Escobar Syndrome in Three Patients of Two Unrelated Families
“Escobar syndrome” or “multiple pterygium syndrome” is a very rare disorder. It is characterized by congenital contractures (arthrogryposis), excessive webbing (pterygia) and scoliosis. The diagnosis is generally confirmed after birth, in the neonatal period. We describe three individuals, from two consanguineous Algerian families, affected by this syndrome. The genetic defect is a mutation of the foetal subunit of Acetyl Choline receptor.
Introduction
The CHRNG (Cholinergic Receptor Nicotinic Gamma subunit) gene, carried on the short arm of chromosome 8, codes for the foetal Gamma subunit of the acetyl choline receptor (AChR), at the post-synaptic membrane of the motor endplate [1]. Its mutations were first discovered in 2006 [2]. Some ten mutations have been identified to date. Many mutations in other AChR subunits are lethal at birth [3]. In contrast, many others are viable [4], causing congenital myasthenic syndromes known as “pre-natal”, and classified as “Escobar syndrome” or congenital multiple pterygium syndrome. It is an autosomal recessive condition characterized by excessive webbing (pterygia), congenital contractures (arthrogryposis) and scoliosis [5, 6]. Congenital contractures are due to a reduction in active foetal movements at sensitive moments in development [7], as a result of neuromuscular damage [8]. On the other hand, patients show no myasthenic symptoms later in life (the adult subunit takes over). This is the main difference with mutations in other AChR subunits.
In this case series, we describe the phenotype of two Algerian families with Escobar syndrome.
Family 1: Two daughters (F1P1 and F1P2) from a consanguineous marriage (Figure 1). They are now aged 16 and 17.
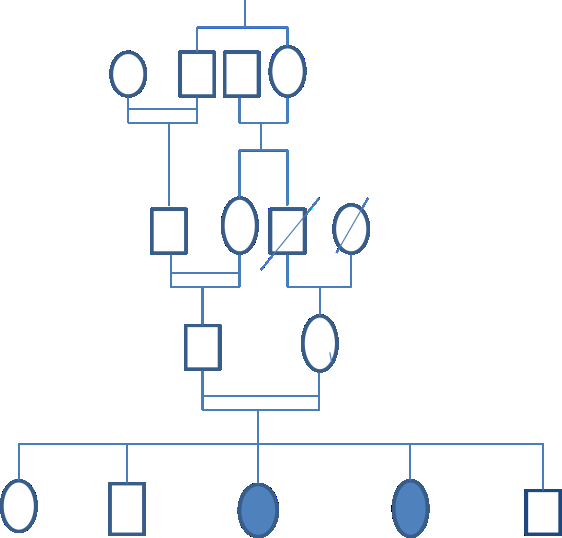
Their phenotype is fairly homogeneous. Their births were uneventful, with the exception of neonatal distress in patient F1P1. On the other hand, both were born with arthrogryposis of all four limbs and pterygia of the neck and elbows. In patient F1P1, scoliosis and valgus feet were observed.
Current neurological examination still reveals arthrogryposis, multiple pterygia and global amyotrophy; Neostigmine testing is negative. The QMG (quantitative myasthenia gravis) score was 4/39 in both cases. Electromyography (EMG) with repetitive stimulation of several nerve/muscle pairs was normal in patient F1P1; it was not performed in the sister. Respiratory function tests revealed a restrictive syndrome in both patients. Muscle biopsy in F1P1 was normal.
No medical treatment was proposed, apart from functional rehabilitation and orthopaedic management, given the significant deformities.
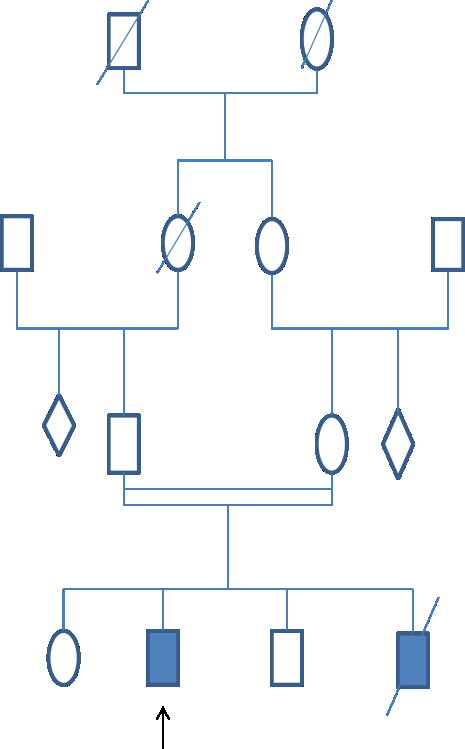
Family 2: A patient (F2P), currently aged 25, from a consanguineous marriage, with a similar case in the family (his brother died at birth in respiratory distress on arthrogryposis and multiple pterygiums) (Figure 2) illustrates their family tree.

