Microbiological Epidemiology at Chris Hani Baragwanath Academic Hospital: Poly-Microbial Osteomyelitis Analysis
Background: The majority of the patients seen and treated at our clinical setting present during chronic osteomyelitis stage, which is anecdotally likely to be poly-microbial. Adults with poly-microbial infection have a predilection for gram-negative bacteria and anaerobes, a scenario that hypothetically leads to a higher morbidity of poly-microbial osteomyelitis following high-energy trauma. Our study looks into the epidemiology of poly-microbial osteomyelitis treated at our Tumour and Infection unit. Methods: This was a retrospective study of patients treated for osteomyelitis from 1st of June 2016 to 30th of May 2021. Medical records of eligible patients were retrieved for examination. Demographic data such as age, sex and race were recorded. Clinical presentation, and organisms cultured, including their anti-microbial sensitivities were documented. Results: There were 63 participants in the study. Thirty-one (49.21%) participants had mono-microbial osteomyelitis with 32 (50.79%) participants having poly-microbial osteomyelitis. Majority of the poly-microbial patients presented with a draining sinus (68.75%) and most was located in the tibia (50%). Multiple mixed pathogens (both gram-positive and gram-negative) were cultured in combination in our patients and this comprised 71.21% of the total bacteria cultured. Staphylococcus Aureus was the commonest bacteria (30%) isolated, followed by Enterococcus faecalis (12%). The commonest gram-negative bacteriae cultured was Enterococcus cloacae (10%) followed by Acinetobacter baumannii at 7%. Most enterobacteriacae species were sensitive to Ertapenem and Ceftazidime. Conclusion: A slightly higher incidence of poly-microbial osteomyelitis was found in our study than that reported in literature. Furthermore, our study demonstrated a wide variety of organisms found in poly-microbial osteomyelitis, with a large contribution made by gram-negative anaerobic rod-shaped bacteria. Cephalosporins were not shown to be valuable as broad-spectrum cover drugs, and most bacteria cultured were found to be insensitive to them. What we suggest is tailoring antibiotics to the specific cultured bacteria and sensitivity. Prompt management of patients with open fractures with early administration of intravenous antibiotics and adequate surgical management may lead to a reduction in the prevalence of chronic osteomyelitis.
Introduction
Osteomyelitis (OM) is an old age disease dating back to the times of Hippocrates [1]. The term is a fusion of two words osteo meaning “bone”, myelitis meaning “infection”. The disease is established following two clinical scenarios: (i) haematogenous spread and (ii) direct inoculation. In adults, 50% of cases are secondary to open fractures and surgery thereof, with the rest of the cases occurring due to haematogenous spread from a distant source [2]. A high volume of patients with open wounds and fractures from road traffic accidents (RTAs) as well as other trauma-related injuries are commonly seen in developing countries [3].
Kremers, et al. reported that OM demonstrated a predilection for males more than females, with more than 60% of cases accounted for by males [2]. These injuries are difficult to treat and subsequently leading to chronic infections in those cases [3].
The gold standard for diagnosing OM is positive microbiological cultures from deep bone tissue biopsy samples obtained during surgery [3]. This approach has demonstrated high sensitivity and specificity for making a causative diagnosis. Blood cultures have high sensitivity only in acute forms of osteomyelitis and are usually not useful in the diagnosis of chronic bone infections [3]. Bernard reported that surgical bone biopsy through the sinus tract had a sensitivity of 87%, a specificity of 79%, and a diagnostic accuracy of 82.5%. Bacteraemia occurred in nearly 20% of the patients presenting with bone infection [4]. Gram- positive organisms are the most commonly isolated bacteria in chronic OM, with Staphylococcus aureus (S. aureus) being the commonest bacteria isolated [3]. Gram-negative bacteria (GnB) are: (i) sharply increasing as reported in literature as causative agents in chronic OM, and (ii) usually drug- resistant e.g. extended broad-spectrum beta-lactam (ESBL) producing organisms. Therefore, GnB presents a challenge in the anti-microbial treatment/approach used [5]. Other studies have identified Methicillin-resistant Staphylococcus aureus (MRSA) as a growing threat for hospital and community acquired infections. In 2016, MRSA infections were reported to account for almost 40% of implant-related infections in the United States of America (USA) [3]. Locally, Mthethwa and Marais in their series reported a combination of Enterobacteriaceae species, followed by Staphylococcus, Pseudomona_s and _Enterococcus species in 45% of their cases of poly-microbial OM [1].
