatriate | Workers n (%) n (%) | Tourist n (%) n (%) | Immigrant | VFRc n (%) | Pb | |
| Fever | 79(16.6) | 13(20) | 0 | 16(25.4) | 17(14.4) | 17(12.7) | 16(87.6) | 0.085 |
| Diarrhea | 71(14.9) | 14(21.5) | 1(5.9) | 16(25.4) | 25(21.4) | 8(6) | 7(88.9) | <0.001 |
| Dermatological symptomsd | 60(12.6) | 7(10.8) | 2(11.8) | 4(6.3) | 25(21.4) | 13(9.7) | 9(11.1) | 0.037 |
Table 4: [INLINE_TABLE:4:1]
Table 4: Symptoms at the time of consultation in patients diagnosed of schistosomiasis 2015-2022 (n= 312). where, acalculated on the basis of 477 diagnoses. bThe Bonferroni adjustment was used to test the significance of the variables, so that all variables with a p-value of less than 0.008 were considered significant. cVFR: visiting friends and relatives. dDermatological symptoms include any skin lesion, such as insect or animal bites, prurigo, cutaneous larva migrans, larva currens or rash.
A total of 165 cases (34.5%) were diagnosed by screening in asymptomatic patients, 103 (62.42%) patients of EC and 61(36.96%) from NEC. Respiratory and urinary symptoms were not registered. The median time elapsed between the travel and diagnosis was 120 days (IQR 26-680), 171 days in patients from EC and 88 days for NEC. In 8 cases (1.66% of the total of positive cases) Schistosoma eggs were found in feces, urine or tissular biopsy. All patients were diagnosed of probable schistosomiasis through a positive serology. Eosinophilia was present in 80 patients (16.8%), which was observed predominantly in EC patients (43.8%). The median eosinophilia count was 770x10e3/µl. Thirty patients with eosinophilia presented coinfection with strongyloidiasis, 10 with Toxocara and 2 with Loa-loa. In 227 Symptomatic patients (47.19%) an additional diagnosis was found, including strongyloidiasis in 41 patients (8.52 %), followed by malaria in 30 (6.24 %).
Discussion
This study examined patients diagnosed with probable schistosomiasis in a large national referral Unit in Spain. To our knowledge, this study is to date the largest Spanish single-center case series of human schistosomiasis providing epidemiology and clinical data of infected patients. The median age in this study was 39 years old, which is higher compared to the multi centric study carried out by TropNet (The European Network for Tropical Medicine and Travel Health) or to a large Italian series (1997-2010). This could be explained because of the higher prevalence of younger migrants in the TropNet sample and the different migration pattern in each country [9, 15].
Almost 90% schistosomiasis cases in published series were acquired from 78 different countries, most of them from Africa [1, 2, 3]. Travelers from European countries to tropical regions diagnosed of Schistosomiasis were mostly imported cases acquired in 34 different countries of Africa (252, 52.3%), as previously reported in other cohorts from non- endemic countries analyzing imported cases [15, 16]. This reflects the high endemicity of schistosomiasis in this region of the world, which harbours the highest number of cases. Similar to the multi centric European study of Geosentinel (a worldwide communication and data collection network for the surveillance of travel-related morbidity) most of our diagnoses were in immigrants [15, 17]. The most frequent geographic origins of immigrant patients in our study were Equatorial Guinea. The over-representation in our cohort of this country can be explained because the historical relationship with Equatorial Guinea, which was once a Spanish colony, results in many of our patients coming from this country.
