Clinical Case Reports 1990 - 91
In this report, five different case scenarios were presented. In the first case, successful use of propranolol to relieve severe right ventricular infundibular obstruction was illustrated which facilitated balloon pulmonary valvuloplasty. In the second case, successful percutaneous occlusion of an atrial septal defect with buttoned device in an infant weighing 3.6 kg was documented. In the next case, rare association tricuspid atresia with persistent truncus arteriosus was recorded. The fourth case illustrates first successful transcatheter closure of patent ductus arteriosus with buttoned device in a child. The final case presents an unusual presentation of coarctation of the aorta in an infant and effective management with balloon angioplasty in the critically ill infant. Each of these cases were unique unto themselves either documenting successful management of these pathologies with innovative techniques or recording rare congenital cardiac abnormalities.
Introduction
A number of clinical cases have been observed and documented during the academic clinical practice of the author during a five-decade period. The cases documented from 1970 to 1989 were gone over in prior publications [1, 2, 3, 4, 5]. This article reviews cases seen in 1990 and 1991.
Use of Propranolol for Relief of Severe Infundibular Obstruction Prior to Balloon Pulmonary Valvuloplasty
Introduction: The prevalence of dynamic infundibular obstruction in association with severe pulmonary stenosis and balloon pulmonary valvuloplasty (BPV) was reviewed in a prior publication [6]. Inability to advance the catheter across the right ventricular (RV) infundibulum to undertake BPV was encountered which will be described by Thapar, et al. [7].
tricuspid regurgitation and right to left shunt across the atrial septum. At cardiac catheterization, the RV systolic pressure was 195 mmHg. RV cineangiogram demonstrated severe RV infundibular stenosis and thickened and domed pulmonary valve leaflets. Attempts to advance several types of catheters across the RV outflow tract were unsuccessful. At this point 0.5 mg of propranolol was slowly administered intravenously. Fifteen minutes after Propranolol, the RV pressure decreased to 168 mmHg and at this point a #6F balloon wedge catheter could be adavance across the RV infundubulum and pulmonary valve into the pulmonary artery. Then BPV was performed by using 18 mm balloon valuloplasty catheter. The residual gradients across the RV infundubulum and pulmonary vlave were 40 and 30 mmHg, respectively. The patient was prescribed 10 mg of Propranolol three times a day for three months. A repeat echo-Doppler study six months after BPV revealed 20 mmHg gradient across the pulmonary valve and no RV infundibular gradient.
any catheter into the pulmonary artery. Administration of 0.5 mg of Propranolol intravenously resulted in reduction of the obstruction which allowed passage of catheters and BPV could be performed without complication. Following the procedure oral Propranolol treatment was initiated which helped to resolve the infundibular obstruction during follow- up. We have therefore recommended the use of Propranolol in patients with severe RV infundibular obstruction so that BPV can be performed as described by Thapar, et al. [7].
In response to our paper on RV infundibular obstruction [6], Pearl and Wilkins, in a letter to the editor [8], described their experience with BPV in an 18-year old male; they were able to reduce the gradient across the pulmonary valve, but RV infundibular obstruction developed which was addressed by surgical resection of RV infundibulum. In a reply to this letter [9], we have discussed the role of beta-blocker therapy, indicated that post-BPV RV infundibular obstruction can be managed with beta-blocker medications without resorting to surgery, and detailed step by step description of the management of infundibular stenosis associated with pulmonary stenosis and BPV [9]. This is listed in Table 1 for the interested reader.
- Discussion: This particular case describes a 10-year-old girl with severe pulmonary valvar stenosis with associated RV infundibular obstruction. This infundibular obstruction was very severe and consequently we were unable to advance
- 1. Consider the possibility of development of infundibular obstruction after BPV in all patients with severe valvar PS
- 2. Perform careful pressure pullback recordings across the pulmonic valve and RV outflow tract both prior to and 15 minutes after BPV
- 3. Perform RV cine-angiography and scrutinize these angiograms for infundibular obstruction both before and 15 minutes after valvuloplasty
- 4. Use a valvuloplasty balloon that will result in a B/A ratio of 1.2 to 1.25
- 5. Use a double-balloon technique when the pulmonary valve annulus is too large to dilate with a commercially available single balloon. When a double balloon technique is used, the effective diameter of both balloons together should be used for calculation of the B/A ratio. Effective balloon diameter may be calculated by the formula: 0.82(D1+D2)
- 6. If pulmonary valve dysplasia is present, a B/A ratio as high as 1.5 may be necessary for effective relief of pulmonary valve obstruction
- 7. Balloons larger than 1.5 times the size of the pulmonary valve annulus should not be used because such large balloons may damage the right ventricular outflow tract muscle. In addition, balloons more than 1.5 times the size of the pulmonary valve annulus did not produce better immediate or intermediate-term results when compared with the subgroup in whom a B/A ratio of 1.2 to 1.4 was achieved during balloon valvuloplasty and the extra-large balloons may precipitate an infundibular reaction
- 8. If angiographic, pressure and/or echo-Doppler data suggest, significant residual infundibular obstruction, beta blocker drug therapy may be necessary; we recommend it if the residual gradient is more than 50 mmHg
- 9. If results of follow-up echo-Doppler or catheterization and angiographic studies performed 6 months to 1 year after balloon valvuloplasty show residual infundibular gradients ≥50 mm Hg, then surgical resection of the infundibular muscle may be considered. If there is significant residual valvar obstruction, repeat BPV with adequately sized balloon(s) would be our therapeutic choice
Table 1: Management of Infundibular Obstruction.
BA, balloon/annulus; BPV, balloon pulmonary valvuloplasty; D1, diameter of the first balloon; D2, diameter of the second balloon; PS, pulmonary stenosis; RV, right ventricle. Modified from Rao PS, et al. [9].
Successful Catheter Closure of an Atrial Septal Defect in a 3.6 Kg Infant
Introduction: In the first report on the buttoned device that we published by Rao PS, et al. [10], we documented the successful closure of an ASD with the buttoned device in an infant weighing 3.6 kg. This report documents this case.
