Risk Assessment in Non-Variceal Upper Gastrointestinal Bleeding: A Comprehensive Review of Scoring Systems
Non-variceal upper gastrointestinal bleeding (NVUGIB) is a critical medical emergency with significant morbidity and mortality rates. The primary cause of NVUGIB is peptic ulcers. Proper risk assessment is vital for the efficient management of NVUGIB patients, impacting both clinical decisions and healthcare resources. Established scoring systems like the Rockall score (RS), Glasgow-Blatchford score (GBS), and AIMS65 have been instrumental in guiding clinical decisions. Their strengths, limitations, and areas of application are discussed. The emerging ABC score, with its potential to outperform existing systems, is highlighted, emphasizing its relevance in both upper and lower GI bleedings. However, The ABC score, though promising, necessitates further research for broader clinical adoption.
Introduction
Non-variceal upper gastrointestinal bleeding (NVUGIB) typically necessitates emergency intervention and is characterized by high mortality and morbidity rates. The most common cause of NVUGIB is peptic ulcers, accounting for around 31% to 67% of cases [1]. In addition to this, Mallory- Weiss syndrome, Dieulafoy lesions, vascular malformations, and tumors are also included [2]. Despite advancements in endoscopic equipment and pharmacotherapy, the prevalence of NVUGIB is reported to be high, ranging from 3.5% to 7.4% [3, 4, 5]. Hence, efforts to predict progression and prognosis in patients with bleeding are imperative. Several scoring systems have been reported for risk assessment in NVUGIB patients, but many are not widely used in clinical settings due to their complexity. Generally, it is recommended to perform endoscopic examinations within 24 hours for NVUGIB patients; however, early endoscopy and intensive treatment are required in high-risk groups [6]. Thus, executing prompt and accurate medical treatment based on the scoring system can be helpful. This review explores various scoring systems for assessing risk in patients presenting with NVUGIB.
Risk assessment in NVUGIB not only aids in the clinical management of individual patients but also has broader implications on hospital resources and healthcare economics [7, 8]. Early risk stratification can prioritize those in dire need of intervention, optimizing bed allocation in intensive care units and helping in timely decision-making regarding the need for invasive procedures [9]. Moreover, by effectively identifying low-risk patients, it prevents unnecessary hospitalizations, reducing the economic burden on healthcare systems and improving overall patient care efficiency.
Initial Evaluation and Fluid Therapy
Treatment for patients presenting with NVUGIB must be individualized, varying according to the underlying disease causing the bleeding. However, it is crucial to measure vital signs in all patients upon admission to ascertain their hemodynamic status and commence appropriate fluid therapy [1]. Vigorous monitoring and fluid and transfusion therapy are needed from the outset in patients presenting with signs of severe bleeding, such as neurological manifestations, hypotension, tachycardia, or oligouria [10]. Even in the presence of bleeding, physiological compensatory mechanisms can maintain blood pressure and normal hemoglobin levels initially, so careful observation is needed where massive bleeding is suspected.
Pre-Endoscopic Scoring Systems
Scoring systems to evaluate NVUGIB patients can be broadly categorized into those including endoscopic findings and those that do not. The Rockall score (RS), introduced in 1996, is one of the most commonly used scoring systems for NVUGIB patients [11]. It utilizes five variables, including age, shock, comorbidities, hemorrhagic etiology, and endoscopic evidence of bleeding, to predict the likelihood of death within 30 days for patients presenting with bleeding. Pre-endoscopic RS (PERS) is calculated by excluding from the five variables of RS the diagnosis causing the bleeding and endoscopic evidence of bleeding, which can only be determined by endoscopy. The Glasgow-Blatchford score (GBS) was developed to predict the need for transfusion, endoscopic treatment, surgery, and mortality [12]. GBS is based on blood urea, hemoglobin, systolic blood pressure, pulse rate, the presence of melena or syncope, and the presence of liver or heart disease, and has the advantage of being simple to calculate because there are no endoscopic findings and no need to obtain the extent of systemic disease. However, it has been pointed out that there are no clear criteria for determining the presence of liver disease or heart disease among the items in the GBS, and that the presence of blood urea and syncope do not represent the situation at the time of arrival at the hospital. For this reason, the AIMS65 score was recently developed, which can be easily calculated at the time of presentation to the emergency department [13, 14]. The AIMS65 score consists of five risk factors: hypoalbuminemia, prothrombin time prolongation, decreased consciousness, decreased systolic blood pressure, and advanced age, and has the advantage of being objectively and easily measured at the time of presentation. Recent studies have shown that AIMS65 is comparable to RS and GBS in predicting mortality [15]. In particular, some studies have shown an increase in mortality in patients with an AIMS65 score of 2 or more compared to those with a score of 2 or less [16]. However, other studies have reported an increase in mortality in patients with an AIMS65 score of 3 or more, suggesting that further research is needed on the appropriate AIMS65 cutoff value [17]. Recently, Japan published a new scoring system based on blood pressure, loss of consciousness, vomiting, hemoglobin levels, blood urea levels, glomerular filtration rate, and antiplatelet medications [18]. This scoring system has been shown to be better at predicting endoscopic hemostasis than RS, GBS, and AIMS65, but needs further validation in other countries. In Italy, a T-score using four factors (patient general condition, pulse rate, blood pressure, and hemoglobin) has been shown to be useful in predicting high-risk endoscopic bleeding foci and bleeding-related mortality [19]. Thus, it appears that the T-score may be helpful in identifying patients who need endoscopy at an earlier stage.