Successful surgical treatment in cases of poly-microbial OM requires aggressive and repeated surgical debridement; followed by a long course of intravenous antibiotics [6]. Anti- microbial therapies should be tailored to local sensitivity patterns and individual scenario. As a result, knowledge of institutional micro-organisms culture patterns is critical to successfully treat OM. In the South African context, we have an endemic problem of adult high-energy trauma with an overwhelming open fracture burden. On that basis, our study aimed to document and analyse the epidemiology of poly-microbial OM treated at our Tumour and Sepsis unit. Furthermore, our study seeked to propose antibiotic therapy relevant at our local clinical setting.
Objectives of the study were to: (i) document the incidence of poly-microbial OM, (ii) identify the commonest micro-organisms in poly-microbial OM and (iii) determine the antibiotic sensitivity profile in poly-microbial OM.
Methods
This was a retrospective study of patients treated for OM from 1st June 2016 to 30th May 2021. Medical records of 63 patients previously treated for OM at our Tumour and Sepsis unit, Chris Hani Baragwanath Academic Hospital (CHBAH) were retrieved for examination. Patient demographic data, i.e. age, race, gender and clinical aspects of the disease (site of infection, type of presentation and microbiological specimen from the national health laboratory services (NHLS)) for each case were documented. All data were entered onto a Microsoft excel spreadsheet by the principal investigator.
Inclusion Criteria
Patients 18 years of age and older Patients treated for poly-microbial osteomyelitis from 01 June 2016 ‒ 30 May 2021 Patients with complete laboratory results
Exclusion Criteria
Patients visiting for re-treatment of osteomyelitis Patients suffering from TB and fungal infections
Data Analysis
All data were imported to Stata version 17 for analysis. Categorical variables were analysed using frequencies and percentages. Bar, Pie and column graphical representations were used to describe the distribution of categorical variables. To determine the incidence of poly-microbial OM and mono-microbial OM patients; frequency distributions were used. The normality assumption for continuous data was done using the Shapiro-Wilk test. Continuous variables were analysed using median and interquartile range (IQR) since the data were non-normal and the study sample size being small. Box and whisker plots were used to describe the distribution of the continuous data. The commonest organism in poly-microbial OM was described using the frequency distribution. The anti-biogram sensitivity profile in poly-microbial OM was reported in a Table 1 using frequencies and percentages. Association between pathogen classification and body classification was done using cross- tabulations and a Fisher’s exact test was used to assess for the significant differences in the proportions. The level of significance was set at 5%.
Results
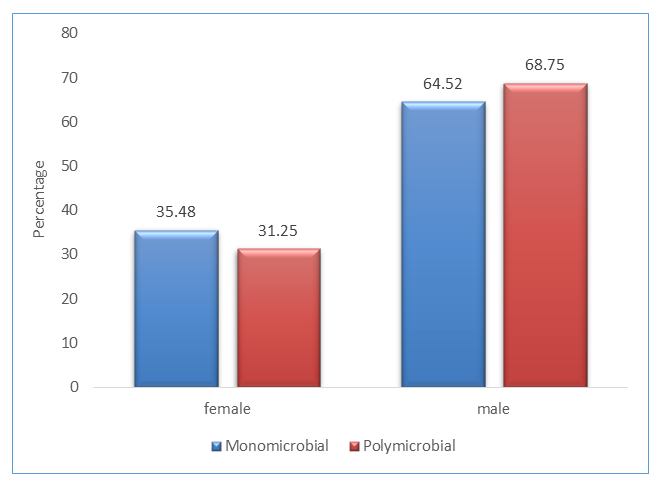
There were 63 participants recorded for our study duration and 31 (49.21%) had mono-microbial OM while 32 (50.79%) had poly-microbial OM. The majority of patients were males in both groups (n = 22, 68.75%) - poly-microbial; and (n = 20, 64.52%) - mono-microbial as shown in Figure 1.
The age distribution is shown in Figure 2. The median age for patients with poly-microbial OM was 36 years (IQR = 31.5 ‒ 56 years).
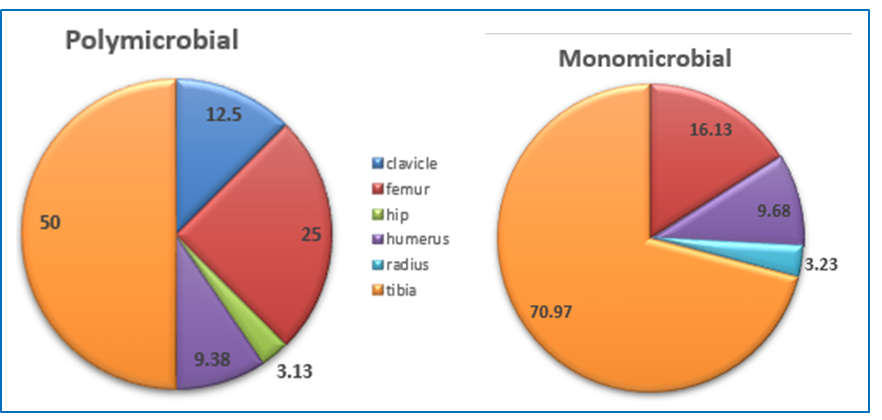
The bone type affected was also assessed and the results are shown in Figure 3. The most common bone affected was the tibia, which accounted for 50% in poly-microbial OM patients. The femur was the second bone of predilection.