Case Report: This female infant was a product of 32 weeks’ gestation, born to a 24.year-old gravida II, para I diabetic mother by cesarean section because of abruptio placenta. The infant weighed 2,270 gm at birth. She developed severe respiratory distress syndrome (hyaline membrane disease) and had to be intubated within hours after birth. On the twelfth day of life, surgical ligation of a patent ductus arteriosus was performed at another institution because of increasing need for respiratory support in the presence of echo-Doppler evidence for significant-sized patent ductus arteriosus. Indomethacin was not administered because of signs of renal insufficiency. The infant was weaned off of respiratory support and was extubated at the age of 4 weeks. She was discharged home at 6 weeks of age; the discharge weight was 2,265 gm. A discharge chest roentgenogram showed prominent bronchopulmonary markings interpreted to be consistent with bronchopulmonary dysplasia, and she was discharged home on l/8 L/min of oxygen per nasal cannula. She was first evaluated by us at the age of 10 weeks. Clinical and echo-Doppler studies suggested a diagnosis of a moderate-sized atria1 septal defect and severe left pulmonary artery stenosis. Continuous flow disturbance was found in the right pulmonary vein with a peak Doppler flow velocity of 1.7 m/set and a diagnosis of right pulmonary vein stenosis was also considered. Cardiac catheterization and cine-angiographic studies were performed at the age of 5 months because of her failure to gain weight adequately (3.4 kg at 5 months), and because of continuing signs of congestive heart failure despite adequate anti-congestive measures. The findings at this study included a moderate left- to-right shunt across the atria1 septal defects (Qp:Qs = 1.5:1), moderate elevation of right ventricular/pulmonary artery peak pressures (mid-50s) with normal left ventricular peak pressures (mid-80s), no opacification of the left pulmonary artery, no evidence for right pulmonary vein stenosis, and a moderate-sized secundum atrial septal defect demonstrated by left atria1 angiography. Doppler flow disturbance in the right pulmonary vein was explained on the basis of torrential flow secondary to the return of all pulmonary blood flow via the right pulmonary vein. Because of continued difficulty in weight gain (3.6 kg at 7 months; only a 0.2 kg weight gain in 2 months) and moderate heart failure, it was decided that the atria1 septal defect (ASD) should be closed; a transcatheter method with a custom-made “buttoned” double-disk device [11] was selected.
The procedure was performed under a protocol for human use of these custom-made devices approved by our institutional Human Subjects Committee (Institutional Review Board). Informed consent was obtained from the parents. A cardiac surgery team was on standby as per the protocol. The device [11] consists of three components: an occluder, a counter-occluder, and a delivery system (Figure 1). The occluder is made of polyurethane foam covering a Teflon-coated wire skeleton. The wire skeleton is x-shaped when unfolded, and the wires are in nearly parallel position when folded and can be introduced into an 8F sheath. A 2 mm string loop is attached to the center of the occluder; the loop is closed by a 1 mm knot (“button”). The counter-occluder is made up of a rhomboid-shaped polyurethane foam mounted on a Teflon-coated wire skeleton. A rubber piece is sutured in its center and becomes a buttonhole. The delivery system consists of: (1) a loading wire, which is a Teflon-coated 0.028-inch guide wire (Cook Inc., Bloomington, Ind.); (2) a folded 0.005-inch nylon thread, the loop of which passes through the loop in the center of the occluder; (3) an 8F long sheath (Cordis Corp., Miami Lakes, Fla.); and (4) a 7F end- hole catheter (pusher) that is used to advance the occluder and counter-occluder within the sheath.
![Figure 1: Photograph of the original buttoned device. Reproduced from Rao PS [12].](/fulltextimages/12059/fig_1.png)
The infant was premeditated with a mixture of meperidine, and chlorpromazine, and no general anesthesia was used. Percutaneous right heart catheterization data were obtained in the usual manner and the data were similar to those obtained at the initial catheterization. Main pulmonary artery and left atria1 cine-angiograms were performed that reconfirmed the presence of an ASD. The right heart catheter was exchanged with 5F Edwards balloon septostomy catheter (Baxter Healthcare Corp., Edwards Division, Santa Ana, Calif.) and the stretched diameter of the ASD was measured by passing progressively larger balloons in a manner described by King et al [13]. The defect measured 10 mm;
it measured 7 mm on an echocardiographic study (Figure 2A). A 25 mm device was chosen for transcatheter closure. At this juncture, 360 units of heparin were administered, and a femoral arterial line to monitor the systemic pressure during the procedure was placed. The #6F sheath in the femoral vein was exchanged over a guide wire with a long #8F Cordis sheath with the help of an #8F catheter, and the tip of the sheath was positioned in the mid-left atrium. The occluder was delivered into the left atrium via the #8F sheath already in place. The counter-occluder was delivered into the right atrium. The occluder and the counter-occluder were buttoned across the ASD. The delivery system was disconnected from the device. A main pulmonary artery cine-angiogram was performed 15 minutes after device implantation. No residual left-to-right shunt across the atria1 septum was detected on the levophase of the cine- angiogram. Echo-Doppler studies to visualize the atria1 septal defect (Figure 2A) and to demonstrate flow across it were performed prior to and immediately after (Figure 2B) device implantation and were repeated 0.5, 3, and 6 months following the procedure. The device was intact (Figure 2C & Figure 2D) and showed no evidence for left-to-right shunt across the atria1 septum, either by pulsed or color Doppler evaluation at the time of follow-up studies. The device was also well visualized on a plain chest roentgenogram. The infant improved clinically and the anti-congestive measures were discontinued 1 month after device implantation.