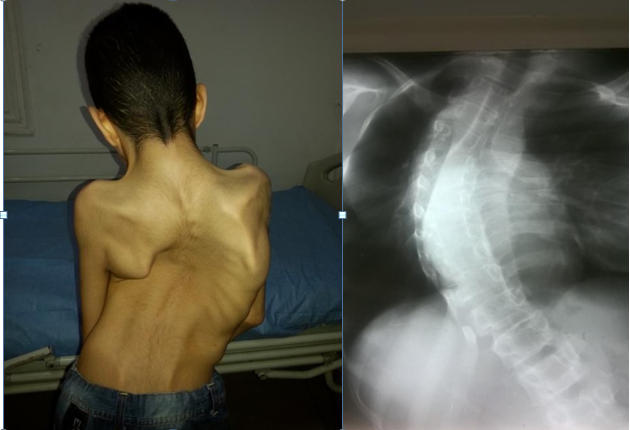
Our propositus, seen at the age of 16, presented with discrete axial hypotonia at birth with neonatal distress, dyspnea and a significant malformative syndrome. Current neurological examination revealed diffuse arthrogryposis, multiple pterygiums, especially in the axillae and elbows (Figure 3), as well as low ear and hair implantation, genu valgum, a stiff pelvis and severe scoliosis (Figure 4). The QMG score is 4/39.

The patient has given us permission to use these photos.
The patient has given us permission to use these photos.
Respiratory function tests revealed a restrictive syndrome. EMG with repetitive nerve stimulation of six nerve/muscle pairs was without abnormalities. Management consisted of functional and orthopaedic rehabilitation. Scoliosis surgery was also proposed, given the respiratory prognosis.
| F1P1 | F1P2 | F2P | |
|---|---|---|---|
| Sex | Female | Female | Male |
| Current age (years) | 16 | 17 | 25 |
| Age at onset | Birth | Birth | Birth |
| Consanguinity | + | + | + |
| Neonatal hypotonia | - | - | + |
| Neonatal respiratory distress | + | - | + |
| Arthrogryposis | ++ | ++ | ++ |
| Pterygiums | ++ | + | ++ |
| Facial dysmorphia | - | - | + |
| Scoliosis | + | + | +++ |
| Other deformities | Valgus feet | - | Genu valgum / Stiff pelvis |
| Neostigmine test | - | Not done | - |
| EMG | Normal | Not done | Normal |
| Respiratory test | Restrictive syndrome | Restrictive syndrome | Restrictive syndrome |
| Muscle biopsy | Normal | Not done | Not done |
Table 1: Summarizing the phenotype of our two Escobar families.
Discussion
The phenotypic data of our 3 patients are consistent with the suspected diagnosis of Escobar syndrome: growth retardation, multiple pterygiums, arthrogryposis, kyphoscoliosis. The main features of this condition were initially described by Matocsy in 1936, but the spectrum was later detailed in 2006 [9]. Our 3 patients have a fairly homogeneous phenotype with this malformative syndrome and these congenital deformities, in consanguineous families. The only differences were the death at birth of a patient from the family 2, and the very severe scoliosis of the propositus from the same family. There were no myasthenic symptoms in either family. Nevertheless, there are no pterygiums of the fingers and toes, as was the case in an Egyptian patient [10], and an Indian one [11].
| Hoffman and al series [2] | Our series | |||||
|---|---|---|---|---|---|---|
| P1 | P2 | P3 | F1P1 | F1P2 | F2P | |
| Sex | Female | Female | Male | Female | Female | Male |
| Age at diagnosis (years) | 12 | 21 | 5 | 14 | 13 | 16 |
| Respiratory distress | + | - | - | + | - | - |
| Arthrogryposis | + | + | + | + | + | + |
| Pterygiums | + | + | + | + | + | + |
| Short stature | + | + | + | - | - | + |
| Scoliosis | + | + | + | + | - | ++ |
| Facial dysmorphia | + | + | - | - | - | + |
| Myasthenic symptoms | - | - | - | - | - | - |
Table 2: Phenotypic comparison with literature.