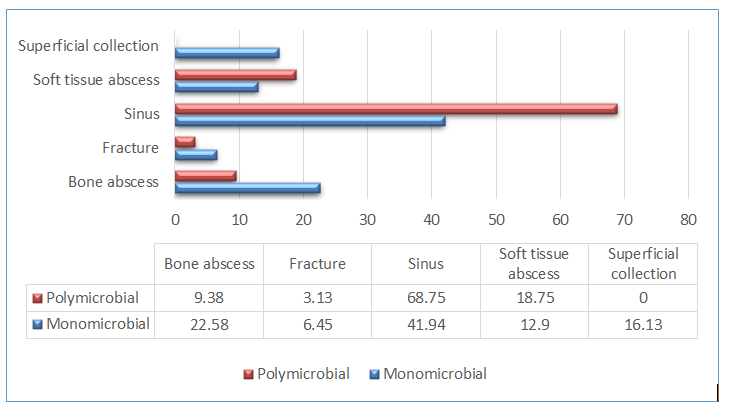
The type of presentation distribution between mono- microbial OM and poly-microbial OM groups is shown in Figure 4. Most patients had a sinus at presentation, 68.75% in the poly-microbial OM group and 41.94% in the mono- microbial OM group. Abscess formation was the second form of presentation, 22.58% of mono-microbial OM patients had a bone abscess while soft tissue abscess was the second mode of presentation in the poly-microbial OM group as it presented in 18.75% of the patients.
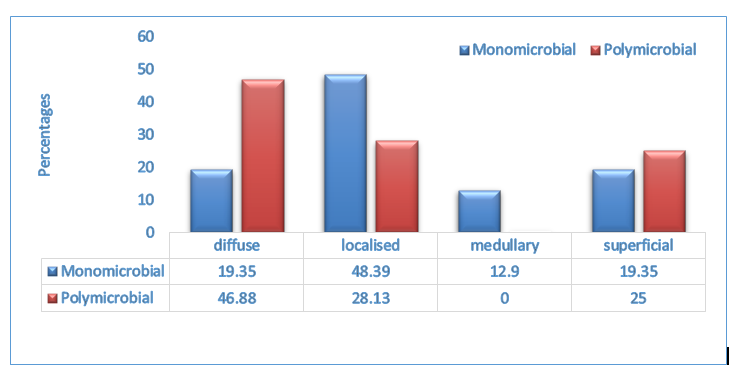
The classification distribution is shown in Figure 5. In the mono-microbial OM group, most people had a localised (48.39%) presentation while in the poly-microbial OM group, majority (46.88%) were classified as diffuse.
The number of pathogens isolated by individual frequency is shown in Figure 6. The poly-microbial OM group is defined as individuals with two or more micro- organisms isolated. Most of the poly-microbial OM patients had two pathogens (31.82%) isolated and 21.21% had four pathogens isolated individually.
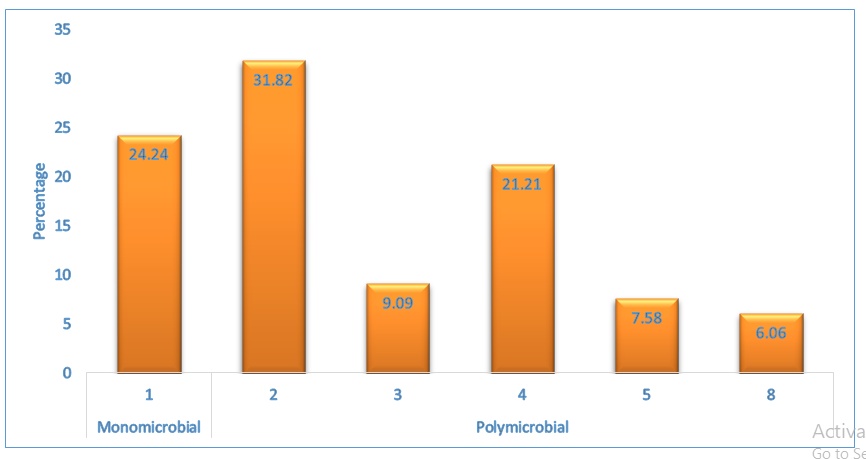
Table 1 shows the list of all the pathogens isolated and their frequency distribution in both the mono-microbial OM group and the poly-microbial OM group. The commonest pathogen was S. aureus identified in 28.79% of the patients followed by Enterococcus faecalis (E. faecalis) identified in 9.09% of the patients. Enterobacter cloacae (E. cloacae), Acinetobacter baumannii (A. baumannii), Proteus mirabilis (P. mirabilis) and Pseudomonas aeruginosa (P. aeruginosa) accounted for 7.58%, 6.82%, 6.82% and 5.3%, respectively. Pseudomonas aeruginosa (P. aeruginosa) accounted for 7.58%, 6.82%, 6.82% and 5.3%, respectively.