![Figure 2: Selected subcostal four-chamber echocardiographic views of the atrial septum, showing a medium-sized atrial septal defect (arrow) prior to device closure (A), shortly after the device implantation (B), and 3 (C) and 6 (D) months following device implantation. The arrow in A shows the atrial septal defect. The large arrows in B, C, and D point to the occluder on the left atrial side and the small arrows in B and C show the counter-occluder end on. LA, Left atrium; RA, right atrium. Reproduced from Rao PS, et al. [10].](/fulltextimages/12059/fig_2.png)
Figure 2: Selected subcostal four-chamber echocardiographic views of the atrial septum, showing a medium-sized atrial septal defect (arrow) prior to device closure (A), shortly after the device implantation (B), and 3 (C) and 6 (D) months following device implantation. The arrow in A shows the atrial septal defect. The large arrows in B, C, and D point to the occluder on the left atrial side and the small arrows in B and C show the counter-occluder end on. LA, Left atrium; RA, right atrium. Reproduced from Rao PS, et al. [10].
Discussion: We documented the successful closure of an ASD with the buttoned device in an infant weighing 3.6 kg who had broncho-pulmonary dysplasia, an occluded left pulmonary artery, and congestive heart failure. Trans- catheter ASD closure devices used by King, Rashkind, and Lock require #23, #16, and #1lF sheaths, respectively, for device delivery [10]. Because of the requirement of large size catheter delivery systems, these devices have not been used in small infants. Based on this experience, we suggested that the closure of ASDs with the buttoned device in small infants is feasible, safe, and effective, and recommended further clinical trials [10].
Tricuspid Atresia in Association with Persistent Truncus arteriosus
Introduction: We reported the clinical, echo-Doppler, and pathologic information of a rare case of tricuspid atresia with Truncus arteriosus (Type IV) [14, 15]. These findings will be presented.
Case Report: A female infant weighing 2.8 kg was born following an emergency cesarean section; this baby had poor Apgar scores and required ventilatory support at birth. An ECG showed right atrial enlargement, left axis deviation, and no anterior and rightward QRS voltages. Echo-Doppler studies showed an atretic tricuspid valve, an atrial septal defect, and a large sub-arterial VSD (Figure 3a & Figure b, Figure 4a & Figure 4b). The left ventricle was close to normal in size but the right ventricle was small (Figure 3a & Figure 4a). One great vessel (truncus) arose from the heart, overriding the VSD (Figure 3b, Figure 3c & Figure 4b). The pulmonary artery appeared to arise from the posterolateral aspect of the truncus (Figure 3d & Figure 4c) and divided into right and left branches shortly after its origin (Figure 4d). The truncal valve leaflets appeared thickened with a Doppler flow velocity of 2 m/s, suggesting mild truncal valve stenosis. Thus, the echo-Doppler data indicated tricuspid atresia with Truncus arteriosus and mild truncal valve stenosis. In spite of supportive measures including endotracheal ventilation, the infant’s condition deteriorated and she passed away 16 hours after being born. At autopsy, the right atrium was enlarged and the tricuspid valve was atretic, with a dimple in the floor of the right atrium – a finding typical for classic tricuspid atresia. A large atrial septal defect was seen. The left ventricle was large. A large sub-arterial VSD was visualized. The RV was small and hypoplastic (Figure 5a). A common arterial trunk arose from both the right and left ventricles. Three thickened dysplastic truncal valve leaflets were seen (Figure 5b). The pulmonary artery arose from the posterolateral aspect of the truncus one cm above the truncal valve and divided into right and left pulmonary artery branches which were diffusely narrow without discrete narrowing. These observations are suggestive of type I Truncus arteriosus. Thus, this was determined to be tricuspid atresia with Truncus arteriosus, classified as Type IV tricuspid atresia [16].
![Figure 3: Two-dimensional echocardiographic video frames demonstrating a. an atretic tricuspid valve (ATV) between the right atrium (RA) and right ventricle (RV), b. a large sub-truncal ventricular septal defect (VSD), c. thickened and somewhat domed truncal valve (TV) leaflets, and d. the origin of the pulmonary artery (PA) from the posterior aspect of the _truncus_ _arteriosus_ (TA). LA, left atrium; LV, left ventricle. Reproduced from Rao PS, et al. [14].](/fulltextimages/12059/fig_3.png)
Figure 3: Two-dimensional echocardiographic video frames demonstrating a. an atretic tricuspid valve (ATV) between the right atrium (RA) and right ventricle (RV), b. a large sub-truncal ventricular septal defect (VSD), c. thickened and somewhat domed truncal valve (TV) leaflets, and d. the origin of the pulmonary artery (PA) from the posterior aspect of the truncus arteriosus (TA). LA, left atrium; LV, left ventricle. Reproduced from Rao PS, et al. [14].
![Figure 4: Video frames from a two-dimensional echocardiographic and color Doppler study demonstrating a. an atretic tricuspid valve (ATV) between the right atrium (RA) and right ventricle (RV) and blood flow from the left atrium (LA) into the left ventricle (LV) across the mitral valve. The RV (arrow) is very small and hypoplastic. b. LV and RV with a large ventricular septal defect (VSD) below the Truncus arteriosus (TA). Turbulent flow across the truncal valve suggests truncal valve stenosis. c. the origin of the pulmonary artery (PA) from the TA by color flow (arrow), and d. the division of right (RPA) and left (LPA) pulmonary arteries from the PA (not labeled in d) in a short-axis view. TV, truncal valve leaflets. Reproduced from Rao PS, et al. [14].](/fulltextimages/12059/fig_4.jpeg)
Figure 4: Video frames from a two-dimensional echocardiographic and color Doppler study demonstrating a. an atretic tricuspid valve (ATV) between the right atrium (RA) and right ventricle (RV) and blood flow from the left atrium (LA) into the left ventricle (LV) across the mitral valve. The RV (arrow) is very small and hypoplastic. b. LV and RV with a large ventricular septal defect (VSD) below the Truncus arteriosus (TA). Turbulent flow across the truncal valve suggests truncal valve stenosis. c. the origin of the pulmonary artery (PA) from the TA by color flow (arrow), and d. the division of right (RPA) and left (LPA) pulmonary arteries from the PA (not labeled in d) in a short-axis view. TV, truncal valve leaflets. Reproduced from Rao PS, et al. [14].