Post-Endoscopic Scoring Systems
As mentioned earlier, the RS uses five variables and is designed to predict the likelihood of death within 30 days in patients presenting with bleeding. The American Baylor score was published in 1993 and was designed to predict rebleeding in patients who underwent endoscopic hemostasis [20]. The Cedar Sinai score was published to predict prognosis and duration of hospitalization in patients with upper GI bleeding [21]. In a real-world comparison study, the RS was found to be superior in predicting low-risk patients in upper GI bleeding compared to the American Baylor and Cedar Sinai scores [22]. The Spanish Almela score was created to identify low-risk patients who could be treated on an outpatient basis [23]. More recently, the Italian Progetto Nazionale Emorragia Digestiva (PNED) score was created to predict mortality after bleeding and has been shown to be superior in predicting 30-day mortality when compared to the RS, but has not been validated outside of Italy [24]. Currently, the RS is the most commonly used scoring system that includes endoscopy, and no other scoring system has been shown to be superior. However, the RS has the disadvantage of being somewhat complex and only available at the time of endoscopy.
ABC Score: An Advanced Prognostic Instrument
The Age, Blood tests, and Comorbidities score, known as the ABC score, was formulated to predict mortality in individuals with upper and lower GI bleeding [25]. Initial data from the validation cohort, which included 4019
patients with upper GI bleeding and 2336 patients with lower GI bleeding suggests good performance for the score (AUROC 0.81 to 0.84). It outperforms predecessors like AIMS65 and GBS, efficiently identifying high-risk patients and ensuring optimal clinical responses [26]. In upper GI bleeding instances, the ABC score is invaluable, providing rapid and accurate assessments crucial for immediate, lifesaving interventions. Its superior predictive abilities can refine management strategies in gastrointestinal bleedings, improving patient care outcomes and broadening prognostic information availability. Continuous research and validations are crucial to unveil its full potential in everyday clinical practice and to consolidate its implementation in evolving medical guidelines, heralding a new era of individualized, advanced care in gastrointestinal bleeding management.
Factors Associated with Rebleeding
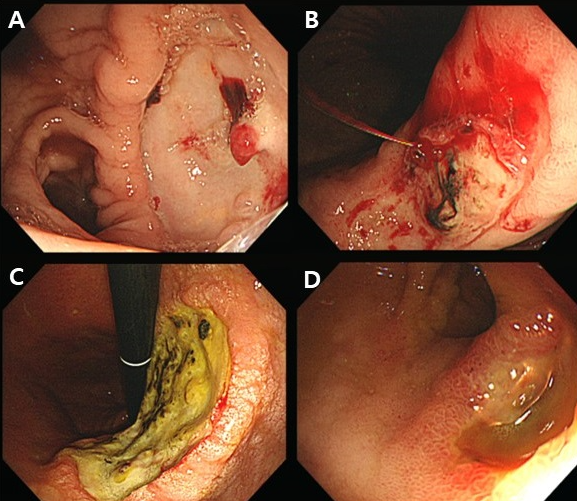
The recent meta-analysis identified several factors associated with an increased risk of rebleeding, including hemodynamic instability, evidenced by a systolic blood pressure of less than 100 mmHg or a heart rate exceeding 100 beats per minute, a hemoglobin level below 10 g/L, and endoscopic evidence of active hemorrhage. Moreover, the size and location of the ulcer are also critical; ulcers larger than 1 to 3 cm, especially those located in the posterior duodenal bulb or high on the lesser gastric curvature, are notably associated with a heightened risk of rebleeding (Figure 1) [27]. For patients with NVUGIB, the ACG (American Journal of Gastroenterology) Clinical Guidelines suggest a transfusion threshold at a hemoglobin level below 7 g/dL, with an adjusted threshold of 8 g/dL for hypotensive patients or those with cardiovascular concerns. This restrictive transfusion approach can mitigate further bleeding and mortality risks [28]. Concurrently, the ESGE(European Society of Gastrointestinal Endoscopy) emphasizes rapid assessment of hemodynamic status in acute NVUGIB cases, advocating for immediate intravascular volume replacement using crystalloid fluids for those hemodynamically unstable [6].