| Bacteria cultured | Mono-microbial n (%) | Poly-microbial n (%) | Frequency | Percentage (%) |
|---|---|---|---|---|
| Staphylococcus aureus (S. aureus) | 8(25.0) | 30(30.0) | 38 | 28.79 |
| Enterococcus faecalis (E. faecalis) | 12(12.0) | 12 | 9.09 | |
| Enterobacter cloacae (E. cloacae) | 4(12.5) | 10(10.0) | 10 | 7.58 |
| Acinetobacter baumannii (A. baumannii) | 2(6.625) | 7(7.0) | 9 | 6.82 |
| Proteus mirabilis (P. mirabilis) | 1(3.13) | 8(8.0) | 9 | 6.82 |
| Pseudomonas aeruginosa (P. aeruginosa) | 1(3.13) | 6(6.0) | 7 | 5.3 |
| Methicillin-resistant Staphylococcus aureus (MRSA) | 1(3.13) | 4(4.0) | 5 | 3.79 |
| Enterococcus faecium (E. faecium) | 3(9.38) | 2(2.0) | 5 | 3.79 |
| Eschericia coli (E. coli) | 1(3.13) | 3(3.0) | 4 | 3.03 |
| Bacillus species | 2 | 2(2.0) | 3 | 2.27 |
| Enterobacter species | 2 | 1(1.0) | 3 | 2.27 |
| Klebsiella species | ----- | 3(3.0) | 3 | 2.27 |
| Citrobacter freundii | 1(3.13) | 1(1.0) | 2 | 1.52 |
| Enterococcus gallinarum | ----- | 2(2.0) | 2 | 1.52 |
| Klebsiela pneumoniae | 1(3.13) | 1(1.0) | 2 | 1.52 |
| Proteus vulgaris | ----- | 2(2.0) | 2 | 1.52 |
| Serratia liquefaciens | 1(3.13) | 1(1.0) | 2 | 1.52 |
| Serratia marcescens | ----- | 2(2.0) | 2 | 1.52 |
| Anaerobic gram-negative bacillus (AGNB) | 1(3.13) | ----- | 1 | 0.76 |
| Bacteroides capillosus (BACTA) | 1(3.13) | ----- | 1 | 0.76 |
| Bacteroides eggerthii | ----- | 1(1.0) | 1 | 0.76 |
| Bacteroides fragilis | ----- | 1(1.0) | 1 | 0.76 |
| Citrobacter koseni | ----- | 1(1.0) | 1 | 0.76 |
| Clostridium clostridioforme | ----- | 1(1.0) | 1 | 0.76 |
| Clostridium perfringes | ----- | 1(1.0) | 1 | 0.76 |
| Klebsiella oxytoca | ----- | 1(1.0) | 1 | 0.76 |
| Staph haemolyticus | 1(3.13) | ----- | 1 | 0.76 |
| Streptococcus pyogenes | ----- | 1(1.0) | 1 | 0.76 |
| Streptococcus viridans | ----- | 1(1.0) | 1 | 0.76 |
| Yersinia enterocolitis | ----- | 1(1.0) | 1 | 0.76 |
Table 1: Anti-microbial sensitivity patterns for both mono-microbial and poly-microbial OM.
Table1: Bacteria cultured for mono-microbial and poly-microbial combined.
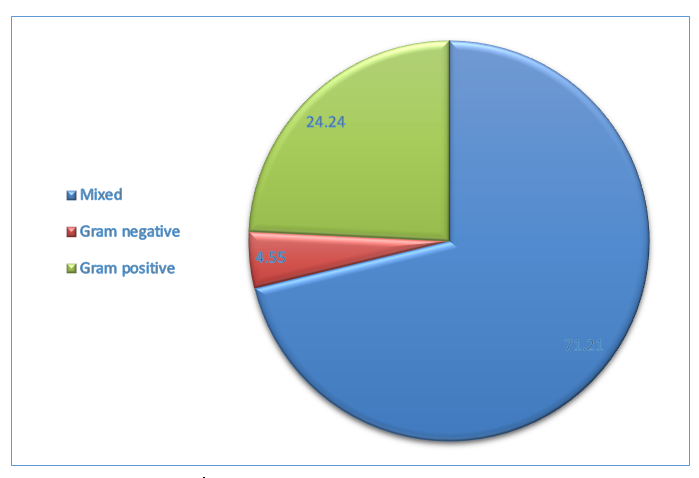
Figure 7 shows the pathogen classification. Most of the patients (n = 94, 71.21%) had mixed pathogens (gram- negative and gram-positive), (n = 32, 24.24%) had gram- positive pathogens and (n = 6, 4.5%) had gram-negative pathogens.