Figure 5a: Photograph of heart and lung specimen of the cases described in figures 2 and 3, showing a large right atrium (RA), large left ventricle (LV) and a small right ventricle (RV). Only one vessel arises from the heart, namely the Truncus arteriosus (T). A pulmonary trunk (white arrowhead) was seen to arise from the posterolateral aspect of the T. The pulmonary trunk divides into the right and left pulmonary arteries, but is not shown in the photograph. b. Close-up photograph of the heart with the truncus arteriosus cut open. Thickened and dysplastic truncal valve leaflets (TVL) are shown. LAA, left atrial appendage. Reproduced from Rao PS, et al. [14].
Discussion: An extensive literature review was undertaken [14, 15] which revealed that there were six reported patients, including our patient, with tricuspid atresia along with Truncus arteriosus in whom pathologic and/or clinical descriptions were made. Six more cases were pointed out, but without a description of the particulars of each case. Based on these data, this anomaly (Type IV tricuspid atresia) has a prevalence of 1.4% of all tricuspid atresia cases. Most babies presented with cyanosis and/or congestive heart failure within a few days of birth to two months of age. Most of the babies died soon afterwards. Laboratory findings included cardiomegaly with increased pulmonary blood flow on the chest x-ray and left axis deviation with left ventricular hypertrophy on the ECG. When performed, the echocardiographic, catheterization, and selective angiographic studies were useful in confirming the pathophysiologic features of this anomaly. We concluded that the concomitant presence of tricuspid atresia and Truncus arteriosus is uncommon; clinical, ECG, echocardiographic, and pathologic characteristics are distinctive; and the presentation soon after birth with fast demise is usual. Consequently, we recommended that prompt surgical palliation should be instituted as recommended by RaoPS, et al. [14, 15].
First Successful Transcatheter Closure of Patent Ductus Arteriosus with Buttoned Device in a Child
Introduction: Following the successful use of the patent ductus arteriosus (PDA) buttoned device in animal models by Sideris and his colleagues [17], and good results with ASD buttoned device closure in human subjects [10, 18], the procedure was adopted to occlude PDA in human subjects [19]. Case Report: A 5 year-old boy, the product of a 24-week gestation, with a birth weight of 900 gm, who required ventilator support for the first 3 months of his life and a hospitalization of 5.5 months was referred to us for further care. A cardiac murmur was noted during the early hospital stay, which was subsequently thought to have disappeared. A cardiac murmur was re-discovered at age 3 years by his new pediatrician and he was referred to one of us for murmur evaluation, at which time a clinical diagnosis of small PDA was made. Recurrent episodes of pneumonia and wheezing, some requiring hospitalization, were noted, and were thought to be related to mild broncho pulmonary dysplasia. Physical examination at age 5 years revealed a grade II/VI continuous murmur heard best at the left upper sternal border, but otherwise normal cardiovascular findings. Chest x-ray revealed a normal-sized heart with normal pulmonary vascular markings. The lung fields were hyperinflated, consistent with his pulmonary disease. The ECG was normal. Echo-Doppler studies performed on the day before catheterization revealed that the diameters of the left atrium and left ventricle were at the upper limits of normal, with normal left ventricular shortening fraction. A small PDA was detected on color Doppler study (Figure 6A). Transcatheter closure was recommended, particularly in view of the child’s pulmonary disease. The procedure was performed under a protocol for human use of custom- made devices approved by our institutional Human Subjects Committee (Institutional Review Board). Informed consent was obtained from the parents. A cardiac surgery team was on standby, as directed by the protocol. After the patient was premeditated with a mixture of meperidine, promethazine, and chlorpromazine and 1% lidocaine infiltration in the right groin, percutaneous right, and left heart catheterization and cineangiography were performed. There was a small left-to- right shunt at the pulmonary artery level giving a pulmonary- to-systemic flow ratio of 1.4:1, and the right ventricular/ pulmonary artery peak systolic pressures were in the high 20s (mmHg). Angiography demonstrated a small patent ductus arteriosus (Figure 7A).
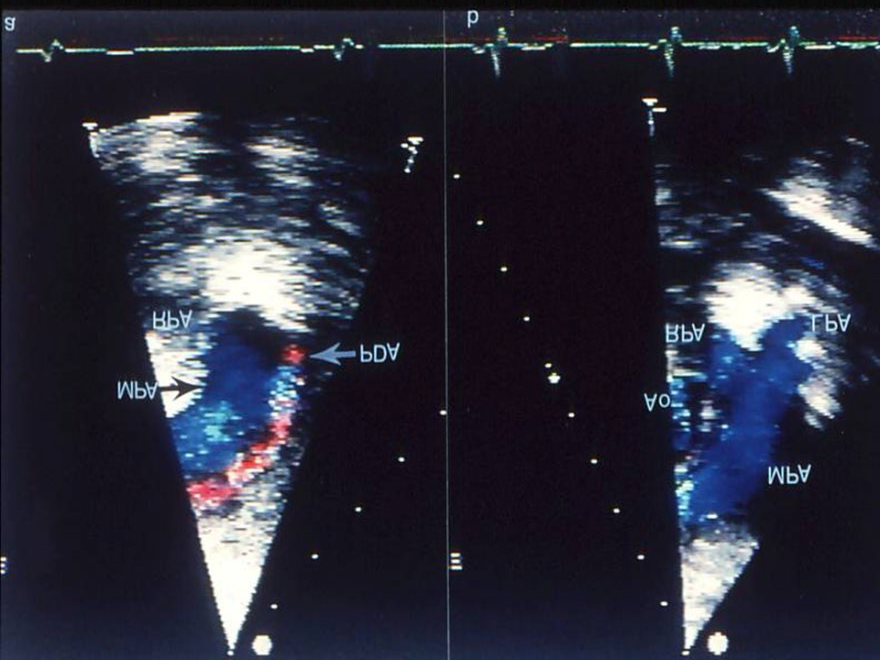
Figure 6: Selected video frames from two-dimensional and color Doppler echocardiographic parasternal short-axis views of the main pulmonary artery (MPA) prior to (a) and following (b) transcatheter buttoned device occlusion of a patent ductus arteriosus (PDA). Note the color flow disturbance indicating a small-to-moderate-sized PDA that is no longer seen in b following transcatheter closure. Forward (blue) flow in the MPA is seen. Also, there is no evidence for obstruction in the main, left (LPA) or right (RPA) pulmonary arteries. Ao, Aorta. Reproduced from Rao PS, et al. [19].