A phenotypic comparison was also made with 3 of the 12 patients, described for the first time, and carrying mutations in the CHRNG gene [2] (Table 2).
The phenotype of our patients remains homogeneous and perfectly in line with the phenotypes reported in the literature with CHRNG gene mutations.
Management remains purely orthopaedic, in view of the severe handicap caused by the dysmorphic syndrome, particularly scoliosis, which can induce respiratory impairment with prognostic consequences. The patient’s autonomy can also be greatly impaired by pterygiums in the elbow, hips and knees, which restrict joint movement [12].
Conclusion
Escobar syndrome is responsible for non-lethal multiple pterygium syndrome. Its phenotype is fairly typical and characteristic, despite its rarity. The main aetiology is a mutation in the CHRNG gene, which codes for a foetal subunit of the acetyl choline receptor. Multidisciplinary management is required for this kind of orphan condition, given the motor and respiratory functional prognosis that could be impacted.
References
-
Bissinger RL, Koch FR (2014) Nonlethal multiple pterygium syndrome: Escobar syndrome. Adv Neonatal Care 14(1): 24-29.
-
Hoffmann K, Muller JS, Stricker S, Megarbane A, Rajab A, et al. (2006) Escobar syndrome is a prenatal myasthenia caused by disruption of the acetylcholine receptor fetal gamma subunit. Am J Hum Genet 79(2): 303-312.
-
Vogt J, Harrison BJ, Spearman H, Cossins J, Vermeer S, et al. (2008) Mutation analysis of CHRNA1, CHRNB1, CHRND, and RAPSN genes in multiple pterygium syndrome/fetal akinesia patients. Am J Hum Genet 82(1): 222-227.
-
Dodson CC, Adjei OB (2005) Escobar syndrome (multiple pterygium syndrome) associated with thoracic kyphoscoliosis, lordoscoliosis, and severe restrictive lung disease: a case report. HSS J 1(1): 35-39.
-
Escobar V, Bixler D, Gleiser S, Weaver DD, Gibbs T (1978) Multiple pterygium syndrome. Am J Dis Child 132(6): 609-611.
-
Rajab A, Hoffmann K, Ganesh A, Sethu AU, Mundlos S (2005) Escobar variant with pursed mouth, creased tongue, ophthalmologic features, and scoliosis in 6 children from Oman. Am J Med Genet A 15: 134A(2): 151-157.
-
Hammond E, Donnenfeld AE (1995) Fetal akinesia. Obstet Gynecol Surv 50(3): 240-249.
-
Hall JG (1997) Arthrogryposis multiplex congenita: etiology, genetics, classification, diagnostic approach, and general aspects. J Pediatr Orthop B 6(3): 159-166.
-
Parashar SY, Anderson PJ, McLean N, Djohansjah M, David DJ (2006) Spectrum of features in pterygium syndrome. Asian J Surg 29(2): 104-108.
-
Shawky RM, Sadik DI (2011) The role of genomics in prevention or reducing the impact of congenital malformations. Genet Couns 22(2): 135-141.
-
Amalnath DS, Subrahmanyam DK, Sridhar S, Dutta TK (2011) Escobar syndrome in three male patients of same family. Indian J Hum Genet 17(1): 22-25.
-
Bissinger RL, Koch FR (2014) Nonlethal multiple pterygium syndrome: Escobar syndrome. Adv Neonatal Care 14(1): 24-29.
- Ramsay Hunt Syndrome Presenting as Gait Imbalance without Facial Paralysis: A Case Report
- Unveiling Hidden Culprits: An Observational Study of Upper Gastrointestinal Endoscopy Findings in Symptomatic Cholelithiasis Patients
- Assessing Health Care Providers’ Proficiency in International Patient Safety Goals: A Study to Assess the Knowledge &Practice on Patient Safety in a Tertiary Care Teaching Hospital in Gujarat
- Challenges in Diagnosing Child Language Disorders
- Stunting Service Management Model in the South-Central Timor Region, East Nusa Tenggara, Indonesia
- Acute Small Bowel Obstruction Presenting as Gangrenous Jejunal Loop Secondary to Intestinal Endometriosis – A Rare Case Report