The anti-microbial sensitivity pattern for each of the pathogens is shown in Table 2.
| Pathogens Antibiotics | S. aureus | E.faecalis | E.cloacae | A. baumannii | P. mirabilis | P. aeruginosa | MRSA | E. faecium | E.coli | K.species |
|---|---|---|---|---|---|---|---|---|---|---|
| n = 38 | n = 12 | n = 10 | n = 9 | n = 9 | n = 7 | n = 5 | n = 5 | n = 4 | n = 3 | |
| n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | |
| Cloxacillin | 33(86.84) | 1(10) | 1(11.11) | 1(20.0) | ||||||
| Ampicillin | 2(5.26) | 11(91.67 | 1(20.0) | |||||||
| Azithromycin | 3(7.89) | |||||||||
| Clindamycin | 2(5.26) | |||||||||
| Erythromycin | 3(7.89) | |||||||||
| Ertapenem | 4(10.53) | 8(80) | 2(22.22) | 1(20.0) | ||||||
| Meropenem | 3(30) | |||||||||
| Imipenem | 5(50) | 2(22.22) | 1(33.33) | |||||||
| Vancomycin | 5(13.16) | 5(100) | 3(60.0) | |||||||
| Colistin | 6(66.67) | |||||||||
| Amoxicillin | 11(91.67) | 1(20.0) | ||||||||
| Piperacillin-Tazocata | 2(22.22) | 2(22.22) | 2(50.0) | 2(66.67) | ||||||
| Amoxicillin_Clavulanic acid | 1(8.33) | 4(44.44) | 2(50.0) | |||||||
| Cefepime | 2(20) | |||||||||
| Ciprofloxacin | 1(10) | 1(11.11) | ||||||||
| Ceftazidime | 1(11.11) | 5(71.43) | ||||||||
| Cefotaxime | ||||||||||
| Cefuroxime | 1(11.11) | |||||||||
| Gentamycin |
Table 2: Anti-microbial sensitivity patterns for both mono-microbial and poly-microbial OM.
S. aureus was variably sensitive to Ampicillin (n = 8, 21.05%), Cloxacillin (n = 6, 15.79%), Vancomycin (n = 7, 18.42%) and Amoxicillin (n = 7, 18.42%). E. faecalis was predominantly sensitive to Ertapenem (n = 4, 33.33%). E. cloacae were mostly sensitive to Cloxacillin (n = 5, 50%). A. baumannii was sensitive to Colisitn (n = 6, 66.67%). All MRSA pathogens were sensitive to Vancomycin (n = 5, 100%).
Table 3 shows the anti-microbial sensitivity pattern exclusively for poly-microbial OM. S. aureus was sensitive to Cloxacillin (n = 13, 72, 22%). E. faecalis was sensitive to Ampicillin (n = 9, 90%) with E. cloacae sensitive to Ertapenem (n = 8, 80%). P. Aeruginosa was sensitive to Ceftazidime (n = 4, 66.67%).
| Pathogens Antibiotics | S. | E. | E. | A. | P. | P. aeruginosa | MRSA | E. faecium | E. | K. |
|---|---|---|---|---|---|---|---|---|---|---|
| aureus | faecalis | cloacae | baumannii | mirabilis | coli | species | ||||
| n = 18 | n = 10 | n = 10 | n = 9 | n = 8 | n = 6 | n = 4 | n = 4 | n = 3 | n = 3 | |
| n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | |
| Cloxacillin | 13(72.22) | 1(10) | 1(11.11) | 1(25.0) | ||||||
| Ampicillin | 2(11.11) | 9(90) | 1(25.0) | |||||||
| Azithromycin | 2(11.11) | |||||||||
| Clindamycin | 1(5.56) | |||||||||
| Erythromycin | 1(5.56) | |||||||||
| Ertapenem | 1(5.56) | 8(80) | 2(25.0) | 1(25.0) | ||||||
| Meropenem | 3(30) | |||||||||
| Imipenem | 5(50) | 2(25.0)) | 1(33.33) | |||||||
| Vancomycin | 1(5.56)) | 2(50.0) | ||||||||
| Colistin | 6(66.67) | |||||||||
| Amoxicillin | 9(90) | 1(25.0) | ||||||||
| Piperacillin-Tazobactam | 2(22.22) | 1(12.5) | 2(50.0) | 2(66.67) | ||||||
| Amoxicillin-Clavulanic acid | 1(10.0)) | 2(25.0) | 2(50.0) | |||||||
| Cefepime | 2(20) | |||||||||
| Ciprofloxacin | 1(10) | 1(12.5) | ||||||||
| Ceftazidime | 1(11.11) | 4(66.67)) | ||||||||
| Cefotaxime | ||||||||||
| Cefuroxime | 1(12.5) | |||||||||
| Gentamycin |
Table 3: Anti-microbial sensitivity patterns for poly-microbial OM.