![Figure 6: Selected video frames from two-dimensional and color Doppler echocardiographic parasternal short-axis views of the main pulmonary artery (MPA) prior to (a) and following (b) transcatheter buttoned device occlusion of a patent ductus arteriosus (PDA). Note the color flow disturbance indicating a small-to-moderate-sized PDA that is no longer seen in b following transcatheter closure. Forward (blue) flow in the MPA is seen. Also, there is no evidence for obstruction in the main, left (LPA) or right (RPA) pulmonary arteries. Ao, Aorta. Reproduced from Rao PS, et al. [19].](/fulltextimages/12059/fig_6.png)
Figure 7: Selected frames from aortic arch (Ao) cine-angiograms in the lateral views, prior to (A) and 10 minutes after (B) transcatheter closure of a patent ductus arteriosus (PDA) with the buttoned device. The PDA (arrow) is clearly seen in A. An aortogram following occlusion (B) but before disconnecting the loading wire (LW) revealed no opacification of the ductus; ductal diverticulum (DD) is seen. DAo, Descending aorta; S, sheath used to deliver the device. Reproduced from Rao PS, et al. [19].
![Figure 7: Selected frames from aortic arch (Ao) cine-angiograms in the lateral views, prior to (A) and 10 minutes after (B) transcatheter closure of a patent ductus arteriosus (PDA) with the buttoned device. The PDA (arrow) is clearly seen in A. An aortogram following occlusion (B) but before disconnecting the loading wire (LW) revealed no opacification of the ductus; ductal diverticulum (DD) is seen. DAo, Descending aorta; S, sheath used to deliver the device. Reproduced from Rao PS, et al. [19].](/fulltextimages/12059/fig_7.png)
A 17 mm buttoned device was chosen for implantation. The device consists of three components: an occluder, a counter-occluder, and a delivery system (Figure 8). The occluder is made up of a rhomboid-shaped polyurethane foam covering a Teflon-coated wire skeleton and can easily be introduced into a 7F sheath. A 2 mm string loop is attached to the center of the occluder; the loop is closed by a 1 mm knot (“button”). The knot is marked with radiopaque material.
The counter-occluder is also made up of polyurethane foam mounted on a Teflon-coated wire skeleton. A rubber piece is sutured in its center and becomes a “buttonhole.” The delivery system consists of:
- a loading wire, which is a Teflon-coated 0.02%inch guide wire (Cook Inc., Bloomington, Ind.);
- a folded 0.005inch Trilene thread, the loop of which passes through the loop in the center of the occluder;
- a 7F long sheath (Cordis Corp., Miami Lakes, Fla.); and
- a 7F end-hole catheter (pusher) that is utilized to advance the occluder and the counter-occluder within the sheath.
A #5F multi-A2 catheter (Cordis Corp.) was introduced from the main pulmonary artery into the descending aorta via the PDA. Heparin, 1,900 units (100 units/kg), was given at this juncture. An 0.032-inch J guide wire was introduced into the descending aorta via the catheter already in place. The #5F catheter was replaced with a #7F catheter with a #7F long sheath (Cordis Corp.), and the tip of the sheath was positioned in the midthoracic aorta. The guide wire and catheter were removed and the sheath was flushed with saline. The occluder was loaded into the sheath and was advanced within the sheath with the help of a #7F (pusher) catheter, and the occluder was delivered into the descending aorta. The sheath and the occluder were slowly withdrawn so that the device occluded the PDA while the sheath was slowly withdrawn into the main pulmonary artery. Gentle traction on the wire connecting the occluder reveals that the occluder was in place and did not come through the PDA. The pusher catheter was removed and the counter-occluder was introduced over the wire but within the sheath and was advanced with the help of the pusher catheter and delivered into the main pulmonary artery. Buttoning, i.e., introducing the 1 mm knot of the occluder (“button”) through the rubber piece (“buttonhole”) of the counter-occluder, is performed by simultaneously (gently) pulling the occluder against the ductus while advancing the counter-occluder with the long sheath. Verification that the knot had been pulled through the buttonhole was obtained by fluoroscopy aided by the radiopaque marker on the knot. After buttoning, the loading wire was cut at the tip and withdrawn, leaving the Trilene strands holding the occluder. The device was disconnected by pulling one of the two Trilene strands. During the withdrawal of the loading wire and the Trilene thread, the sheath was gently pressed against the device to prevent application of excessive force on the device, thereby preventing inadvertent dislodgment of the device. The long sheath was removed and was replaced with a short regular sheath. No oxygen saturation data from the pulmonary artery were obtained in order to prevent inadvertent device dislodgement. An aortic arch cine-angiogram performed 10 minutes after device implantation but prior to disconnecting the loading wire (Figure 7B) via the catheter already in place revealed no residual shunt. The catheters and sheaths were removed. Cefazolin (50/mg/kg) was administered intravenously and was repeated at 6 and 12 hours following the procedure. Aspirin, 160 mg per day (5 to 10 mg/kg), was begun on the day following device placement and was continued for 3 months. Echo-Doppler studies were repeated on the day after and 2 weeks following transcatheter closure of PDA and did not reveal any residual shunt (Figure 6B). Discussion: The device used in this report can be delivered through a #7F size sheath, thus making it more suitable for younger and smaller children. Because of this and because of the simple mechanism of the device for implantation across the PDA, we have chosen this device to occlude the PDA in both children and adults with considerable success [21, 22, 23]. The device remained in position during the follow- up period and no residual shunt was documented by pulsed and color Doppler studies. We concluded that implantation of the “buttoned” double-disc device for occlusion of the PDA provides a feasible, effective, and safe method for this procedure [19]. Further clinical trials were recommended by Rao, et al. [19].