Conclusion
Non-variceal upper gastrointestinal bleeding (NVUGIB) remains a critical medical emergency due to its high morbidity and mortality, necessitating swift and precise risk assessment approaches [22, 29, 30]. Scoring systems such as RS, GBS, and AIMS65 offer valuable tools for clinicians, but each possesses distinct predictive advantages and limitations. For instance, regarding 30-day mortality, the AIMS65 showed an AUROC of 0.79, the clinical Rockall score registered 0.76, while the full Rockall score posted 0.81, and the GBS trailed at 0.61 [31]. Notably, AIMS65, both clinical and full Rockall scores performed well in predicting 30-day mortality, with no significant disparities among them. When assessing rebleeding risks, the clinical Rockall score (AUROC: 0.72), full Rockall score (AUROC: 0.77), and GBS (AUROC:
0.71) all demonstrated efficacy, outstripping AIMS65 which showed an AUROC of 0.61 [31].
Recently, the ABC score has surfaced as a potent tool, outperforming predecessors like AIMS65 and GBS by providing a comprehensive and swift prognostic outlook for both upper and lower GI bleedings [25, 32]. Such evaluations are essential for expeditious and precise clinical interventions. Although the ABC score hints at a promising future, ongoing research and validation are indispensable for its full realization in medical guidelines. The overarching aim remains to meld advanced and tailored care, honing these scoring systems for wider relevance, precision, and simplicity in diverse clinical environments, thereby refining prognosis and treatment modalities for NVUGIB patients.
| Category | Score Point | ||
|---|---|---|---|
| GBS | Blood urea, Hemoglobin, Sex, Systolic blood pressure, Pulse, Melena, Syncope, Hepatic disease, Cardiac failure | 0 point: Very low risk. Most of these patients can be safely managed as outpatients. | 0-23 |
| GBS | Blood urea, Hemoglobin, Sex, Systolic blood pressure, Pulse, Melena, Syncope, Hepatic disease, Cardiac failure | ≥1 point: Relatively higher risk. These patients may require admission or further evaluation. | 0-23 |
| AIMS65 score | Albumin, INR, Systolic blood pressure, Altered Mental status, Age | 0 point: Low risk of mortality | 0-5 |
| AIMS65 score | Albumin, INR, Systolic blood pressure, Altered Mental status, Age | 1 point: Moderate risk | 0-5 |
| AIMS65 score | Albumin, INR, Systolic blood pressure, Altered Mental status, Age | ≥2 points: High risk | 0-5 |
| Rockall score | Age, Shock, Comorbidity (Source of bleeding, Stigmata of recent bleeding) | 0-2 points: Low risk of rebleeding and mortality | 0-7 |
| (Post Rockall score) | Age, Shock, Comorbidity (Source of bleeding, Stigmata of recent bleeding) | 3-4 points: Moderate risk | (0-11) |
| (Post Rockall score) | Age, Shock, Comorbidity (Source of bleeding, Stigmata of recent bleeding) | ≥5 points: High risk | (0-11) |
| ABC score | Age, Blood urea, Albumin, Creatinine, Mental status, Liver cirrhosis, Disseminated malignancy, ASA score | 0-3 points: low risk of mortality | 0-18 |
| ABC score | Age, Blood urea, Albumin, Creatinine, Mental status, Liver cirrhosis, Disseminated malignancy, ASA score | 4-7 points: Moderate risk | 0-18 |
| ABC score | Age, Blood urea, Albumin, Creatinine, Mental status, Liver cirrhosis, Disseminated malignancy, ASA score | ≥8 points: High risk | 0-18 |
Table 1: Comparative Overview of Risk Assessment Scoring Systems in Gastrointestinal Bleeding. GBS Glasgow-Blatchford Bleeding Sc
Contributions
Constructing Table and Figure: Ah Young Lee Drafting Abstract: Hyun Take Lee, and Jun-young Seo Critical Revision for intellectual Content: Jun-young Seo
References
-
Kim KB, Yoon SM, Youn SJ (2014) Endoscopy for non- variceal upper gastrointestinal bleeding. Clin Endosc 47(4): 315-319.