Unexpectedly, we found 29 patients from Bolivia without a previous history of travel to tropical endemic countries and who have positive serology for Schistosomiasis. In this group we didn´t detect Schistosoma eggs in urine or feces. A high number of Bolivian patients are attended yearly in our unit because our center gathers a large cohort of patients with Chagas disease. WHO does not consider Bolivia an endemic country for schistosomiasis. However, one study reported that B. amazonica- a planorbid identified in Brazil and North Bolivia- is susceptible to strains of S. mansoni and has been proposed as a potential vector of the trematode [17, 18]. We have some hypotheses that might explain our findings: possible cross-reactions of the serology with other helminths, false positive serology, or unreported additional travel [10, 19]. We also found 19 people whose last travel was to Ecuador. This country is theoretically free of Schistosoma, and as previously discussed, we cannot ascertain the precise cause of these microbiological findings but one of the reasons we believe our study is relevant is because it can flag the likelihood of Schistosomiasis in countries where is not known to be present.
In line with the literature [9, 17, 20] schistosomiasis is frequently asymptomatic in NEC, as in our cohort. As shown in other series, the EC patients are diagnosed during the chronic phase and this explains symptomless. For those with symptoms, fever, diarrhea and dermatological manifestations were the most frequent reasons at consultation, but we cannot rule out that these were related to other diseases asides from schistosomiasis- as we report a number of concomitant infections at the time of schistosoma diagnosis. Urinary and respiratory specific symptoms were not reflected in many medical records. We did not have suspicion of acute schistosomiasis in persons with fever and this symptom was attributed to other infections, as malaria.
Diagnosis was made by ELISA test in all cases and we could only confirm it in 8 patients proving the presence of ova in different body fluids or tissular biopsy, of these 7 were EC and one was a tourist returning from Mali. ELISA test has a high predictive positive value and specificity [21]. Serological assays have proven useful clinically for diagnosis, especially for a symptomatic traveler although these tests strongly vary depends on the assay of the involved schistosoma species [8].
Marchese, et al. [15] described 103 patients with positive eggs in body fluids despite the fact that the percentage of immigrants in their series and in ours was similar. This may be due to a different urine and feces concentration technique or because the characteristics of the immigrants are not the same, as we do not usually attend asylum seekers or refugees. Finally, our microbiologists do not routinely search for eggs in urine unless microscopy haematuria is present, so this may be another possible explanation for the low number of eggs identified. Other test as western blot (WB), real-time polymerase chain reaction (RT-PCR), circulating cathodic antigen (CCA) or immunochromatographic tests can be used to diagnose schistosomiasis [9, 12, 17, 21], but we do not have them available in our hospital. The long period of time that has elapsed since the return from the last trip, which does not necessarily have to be the trip during which the infection was acquired, and the diagnosis should make us reflect on the implications of this delay in diagnosis and the risk of complications for the patient [5, 6]. This period of time elapsed since the return of the travel until the diagnosis, however prolonged, is similar to other series [9]. Yet, in our study we did not have any case of hepatosplenic or neuroschistosomiasis.
Schistosomiasis can produce eosinophilia, especially during the acute phase. In this study eosinophilia was found in 80 (16.8%) patients of whom, almost half of them were co- infected with another parasite that can explain the presence of this laboratory abnormality [22, 23, 24]. Since autochthonous transmission has been reported in Spain, we should be aware of this illness not only in immigrants or travelers but also in Spanish people with symptoms suggestive of schistosomiasis, especially if the patient resides or have been traveled to Almeria, in the southwest of Spain, where the snail has been established. Early diagnosis is crucial to prevent transmission in further regions of Spain [5]. Early detection of imported pathology in exposed and/or vulnerable population is also a fundamental backbone to prevent the transmission of pathogens in non-endemic areas. Persons from EC consulted later than NEC, this could point to a lower perception of risk in this population and should prompt clinicians to perform proactive screening.
Our study has several limitations. First and foremost, the retrospective nature of this study makes it difficult to retrieve some missing data. Second, the country last visited prior to schistosomiasis diagnosis does not have to be necessarily the country of infection. We cannot ascertain if eosinophilia or presenting symptoms can be related to schistosomiasis or to other concomitant diseases, although it highlights the importance of the microbiological study in travelers and migrants with these and other symptoms and analytical alterations. Being a single-center study means our data may not be applicable in other settings. Although coming from a large referral unit, the number of cases with parasite detection in feces and/or urine is very low and we do not have further diagnostic techniques other than serology which may limit our diagnostic capacity. As we do not include treatment evaluation and follow-up as an objective of the study, all this information is missing.