An Unusual Presentation of Coarctation of the Aorta in Infancy: Role of Balloon Angioplasty in the Critically Ill Infant
Introduction: An infant with aortic coarctation who presented with a severe degree of myocardial dysfunction similar to “cardiomyopathy” was successfully treated by balloon angioplasty, with restoration of normal left ventricular size and function. This case illustrates successful use of balloon angioplasty to address this problem [24]. Case Report: A 3-month-old boy was referred to us in March 1989 for evaluation of his failure to thrive and of symptoms suggestive of heart failure and cardiomegaly on a chest roentgenogram. Physical examination revealed a weight of 4.0 kg (below the fifth percentile), tachycardia, tachypnea, a loud third heart sound with a gallop, no audible murmur, hepatomegaly, and barely felt brachial and femoral pulses without any discernible brachio-femoral pulse delay. Blood pressure in the arm by palpation was 90 mm Hg and leg pressure was not recorded. Chest x-ray films revealed severe cardiomegaly (Figure 9A) and pulmonary venous congestion. ECG showed left ventricular hypertrophy with ST segment depression and a biphasic T wave in the left chest leads. An echocardiogram revealed a markedly enlarged left ventricle and a diminished left ventricular shortening fraction (Figure 10A & Table 2). Viral cultures and carnitine levels were drawn, and the results, which became available later, were normal. Anti-congestive measures including digitalis and diuretic therapy were started immediately after the above studies were obtained and afterload reduction with hydralazine [25] was started 2 days later. The infant improved with respect to the signs of heart failure.
![Figure 8: Cartoon of the adjustable buttoned device. A. button loop. B. components of the device: occluder (Occ), counter-occluder (COcc) and sheath (Sh). See text for a detailed description of the device components. Reproduced from Rao PS [20].](/fulltextimages/12059/fig_8.png)
![Figure 9: A. A chest x-ray in postero-anterior view at presentation, showing marked cardiomegaly and pulmonary venous congestion. B. A dramatic improvement of the cardiac size and pulmonary venous congestion on a chest x-ray obtained 12 months following balloon angioplasty. Reproduced from Saluhuddin, et al. [24].](/fulltextimages/12059/fig_9.png)
Figure 10: A. M-mode echocardiogram of the left ventricle (LV) at the time of initial presentation. A marked enlargement of the LV and poor LV function are shown. B. A similar echogram of the LV 12 months following balloon angioplasty shows remarkable improvement in LV size and function. ECG, Electrocardiogram; MV, mitral valve. Reproduced from Saluhuddin N, et al.[24]
| At Presentation | After CHF Treatment | Before BA | After BA | 1 mo | 2 mo | 4 mo | 6 mo | 12 mo | 15 mo (Cath)& | 18 mo | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Weight (Kg) | 4.1 | 4 | - | - | 4.3 | 5.3 | 6.1 | 7 | 8 | 8.8 | 10.4 |
| BP (mmHg) | 90 (systolic) | 140/80 | - | - | 121/ | 107/ | 120/ | 123/ | 106/ | 116/ | 116/ |
| 87 | 75 | 78 | 80 | 60 | 60 | 57 | |||||
| Coarctation gradient | - | 60* | 45* | 15* | 15* | 16* | 16* | 21* | 27* | 10# | 27* |
| LVDD (mm/%)@ | 42 (>90) | 39 (>90) | - | 37 | 35 (>90) | 32 (>90) | 29 (80) | 27 (70) | 27 (55) | - | 30 (60) |
| LV shortening fraction | 17 (%) | 18 (%) | - | 21 (%) | 22 (%) | 20 (%) | 38 (%) | 37 (%) | 41 | - | 39 |
| (%) | (%) |
Table 2: Clinical and echo-Doppler values prior to and following balloon angioplasty (BA) of’ aortic coarctation.
BP, blood pressure; CHF, congestive heart failure; LV, left ventricle; LVIDd, left ventricular internal dimension in diastole.
*Peak instantaneous gradient obtained by using a formula: gradient = 4 (V22 – V12)‘, where VI and V2 are Doppler flow velocities proximal and distal to aortic coarctation, respectively.
#Peak-to-peak systolic pressure gradient across aortic coarctation measured by pullback pressures during cardiac catheterization.
@Percentile standards are based on values published previously &Note difference between catheterization- measured gradient (10 mm Hg) 15 months following angioplasty and Doppler-measured gradients at 6, 12, and 18 months following angioplasty. Reproduced from Saluhuddin N, et al. [24].