Table 4 shows the body classification and pathogens. Most of the pathogens were in the tibia. However, there was no association between pathogen classification and body classification, p-value > 0.05.
| Mixed n (%) | Gram-negative n (%) | Gram-positive n (%) | p-value | |
|---|---|---|---|---|
| Clavicle | 6(6.38) | 0 | 0 | 0.549 |
| femur | 24(25.53) | 2(33.3) | 6(18.75) | |
| hip | 5(5.32) | 0 | 0 | |
| humerus | 4(4.26) | 0 | 4(12.5) | |
| radius | 2(2.13) | 0 | 1(3.13) | |
| tibia | 53(56.38) | 4(66.67) | 21(65.63) |
Table 4: Bacterial pathogens in relation to body classification.
Discussion
Chronic OM is a complex infection due to its varied aetiology and associated factors. It needs to be approached in a multi-disciplinary manner. Because OM requires antibiotic therapy for prolonged periods, this poses a major financial burden; therefore, epidemiological studies on the bacterial and anti-microbial sensitivity profile are valuable in guiding healthcare policy developers on developing appropriate antibiotic guidelines.
Our study demonstrated that a majority of patients with infected with poly-microbial OM (50.79%) were males (68.75%), with a median age of 36 years. This is in agreement with what Khalid, et al. found in their study, where they reported 67.35% of patients out of 130 patients to be male [7]. The majority of our patients with poly- microbial OM were of African descent (87.5%). This reflects, demographically the population of Soweto, of which CHBAH is the main treating hospital.
The most common type of inoculation found in our study for mono-microbial OM was post-surgical (20.03%) following either tibial or femoral intramedullary nailing. For poly-microbial OM, surgery was only causal in 15.63% of that cohort. The above-statements cements trauma as the leading cause of chronic OM and theoretically poly-microbial OM. Neeharika, et al. in their study reported that 45% of their cases of chronic OM resulted from trauma [8]. Mthethwa and Marais reported mixed poly-microbial infections to be 16.7% resulting from post-traumatic aetiology [1]. This is similar to the findings of our study. The tibia bone was the commonest affected lower limb bone in our study, accounting for 50% of poly-microbial infected patients. The femur bone was secondarily affected, accounting for 25% of poly-microbial infected patients. Our results are consistent with those of Salman, et al. where 12% of their patients presented with lower limb infections [9]. Jorge, et al. in their study had 79.2% infections in the lower limbs [10].
The majority of poly-microbial infected patients in our study presented clinically with a draining sinus (68.75%). Kubwimana, et al. also discovered the hallmark clinical presentation to be a sinus discharging pus in 50 ‒ 93% of their patients [11]. Our findings are clear and consistent with these global findings. Mthethwa and Marais in their study, published results that revealed bacterial pathogens in relation to the physiological status of the host/patient, in accordance with the Cierny and Mader staging classification system for chronic OM, with the majority of their patients being host Type B [1]. Our study focused on the anatomical component of the classification system, and showed that the majority of our poly-microbial infected patients presented with diffuse chronic OM according to Cierny and Mader’s classification scheme (46.8%). This correlates to a type IV infection which has both medullary and cortical involvement [12]. The latter representing a severe spectrum component of the disease.
Sheehy, et al. in their series found S. aureus to be the most commonly isolated organism regardless of aetiology (32%), and their poly-microbial OM infections accounted for 29% of cases [13]. In our study, S. aureus was identified in 28.79% of patients as the commonest organism, and in agreement with Sheehy, et al. [13]. This was followed by E. faecalis at 9.04% and E. cloacae at 7.58%. The high prevalence of E. cloacae in 10% of poly-microbial infected patients in our study group highlights the rise of gram-negative organisms in poly- microbial OM already highlighted in the literature [14].