-
Holster IL, Kuipers EJ (2012) Management of acute nonvariceal upper gastrointestinal bleeding: current policies and future perspectives. World J Gastroenterol 18(11): 1202-1207.
-
Hearnshaw SA, Logan RF, Lowe D, Travis SP, Murphy MF, et al. (2011) Acute upper gastrointestinal bleeding in the UK: patient characteristics, diagnoses and outcomes in the 2007 UK audit. Gut 60(10): 1327-1335.
-
Leontiadis GI, Molloy-Bland M, Moayyedi P, Howden CW (2013) Effect of comorbidity on mortality in patients with peptic ulcer bleeding: systematic review and meta- analysis. Am J Gastroenterol 108(3): 331-45.
-
Targownik LE, Nabalamba A (2006) Trends in management and outcomes of acute nonvariceal upper gastrointestinal bleeding: 1993-2003. Clin Gastroenterol Hepatol 4(12): 1459-1466.
-
Gralnek IM, Dumonceau JM, Kuipers EJ, Lanas A, Sanders DS, et al. (2015) Diagnosis and management of nonvariceal upper gastrointestinal hemorrhage: European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy 47(10): a1-46.
-
Adam V, Barkun AN (2008) Estimates of costs of hospital stay for variceal and nonvariceal upper gastrointestinal bleeding in the United States. Value Health 11(1): 1-3.
-
Marshall JK, Collins SM, Gafni A (1999) Prediction of resource utilization and case cost for acute nonvariceal upper gastrointestinal hemorrhage at a Canadian community hospital. Am J Gastroenterol 94(7): 1841- 1846.
-
Laursen SB, Leontiadis GI, Stanley AJ, Møller MH, Hansen JM, et al. (2017) Relationship between timing of endoscopy and mortality in patients with peptic ulcer bleeding: a nationwide cohort study. Gastrointest Endosc 85(5): 936-944.e3.
-
Cappell MS, Friedel D (2008) Initial management of acute upper gastrointestinal bleeding: from initial evaluation up to gastrointestinal endoscopy. Med Clin North Am 92(3): 491-509.
-
Rockall TA, Logan RF, Devlin HB, Northfield TC (1996) Risk assessment after acute upper gastrointestinal haemorrhage. Gut 38(3): 316-321.
-
Blatchford O, Murray WR, Blatchford M (2000) A risk score to predict need for treatment for upper- gastrointestinal haemorrhage. Lancet 356(9238): 1318- 1321.
-
Saltzman JR, Tabak YP, Hyett BH, Sun X, Travis AC, et al. (2011) A simple risk score accurately predicts in- hospital mortality, length of stay, and cost in acute upper GI bleeding. Gastrointest Endosc 74(6): 1215-1224.
-
Nakamura S, Matsumoto T, Sugimori H, Esaki M, Kitazono T, et al. (2014) Emergency endoscopy for acute gastrointestinal bleeding: prognostic value of endoscopic hemostasis and the AIMS65 score in Japanese patients. Dig Endosc 26(3): 369-376.
-
Hyett BH, Abougergi MS, Charpentier JP, Kumar NL, Brozovic S, et al. (2013) The AIMS65 score compared with the Glasgow-Blatchford score in predicting outcomes in upper GI bleeding. Gastrointest Endosc 77(4): 551-557.
-
Thandassery RB, Sharma M, John AK, Al-Ejji KM, Wani H, et al. (2015) Clinical Application of AIMS65 Scores to Predict Outcomes in Patients with Upper Gastrointestinal Hemorrhage. Clin Endosc 48(5): 380-384.
-
Abougergi MS, Charpentier JP, Bethea E, Rupawala A, Kheder J, et al. (2016) A Prospective, Multicenter Study of the AIMS65 Score Compared With the Glasgow- Blatchford Score in Predicting Upper Gastrointestinal Hemorrhage Outcomes. J Clin Gastroenterol 50(6): 464- 469.
-
Iino C, Mikami T, Igarashi T, Aihara T, Ishii K, et al. (2016) Evaluation of scoring models for identifying the need for therapeutic intervention of upper gastrointestinal bleeding: A new prediction score model for Japanese patients. Dig Endosc 28(7): 714-721.