Reexamination of the infant revealed well-felt brachial pulses with poorly felt femoral pulses, a right arm blood pressure of 140/80 mmHg, and a right lower extremity pressure of 86/54 mmHg. Repeat echo-Doppler studies revealed evidence for aortic coarctation with a descending aortic Doppler flow velocity of 4 m/sec, indicating an approximately 60 mmHg gradient across the coarctation. The left ventricle continued to be large with poor left ventricular function (Table 2). Because of poor left ventricular function and our past experience [26, 27], balloon angioplasty was recommended in preference to surgical treatment. Percutaneous right and left heart catheterization were performed under sedation and local xylocaine anesthesia. No abnormalities other than discrete aortic coarctation measuring 2.7 mm and mild-to-moderate isthmic hypoplasia were found. Peak-to-peak systolic pressure gradient across the coarctation was 45 mmHg. After heparinization, an 8 mm, low-profile balloon on a 5F catheter was chosen for balloon angioplasty. Three successive balloon inflations at 4, 5, and 6 atm of pressure, respectively, for a duration of 5 seconds each with a 5-minute-interval between each dilatation [26, 27] were then performed. Following angioplasty, the peak-to-peak gradient across the coarctation was reduced to 15 mm Hg and the coarctation segment increased to 6.0 mm. Digitalis, furosemide, and hydralazine (for reducing afterload) were continued and the infant was discharged home after he showed an adequate weight gain 1 week following angioplasty. Follow-up clinical, chest x-ray, and echo-Doppler studies were obtained periodically (Table 2), and these showed gradual but consistent improvement with normalization of cardiac size on chest x-ray examination (Figure 9B) and of left ventricular size and shortening fraction on echocardiogram (Figure 10B). Approximately 15 months following angioplasty a repeat cardiac catheterization was performed, which revealed a residual gradient of 10 mm Hg and continued angiographic improvement. No aneurysm was seen. The cardiac medications were gradually discontinued. The infant weighed 10.0 kg at 21 months of age (18 months following balloon angioplasty) and his blood pressure was 116/57 mm Hg. Three important aspects of this case are worthy of discussion: (1) the unusual appearance of “hypertensive cardiomyopathy” in an infant with aortic coarctation; (2) diagnosis at the time of presentation; and (3) the choice of therapy.
Cardiomyopathy: Cardiomyopathy. Although this infant’s condition may be best described as hypertensive cardiomyopathy, such a term may not be appropriate by generally accepted terminology. The term cardiomyopathy is reserved for cardiac muscle disease of unknown etiology. The condition under consideration is perhaps best described as hypertensive heart disease. The pathogenesis of a markedly enlarged left ventricle and left ventricular dysfunction seen in this infant may be surmised as follows: hypertension associated with aortic coarctation produces abnormal systolic pressure load on the left ventricle, thus increasing left ventricular systolic circumferential wall stress [28], which may be defined as: stress = Pr/Zh, where P is intracavitary pressure, r is chamber radius, and h is myocardial wall thickness. The increased wall stress is an important stimulus to left ventricular hypertrophy. The increased wall thickness may help reduce systolic wall stress toward normal, and this may indeed be an adaptive mechanism to pump blood against high pressures. While myocardial hypertrophy may be an important compensatory mechanism, it may itself become a pathologic process [29, 30] especially if there is progressive hypertrophy. Myocardial hypertrophy is accomplished by an increase in muscle cell volume (not hyperplasia) and is usually accompanied by an increase in collagen synthesis and hyperplasia of stromal elements. In the presence of excessive hypertrophy, maintenance of adequate oxygen supply, especially to the subendocardial region, may become difficult. The hypertrophied myocardium may be functionally abnormal. Furthermore, if the hypertrophy does not keep pace with the work load, myocardial dysfunction sets in. There is thus a complex interrelationship between myocardial hypertrophy and cardiac dysfunction [28]. In our case, exposure of the left ventricle to excessive and continued pressure load may have resulted in left ventricular hypertrophy, myocardial dysfunction, and left ventricular dilatation, resulting in “hypertensive cardiomyopathy” or more correctly in hypertensive heart disease. It is not clear whether this is a normal response to excessive pressure load or if it is an abnormal myocardial response in this infant to the pressure load.
Diagnosis
The cause of extreme left ventricular dilatation and poor left ventricular function was not identified at presentation. Poor pulses in all four extremities secondary to markedly diminished cardiac output masked the initial diagnosis of aortic coarctation. However, following anti- congestive therapy, the cardiac output increased and the pulse differential between the arm and leg became obvious, and the diagnosis of coarctation became clear. Initial echocardiographic studies were brief and once an enlarged left ventricle with poor function was detected, the usual complete examination was not performed. A brief view of the aortic arch from the suprasternal notch was unrevealing. After high clinical suspicion of aortic coarctation following anti-congestive therapy, aortic coarctation was detected by a suprasternal notch two-dimensional image of the aortic arch and by markedly increased descending aortic Doppler flow velocity. Subsequent to this experience, we insist on a complete echo-Doppler study in each patient, even if the clinical diagnosis is clearly confirmed in the initial phases of the echo-Doppler study.
Choice of Therapy
In this infant relief of aortic obstruction was the only way one could conceivably expect improvement in left ventricular function. Of the two choices, surgical resection, and balloon angioplasty, we opted for the latter. We felt that anesthetic and surgical risk was high in the face of poor left ventricular function. Although there is some controversy with respect to balloon angioplasty of native coarctations [31, 32, 33, 34], based on our previous experience [26, 27, 35, 36] we felt that balloon angioplasty was the therapeutic procedure of choice and accomplished it safely. The follow-up data (Figure 9, Figure 10 & Table 2) suggested excellent relief of coarctation, with improvement in left ventricular size and normalization of left ventricular function. We will continue to recommend balloon angioplasty as a therapeutic procedure of choice for symptomatic infants with aortic coarctation. Although the re- coarctation rate is high when balloon angioplasty is used in neonates and infants [36, 37], such re-coarctation can easily be treated with repeat balloon angioplasty (or even surgery if one prefers) at a later date when the infant is stable and less acutely ill than at the time of initial presentation.
Conclusion
Based on the experience with this case and other observations, we would continue to suggest that balloon angioplasty in neonates and young infants is valuable in critically ill infants, particularly when the avoidance of aortic cross-clamping required for surgery is helpful in the overall management. Such special circumstances include infants with shock-like syndrome [38], severe myocardial dysfunction and hypertensive cardiomyopathy (Figures 9A & Figure 10A) [24], prior spontaneous cerebral hemorrhage [39], severely compromised ventricular function [24, 39] and biliary atresia awaiting liver transplantation [39].
