Myelolipoma: A Rare Case Presentation and Review
Background: Myelolipomas are rare, benign tumors composed of mature adipose tissue and hematopoietic elements, primarily encountered in the adrenal glands. However, their occurrence in other locations is exceptionally rare. Case report: We present our case of a 63-year-old male, presented with a sub xiphoid myelolipoma. This mass was incidentally discovered during imaging, with the patient reporting no associated pain or symptoms. Imaging studies were concerning for neoplastic etiology like liposarcoma. An interventional radiology (IR) biopsy revealed "unremarkable bone marrow." Subsequent resection confirmed the diagnosis of myelolipoma. Conclusion: The myelolipoma in this unusual location highlights the importance of considering tumor atypical locations in the differential diagnosis when evaluating patients with uncommon mass presentations
Introduction
Myelolipomas are typically benign tumors consisting of a combination of mature adipose tissue and hematopoietic elements, primarily encountered in the adrenal glands, representing around 3% of adrenal incidentalomas [1]. First described in 1905 by Gierke [2], these tumors were later coined “myelolipomas” by Oberling in 1929 due to their dual composition. They are generally asymptomatic and are often discovered incidentally during imaging studies for unrelated conditions. However, myelolipomas occurring in unusual locations outside the adrenal glands are exceedingly rare. These tumors have been described in various locations, including the liver, retroperitoneum, and pelvis [3]. We present a case report of a myelolipoma located sub xiphoid, a location seldom associated with this tumor, and discuss the characteristics and management of extra-adrenal myelolipomas.
The patient is a 63-year-old Caucasian male with a history of diabetes mellitus (DM), hypertension (HTN), chronic kidney disease (CKD), and coronary artery disease (CAD), presented for a regular check-up. He had been asymptomatic and reported no abdominal pain, discomfort, or other symptoms related to the abdomen or subxiphoid region. The sub-xiphoid mass was incidentally discovered during a routine echocardiographic examination. The echocardiogram described a “large echo-dense structure” in the subxiphoid area. This unexpected finding prompted further evaluation to determine the nature and origin of the mass. Subsequent chest magnetic resonance imaging (MRI) revealed a lobulated, heterogeneous, and encapsulated mass posterior to the xiphoid process. The mass measured up to 11 cm in size and exerted a mass effect on the left hepatic lobe, displacing it posteriorly. Notably, the mass was abutting and adherent to the liver capsule without definitive evidence of liver capsular invasion. MRI further characterized the mass as containing fat and soft tissue components with no significant enhancement. These radiological features were concerning for a neoplastic etiology, particularly liposarcoma. An IR biopsy of the subxiphoid mass was performed to establish a definitive diagnosis and guide further management. Surprisingly, the biopsy results showed “unremarkable bone marrow,” a finding that did not provide a precise diagnosis and introduced additional complexity to the case. Ultimately, surgical resection of the specimen was deemed necessary. During the operation, it was observed that the mass was well-encapsulated and did not invade any intra-abdominal organs. However, it was intimately associated with the sternum and xiphoid process. Subsequent pathology analysis of the resected specimen yielded an unexpected diagnosis of myelolipoma.
Case Discussion
Extra-adrenal myelolipomas have been reported in various locations, often causing diagnostic challenges due to their rarity and diverse clinical presentations. Here, we summarize key findings from the existing literature on extra- adrenal myelolipomas.
Clinical Presentation
Extra-adrenal myelolipomas typically present as painless masses, with symptoms depending on their size and location. Retroperitoneal myelolipomas may cause abdominal discomfort or pain due to the mass effect [4]. Presacral myelolipomas can lead to lower back pain, constipation, or urinary symptoms. Pelvic myelolipomas may result in pelvic pain, urinary symptoms, or discomfort. Thoracic myelolipomas are exceedingly rare and can cause chest pain, cough, or respiratory issues. Although some patients may experience discomfort or pain, many remain asymptomatic [5]. Radiological Features Imaging studies like CT and MRI are crucial in diagnosing myelolipomas. These tumors typically appear as well-defined, heterogeneous masses containing fatty and hematopoietic components. The presence of fat and hematopoietic elements often leads to characteristic imaging findings [6].