Peng, et al. reported on the proportion and cases of gram-positive (53.85%) and gram-negative bacteria at 46.15% in their 84 patient study [15]. In our study, 24.24% of our patients cultured gram-positive organisms and 4.55% patients cultured gram-negative organisms. A high proportion of our patients cultured a mixed pathogen pattern at 71.21%. This is significantly higher than previously reported in both local and international literature. The latter can possibly be explained by the delays our patients experience before they are taken to theatre for their initial debridement post- injury. This coupled with the significant burden of open fractures in our context has serious implications on chronic OM and subsequently the poly-microbial type. Jorge, et al. [10] reported an increased number of post-traumatic poly- microbial infections in Gustilo-Andersen grade 3 type open fractures [7]. Kindsfater, et al. [16] infections in 7% of their grade 2 and 3 open fracture patients debrided in < 5 hours, a percentage that rose to 38% for patients debrided ≥ 5 hours’ post-injury [16]. This correlates well with our findings and it possibly explains our high number of mixed pathogen poly- microbial infections.
The commonest gram-positive organism cultured in our poly-microbial group was S. aureus at 30%, followed by E. faecalis at 12%. MRSA although dreaded was present in 4% of cases with E. faecium accounting for only 2% of our cohort. Gram-negative bacteria cultured in the poly-microbial group were E. cloacae (10%), P. mirabilis (8%), A. baumannii (7%) and P. aeruginosa in 6% of cases. This reflects an increase in the number of gram-negative bacteria prevalence in poly- microbial infections consistent with international trends already highlighted earlier.
The micro-organisms cultured in our group displayed a broad range of sensitivities to antibiotics. The majority of S. aureus were sensitive to Cloxacillin (72.22%). Jones, et al. revealed 53% of S. aureus in their study being susceptible to Oxacillin [17]. This correlates well with our findings. S. aureus was also sensitive to Ampicillin, Azithromycin and Clindamycin in our study group. MRSA cultured (n = 5) was sensitive to Vancomycin in all our poly-microbial infected patients (100%). E. faecalis was sensitive to both Ampicillin and Amoxicillin (90%) and, Amoxicillin-Clavulanic acid in 10% of cases. Enterobacteriaceae species, E. cloacae and P. mirabilis were sensitive to Ertapenem, 80% and 25%, respectively. P. aeruginosa was mainly sensitive to Ceftazidime (66.67%) in our poly-microbial group.
A. baumannii was mostly sensitive to Colistin (66.67%) and Piperacillin-Tazobactam (22.22%). Mthethwa and Marais in 2017 found A. baumannii to be sensitive to Cloxacillin in 5 of 7 patients who cultured the bacteria.1The sensitivity differential displays the potential difficulty at our local setting when treating A. baumannii, with resistance to anti-microbials most likely due to geographical reasons. In future we can expand our study to explore the in-depth the resistance patterns that exist for organisms cultured. A further discussion around the impact of HIV on poly-microbial osteomyelitis in our context can further be explored, even though Mthethwa and Marais showed that HIV does not appear to alter the microbiology of chronic osteomyelitis, a different context may yield different outcomes.
Conclusion
The incidence of poly-microbial osteomyelitis in our study was found to be slightly higher than previously reported in other studies. In our study we had an incidence of 50.79% of poly-microbial OM, with a high incidence of mixed pathogens cultured (72.1%). The commonest micro-organisms in our poly-microbial OM group of patients were S. Aureus (30%). Our study found that, the majority of S. aureus were sensitive to Cloxacillin (72.22%) and A. baumannii was mostly sensitive to Colistin (66.67%) and Piperacillin-Tazobactam (22.22%). Moreover, the proportion of mono-microbial OM patients in our study was 49.1%. We recommend treating surgeons to be aware of the importance of instituting early debridement in minimising the occurrence of poly-microbial OM. A wide variety of anti-microbial sensitivities noted for the different pathogens will hopefully sensitize and depict the burden of treatment posed by poly-microbial OM, especially in a high trauma burden context.
Ethics statement
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Prior to the commencement of the study, ethical approval was obtained from the Human Research Ethics Committee (Medical) of University of the University with reference number: M210842.
Declaration
I Tiego Josiah Hlapolosa declare that this research report in the format of a “submissible” paper is my own, unaided work. It is being submitted for the Degree of Master of Medicine in the division of Orthopaedic Surgery at the University of the Witwatersrand, Johannesburg. It has not been submitted before for any degree or examination at any other University.
The authors declare authorship of this article and that they have followed sound scientific research practice. This research is original and does not transgress plagiarism policies.
Dedication
To my wife and son, I wouldn’t be where I am without the support structure and love that you continuously provide to me. Thank you.
In memory of my parents Mbuti Andries & Leah Koko Hlapolosa
Presentations and publications arising from the research project
South African Orthopaedic Association Annual Congress-
Cape Town September 2023
Author Contributions
JTH: Study Conceptualisation, Data Capture, Data Analysis, Manuscript Preparation, Revision And Approval of Final Manuscript. PMK: Study Conceptualisation, Manuscript Revision and Approval of Final Manuscript. MJ: Study Conceptualisation, Manuscript Revision and Approval of Final Manuscript.