In the other hand, this study has some important strengths: all patients were attended in the same center, we can therefore ensure that a homogeneous evaluation and diagnosis of the patients has been made, the expertise of clinicians specifically dedicated to tropical diseases ensures a high level of suspicion of cases.
Data found in this study highlights the importance of giving appropriate pre-travel advice with particular emphasis on baths in freshwaters. Specific high-risk travelers might benefit from a post- travel evaluation. This is particularly important in patients that can be asymptomatic and return to areas of the world where the vector is present which can perpetuate disease transmission, especially in pathologies with long latency periods. Schistosomiasis is one of the most prevalent neglected tropical diseases, and it is up to us to contribute to its eradication.
Conclusions
Schistosomiasis remains a global health problem. Most of the diagnoses in our unit were in asymptomatic persons. This suggests that immigrants and persons with long-length travel to African countries should be offered screening regardless of the presence of symptoms. Travelers should be specifically advised about the risks of bathing freshwater and instructed to consult if symptoms suggestive of schistosomiasis appear. Post-travel screening should be considered in high risked persons to avoid future complications and to prevent further local cases in areas where the vector is established.
Author Contributions
All authors have contributed equally to this article. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by Ethics Committee of Hospital La Paz- Carlos III. HULP: PI-3707.
Informed Consent Statement
Informed consent was not necessary as the Ethics Committee resolved.
Data Availability Statement: Not applicable.
Acknowledgments
CIBERINFEC. Natalia Romero who helped us with the
data record. Maria Jimenez Gonzalez as a biostatistics. Thanks to all patients who selflessly have participated in the study.
Conflicts of Interest
The authors declare no conflict of interest.
References
-
WHO (2023) Schistosomiasis.
-
Onasanya A, Bengtson M, Oladepo O, Van Engelen J, Diehl JC (2021) Rethinking the Top-Down Approach to Schistosomiasis Control and Elimination in Sub-Saharan Africa. Front Public Health 9: 622809.
-
Colley DG, Secor WE (2014) Immunology of human schistosomiasis. Parasite Immunol 36(8): 347-357.
-
Ramalli L, Mulero S, Noel H, Chiappini JD, Vincent J, et al. (2018) Persistence of schistosomal transmission linked to the Cavu river in southern Corsica since 2013. Euro Surveill 23(4): 18-00017.
-
Coronas JS, Bargues MD, Serrano ABL, Artigas P, Orti AM, et al. (2021) Evidence of autochthonous transmission of urinary schistosomiasis in Almeria (southeast Spain): An outbreak analysis. Travel Med Infect Dis 44: 102165.
-
Arsuaga M, Menendez MD, Gobbi FG (2022) Autochthonous schistosomiasis in Europe: A silent threat. Travel Med Infect Dis 45: 102244.
-
WHO (2016) Helminth controls in school age children: a guide for managers of control programmes. World Health Organization, Geneva.
-
Colley DG, Bustinduy AL, Secor WE, King CH (2014) Human schistosomiasis. Lancet 383(9936): 2253-2264.
-
Lingscheid T, Kurth F, Clerinx J, Marocco S, Trevino B, et al. (2017) Schistosomiasis Investigator Group. Schistosomiasis in European Travelers and Migrants: Analysis of 14 Years TropNet Surveillance Data. Am J Trop Med Hyg 97(2): 567-574.
-
Palomar NM, Sulleiro E, Perez GI, Espiau M, Arandes AS, et al. (2020) Schistosomiasis in children: review of 51 imported cases in Spain. J Travel Med 27(1): taz099.