-
Tammaro L, Buda A, Di Paolo MC, Zullo A, Hassan C, et al. (2014) A simplified clinical risk score predicts the need for early endoscopy in non-variceal upper gastrointestinal bleeding. Dig Liver Dis 46(9): 783-787.
-
Saeed ZA, Winchester CB, Michaletz PA, Woods KL, Graham DY (1993) A scoring system to predict rebleeding after endoscopic therapy of nonvariceal upper gastrointestinal hemorrhage, with a comparison of heat probe and ethanol injection. Am J Gastroenterol 88(11): 1842-1829.
-
Hay JA, Maldonado L, Weingarten SR, Ellrodt AG (1997) Prospective evaluation of a clinical guideline recommending hospital length of stay in upper gastrointestinal tract hemorrhage. Jama 278(24): 2151- 2156.
-
Camellini L, Merighi A, Pagnini C, Azzolini F, Guazzetti S, et al. (2004) Comparison of three different risk scoring systems in non-variceal upper gastrointestinal bleeding. Dig Liver Dis 36(4): 271-277.
-
Almela P, Benages A, Peiró S, Añón R, Pérez MM, et al. (2004) A risk score system for identification of patients with upper-GI bleeding suitable for outpatient management. Gastrointest Endosc 59(7): 772-781.
-
Marmo R, Koch M, Cipolletta L, Capurso L, Grossi E, et al. (2010) Predicting mortality in non-variceal upper gastrointestinal bleeders: validation of the Italian PNED Score and Prospective Comparison with the Rockall Score. Am J Gastroenterol 105(6): 1284-1291.
-
Laursen SB, Oakland K, Laine L, Bieber V, Marmo R, et al. (2021) ABC score: a new risk score that accurately predicts mortality in acute upper and lower gastrointestinal bleeding: an international multicentre study. Gut 70(4): 707-716.
-
Morarasu BC, Sorodoc V, Haisan A, Morarasu S, Bologa C, et al. (2023) Age, blood tests and comorbidities and AIMS65 risk scores outperform Glasgow-Blatchford and pre-endoscopic Rockall score in patients with upper gastrointestinal bleeding. World J Clin Cases 11(19): 4513-5430.
-
García-Iglesias P, Villoria A, Suarez D, Brullet E, Gallach M, et al. (2011) Meta-analysis: predictors of rebleeding after endoscopic treatment for bleeding peptic ulcer. Aliment Pharmacol Ther 34(8): 888-900.
-
Laine L, Barkun AN, Saltzman JR, Martel M, Leontiadis GI (2021) ACG Clinical Guideline: Upper Gastrointestinal and Ulcer Bleeding. Official journal of the American College of Gastroenterology ACG 116(5): 899-917.
-
Bozkurt S, Köse A, Arslan ED, Erdoğan S, Üçbilek E, et al. (2015) Validity of modified early warning, Glasgow Blatchford, and pre-endoscopic Rockall scores in predicting prognosis of patients presenting to emergency department with upper gastrointestinal bleeding. Scand J Trauma Resusc Emerg Med 23: 109.
-
Barkun AN, Bardou M, Kuipers EJ, Sung J, Hunt RH, et al. (2010) International consensus recommendations on the management of patients with nonvariceal upper gastrointestinal bleeding. Ann Intern Med 152(2): 101- 113.
-
Park SM, Yeum SC, Kim BW, Kim JS, Kim JH, et al. (2016) Comparison of AIMS65 Score and Other Scoring Systems for Predicting Clinical Outcomes in Koreans with Nonvariceal Upper Gastrointestinal Bleeding. Gut Liver 10(4): 526-531.
-
Sakong H, Moon HS, Choi SW, Kang SH, Sung JK, et al. (2022) ABC score is an effective predictor of outcomes in peptic ulcer bleeding. Medicine (Baltimore) 101(49): e31541.
- Ramsay Hunt Syndrome Presenting as Gait Imbalance without Facial Paralysis: A Case Report
- Unveiling Hidden Culprits: An Observational Study of Upper Gastrointestinal Endoscopy Findings in Symptomatic Cholelithiasis Patients
- Assessing Health Care Providers’ Proficiency in International Patient Safety Goals: A Study to Assess the Knowledge &Practice on Patient Safety in a Tertiary Care Teaching Hospital in Gujarat
- Challenges in Diagnosing Child Language Disorders
- Stunting Service Management Model in the South-Central Timor Region, East Nusa Tenggara, Indonesia
- Acute Small Bowel Obstruction Presenting as Gangrenous Jejunal Loop Secondary to Intestinal Endometriosis – A Rare Case Report