Acknowledgements
I would like to pay tribute to my mentor and primary supervisor Dr Paul Kgagudi for all the support and guidance throughout this challenging journey. I would also like to pay credit to Dr Maxwell Jingo for all the expert guidance and direction from inception until the completion of this research report.
References
-
Mthethwa PG, Marais LC (2017) The microbiology of chronic osteomyelitis in a developing world setting. South African Orthopaedic Journal 16(2): 39-45.
-
Kremers HM, Mceuly EN, Jeanin E (2015) Trends in the epidemiology of osteomyelitis: a population-based study, 1969 to 2009.The Journal of Bone and Joint surgery (America) 97: 837-845.
-
Fantoni M, Taccari F, Giovanneze F (2019) Systemic antibiotic treatment of chronic osteomyelitis in adults. European review for Medical and Pharmacological Sciences 23(S2): 258-270.
-
Glaudemans AW, Jutte PC, Cataldo MA (2019) Consensus document for the diagnosis of peripheral bone infection in adults: a joint paper by the EANM, EBJIS, and ESR (with ESCMID endorsement). European Journal of Nuclear Medicine and Molecular Imaging 46(4): 957-970.
-
Kavanagh N, Ryan EJ, Widaa A (2018) staphylococcal osteomyelitis: disease progression, treatment challenges, and future directions. Clinical Microbiology Reviews 31(2): e00084-17.
-
Clerc A, Zeller V, Marmor S (2020) Haematogenous osteomyelitis in childhood can relapse many years later into adulthood: a retrospective multicentric cohort study in France. Medicine 99(20): e196197.
-
Khalid, Ihsanullah, Inam M, Shabir M (2020) Frequency of Different Bacteria and their antibiotic sensitivity pattern in chronic osteomyelitis. Journal of Pakistan Orthopaedic Association 32(2): 92-96.
-
Neeharika B, Virod R, Rakesh G (2019) A study of aerobic bacterial profile and their antibiogram in patients with chronic osteomyelitis with specific references to Staphylococcus aureus. Indian Journal of Microbiology Research 6(4): 350-354.
-
Salman AA, Hussein E, Yonis A (2008) Epidemiological and bacteriological study of chronic osteomyelitis. Tikrit Medical Journal 14(10): 59-62.
-
Jorge LS, Fucuta PS, Oliveira MGL (2018) Outcomes and risk factors for polymicrobial posttraumatic osteomyelitis. Journal of Bone and Joint Infection 3(1): 20-26.
-
Kubwimana O, Uwizeyimana E, Lynn L (2019) Chronic osteomyelitis in Sub- Saharan Africa. A Review-Global Surgery 5: 1-5.
-
Marais LC, Ferreira N, Aldous C (2014) The classification of chronic osteomyelitis. South African Orthopaedic Journal 13(1): 22-28.
-
Sheehy SH, Atkins BA, Bejon P (2010) The microbiology of chronic osteomyelitis: Prevalence of resistance to common empirical anti-microbial regiments. Journal of Infections 60: 338-343.
-
Moriarty FT, Kuehl R, Coenye T (2016) Orthopaedic device-related infection: Current and further interventions for improved prevention and treatment. EFORT Open Review 1(4): 89-99.
-
Peng J, Ren Y, Wenbin H (2017) Epidemiological, clinical and microbiological characteristics of patients with post- traumatic osteomyelitis of limb fractures in Southwest China: A Hospital-Based study. Journal of Bone and Joint Infection 2(3): 149-153.
-
Kindsfater K, Jonassen EA (1995) Osteomyelitis in Grade 2 and 3 open fractures with late debridement. Journal of Orthopaedic Trauma 9(2): 121-127.
-
Jones ME, Karlowsky JA, Draghi DC (2004) Antibiotic susceptibility of bacteria most commonly isolated from bone related infections: The role of cephalosporins in antimicrobial therapy. International Journal of Antimicrobial Agents 23(3): 240-246.
- Ramsay Hunt Syndrome Presenting as Gait Imbalance without Facial Paralysis: A Case Report
- Unveiling Hidden Culprits: An Observational Study of Upper Gastrointestinal Endoscopy Findings in Symptomatic Cholelithiasis Patients
- Assessing Health Care Providers’ Proficiency in International Patient Safety Goals: A Study to Assess the Knowledge &Practice on Patient Safety in a Tertiary Care Teaching Hospital in Gujarat
- Challenges in Diagnosing Child Language Disorders
- Stunting Service Management Model in the South-Central Timor Region, East Nusa Tenggara, Indonesia
- Acute Small Bowel Obstruction Presenting as Gangrenous Jejunal Loop Secondary to Intestinal Endometriosis – A Rare Case Report