Histopathology and Differential Diagnosis
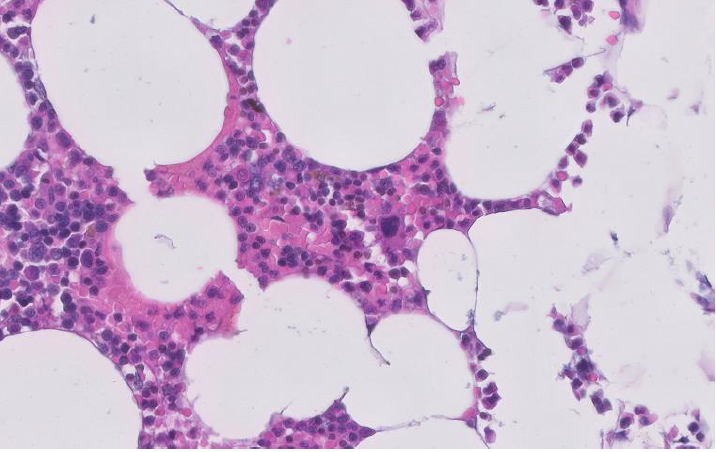
Histologically, myelolipomas consist of mature adipose tissue and hematopoietic elements Figure1, including myeloid and erythroid precursors. The presence of megakaryocytes is a distinctive feature [7]. The differential diagnosis of extra- adrenal myelolipomas includes liposarcoma, teratoma, and other fat-containing tumors. Histopathological examination is essential to confirm the diagnosis [8].
Management and Prognosis
Surgical resection is the mainstay of treatment for symptomatic or large myelolipomas. Asymptomatic, small tumors can be managed conservatively with regular monitoring [9]. Extra-adrenal myelolipomas are generally considered benign, and the prognosis after surgical resection is excellent. Recurrence is rare [10].
Conclusion
Myelolipomas are rare, benign tumors primarily found in the adrenal glands. However, their occurrence in extra- adrenal locations is exceptionally rare. We presented a case report of a myelolipoma located sub xiphoid, an unusual location for this tumor. Our literature review highlighted extra-adrenal myelolipomas’ diverse clinical presentations and radiological features. Although these tumors are typically benign, their rarity and potential for atypical locations emphasize the importance of considering uncommon tumor locations in the differential diagnosis when evaluating patients with unusual mass presentations.
References
-
Lam AK (2017) Update on Adrenal Tumours in 2017 World Health Organization (WHO) of Endocrine Tumours. Endocr Pathol 28(3): 213-227.
-
Gierke E (1905) Uber Knochenmarksgewebe in der Nebenniere. Beitr Pathol Anat 39(1): 533-537.
-
Yu HH, Lee YC, Liu KL (2014) Extraglandular retroperitoneal myelolipoma: a case report. J Med Case Rep 8: 199.
-
Lam KY, Lo CY (2001) Adrenal lipomatous tumours: a 30 year clinicopathological experience at a single institution. J Clin Pathol 54(9): 707-712.
-
Goldman HB, Daskivich TJ, Blaschko SD (2005) Management of a large, symptomatic, extraglandular adrenal myelolipoma: case report and review of the literature. Urology 66(4): 880.
-
Rao P, Kenney PJ, Wagner BJ, Davidson AJ (1997) Imaging and Pathologic Features of Myelolipoma. Radiographics 17(6): 1373-1385.
-
Yagci G, Yilmaz E, Yorukoglu K, Magi-Galluzzi C, Lopez JI (2006) Myelolipoma of the kidney: report of a rare entity. Int J Surg Pathol 14(3): 233-235.
-
Faria SC, Ikejiri ES, Marques EF (2005) Adrenal myelolipomas: CT and MRI findings. AJR Am J Roentgenol 185(2): 488-493.
-
Escudier B, Duvillard P, Droz JP (1991) Adrenal myelolipoma. J Urol 147(4): 1089-1090.
-
Singh R, Mittal A, Gupta S, Rana A (2017) Giant Extra- Adrenal Retroperitoneal Myelolipoma: A Rare Entity. J Clin Diagn Res11(8): Pd05-Pd06.
- Ramsay Hunt Syndrome Presenting as Gait Imbalance without Facial Paralysis: A Case Report
- Unveiling Hidden Culprits: An Observational Study of Upper Gastrointestinal Endoscopy Findings in Symptomatic Cholelithiasis Patients
- Assessing Health Care Providers’ Proficiency in International Patient Safety Goals: A Study to Assess the Knowledge &Practice on Patient Safety in a Tertiary Care Teaching Hospital in Gujarat
- Challenges in Diagnosing Child Language Disorders
- Stunting Service Management Model in the South-Central Timor Region, East Nusa Tenggara, Indonesia
- Acute Small Bowel Obstruction Presenting as Gangrenous Jejunal Loop Secondary to Intestinal Endometriosis – A Rare Case Report