-
Poddighe D, Castelli L, Pulcrano G, Grosini A, Balzaretti M, et al. (2016) Urinary Schistosomiasis in an Adolescent Refugee from Africa: An Uncommon Cause of Hematuria and an Emerging Infectious Disease in Europe. J Immigr Minor Health 18(5): 1237-1240.
-
Bocanegra C, Salvador F, Sulleiro E, Montalva AS, Pahissa A, et al. (2014) Screening for imported diseases in an immigrant population: experience from a teaching hospital in Barcelona, Spain. Am J Trop Med Hyg 91(6): 1277-1278..
-
Cucchetto G, Buonfrate D, Marchese V, Rodari P, Ferrari A, et al. (2019) High-dose or multi-day praziquantel for imported schistosomiasis? A systematic review. J Travel Med 26(7): taz050.
-
Santano R, Rubio R, Pujol BG, Escola V, Muchisse O, et al. (2022) Evaluation of antibody serology to determine current helminth and Plasmodium falciparum infections in a co-endemic area in Southern Mozambique. PLoS Negl Trop Dis 16(6): e0010138.
-
Marchese V, Beltrame A, Angheben A, Monteiro GB, Giorli G, et al. (2018) Schistosomiasis in immigrants, refugees and travellers in an Italian referral centre for tropical diseases. Infect Dis Poverty 7(1): 55.
-
Leblanc C, Brun S, Bouchaud O, Izri A, Ok V, et al. (2021) Imported schistosomiasis in Paris region of France: A multicenter study of prevalence and diagnostic methods. Travel Med Infect Dis 41: 102041.
-
Comelli A, Riccardi N, Canetti D, Spinicci M, Cenderello G, et al. (2020) Delay in schistosomiasis diagnosis and treatment: a multicenter cohort study in Italy. J Travel Med 27(1): taz075.
-
WHO (2021) Status of schistosomiasis endemic countries.
-
Simoes LF, Bastos LDB, Camargo EAF, Neves MF, Linhares AX, et al. (2017) Host-parasite relationship between Biomphalaria amazonica (Paraense, 1966) and Schistosoma mansoni (Sambon, 1907). Braz J Biol 77(2): 340-346.
-
Hinz R, Schwarz NG, Hahn A, Frickmann H et al. (2017) Serological approaches for the diagnosis of Schistosomiasis-A review. Mol Cell Probes 31: 2-21.
-
Coltart C, Whitty CJM (2015) Schistosomiasis in non- endemic countries. Clin Med (Lond) 15(1): 67-69.
-
Beltrame A, Guerriero M, Angheben A, Gobbi F, Mendez AR, et al. (2017) Accuracy of parasitological and immunological tests for the screening of human schistosomiasis in immigrants and refugees from African countries: an approach with Latent Class Analysis. PLoS Neglected Trop Dis 11(6): e0005593.
-
Baaten GG, Sonder GJ, Gool TV, Kint JA, Hoek AVD (2011) Travel-related schistosomiasis, strongyloidiasis, filariasis, and toxocariasis: the risk of infection and the diagnostic relevance of blood eosinophilia. BMC Infect Dis 11: 84.
-
Bierman WF, Wetsteyn JC, Gool TV (2005) Presentation and diagnosis of imported schistosomiasis: relevance of eosinophilia, microscopy for ova, and serology. J Travel Med 12(1): 9-13.
- Epidemiological and Clinical Aspects of Intestinal Parasitoses Among Students in the City of Bocaranga, Central African Republic
- Artificial Intelligence Empowers Global Infectious Disease Prevention and Control: Opportunities and Challenges
- Factors that Affect the Incidence of Babesia and Blood Donor Testing in Select States: A Regression Analysis
- Neuro-TB: The Battle between Tuberculosis and the Nervous System
- The Biological and Health Implications of Cat Fleas (Ctenocephalides felis): Assessing Zoonotic Risks and Hygiene Strategies
- Biostatistical Analysis of Medicinal Plants for Treating Schizophrenia