Summary and Conclusions
Five different cases were reviewed in this paper. The first case describes effective use of propranolol to relieve severe right ventricular infundibular obstruction which helped passing a catheter across the obstruction. This resulted in relieving pulmonary valve stenosis with balloon pulmonary valvuloplasty. Step by step description of the management of infundibular stenosis associated with pulmonary stenosis was reviewed. The second case reports first successful transcatheter closure of an ASD with buttoned device in a baby weighing 3.6 kg. This report indicated that it is possible to close ASDs with the buttoned device and that further clinical trials are in order. An unusual combination of tricuspid atresia and persistent Truncus arteriosus was documented in the next case. Rarity of this abnormality and recommendation for prompt surgical palliation were emphasized. First successful percutaneous occlusion of PDA with buttoned device in a child was documented in the fourth case. Based on this experience, we concluded that placement of buttoned device for occlusion of the PDA is feasible and that further clinical trials are justified. The final case illustrates an uncommon manifestation of coarctation of the aorta as cardiomyopathy in a baby and successful management with balloon angioplasty in the critically ill infant. These cases document either uncommon combination of congenital heart defects or illustrate effective treatment of congenital heart defects with novel medical or percutaneous methods.
References
-
Rao PS (1970) Clinical Case Reports – 1970. Jour of Clin Cas Rep, Med Imag and Heal Sci 5(5).
-
Rao PS (2023) Clinical Case Reports 1971-1974. Jour of Med Case Stud 1(1): 000105.
-
Rao PS (2023) Clinical Case Reports 1976-1979. Jour of Med Case Stud 1(1): 000109.
-
Rao PS (2024) Clinical Case Reports 1980 - 84 (Contrast Echocardiography). Jour of Med Case Stud 2(1): 000113.
-
Rao PS (2024) Clinical Case Reports 1983 - 87. Jour of Med Case Stud 2(1): 000114.
-
Thapar MK, Rao PS (1989) Significance of infundibular obstruction following balloon valvuloplasty for valvar pulmonic stenosis. Am Heart J 118(1): 99-103.
-
Thapar MK, Rao PS (1990) Use of propranolol for severe dynamic infundibular obstruction prior to balloon pulmonary valvuloplasty. Cathet Cardiovasc Dgn 19(4): 240-241.
-
Pearl W, Wilkin JH (1991) Balloon pulmonary valvuloplasty. Am Heart J 121: 1839.
-
Rao PS, Thapar MK (1991) Balloon pulmonary valvuloplasty (Reply to letter). Am Heart J 121: 1839- 1840.
-
Rao PS, Sideris EB, Chopra PS (1991) Catheter closure of atrial septal defect: Successful use in a 3.6 kg infant. Am Heart J 121: 1826-1829.
-
Sideris EB, Sideris SE, Foulkes JP, Ehly RL, Smith JE, et al. (1990) Transvenous atria1 septal occlusion in piglets using a “buttoned” double disk device. Circulation 81(1): 312-318.
-
Rao PS (2020) Atrial septal defects. In: Rao PS (Eds.), Pediatric Cardiology: How It Has Evolved Over The Last 50 Years. Cambridge Scholars Publishing, pp: 321-386.
-
King TD, Thompson SL, Mills NL (1978) Measurements of atria1 septal defect during cardiac catheterization: Experimental and clinical results. Am J Cardiol 41(3): 537-542.
-
Rao PS, Levy J, Nikicicz E, Gilbert-Barness EF (1991) Tricuspid atresia: Association with persistent _truncus_ _arteriosus_ - A review. Am Heart J 122: 829-835.
-
Rao PS (1991) Tricuspid atresia with common arterial trunk (Letter).International J Cardiol 30: 367-368.
-
Rao PS (1980) A unified classification of tricuspid atresia. Amer Heart J 99: 799-804.
-
Sideris EB, Sideris SE, Ehly RL (1990) Occlusion of patent ductus arteriosus in piglet by a double disk self- adjustable device (Abstract). J Am Coll Cardiol 15: 240A.
-
Rao PS, Wilson AD, Levy JM, Gupta VK, Chopra PS (1991) Role of “buttoned” double-disk device in the management of atrial septal defects (abstract). J Am Coll Card 17: 134A.
-
Rao PS, Wilson AD, Sideris EB, Chopra PS (1991) Transcatheter closure of patent ductus arteriosus with buttoned device: First successful clinical application in a child. Am Heart J 121(6): 1799-1802.
-
Rao PS (2020) Patent ductus arteriosus. In: Rao PS (Eds.), Pediatric Cardiology: How It Has Evolved Over The Last 50 Years. Cambridge Scholars Publishing.
-
Rao PS, Sideris EB, Haddad J, Rey C, Hausdorf G, et al. (1993) Transcatheter occlusion of patent ductus arteriosus with adjustable buttoned device: Initial clinical experience. Circulation 88(3): 1119-1126.
-
Rao PS, Kim SH, Rey C, Onorato E, Sideris EB (1998) Results of transvenous buttoned device occlusion of patent ductus arteriosus in adults. Am J Cardiol 82(2): 827-829.
-
Rao PS, Kim SH, Choi J, Rey C, Haddad J, et al. (1999) Follow-up results of transvenous occlusion of patent ductus arteriosus with buttoned device. J Am Coll Cardiol 33(3): 820-826.
-
Salahuddin N, Wilson AD, Rao PS (1991) An unusual presentation of coarctation of the aorta in infancy: Role of balloon angioplasty in the critically ill infant. Am Heart J 122(6): 1772-1775.
-
Rao PS, Andaya WG (1986) Chronic afterload reduction in infants and children with primary myocardial disease. J Pediatr 108(4): 530-534.
-
Rao PS (1987) Balloon angioplasty for coarctation of the aorta in infancy. J Pediatr 110: 713-718.
-
Rao PS, Thapar MK, Gala, Wilson AD (1990) Follow-up results of balloon angioplasty of native coarctation in neonates and infants. Am Heart J 120(6): 1310-1314.
-
Massie BM (1987) Myocardial hypertrophy and cardiac failure: a complex interrelationship. In: Massie BM (Eds.), The heart and hypertension, Yorke Medical Books, New York, USA, pp: 249-260.
-
Wikman-Coffelt J, Parmby WW, Mason DT (1979) The cardiac hypertrophy process: analysis of factors determining pathologic versus physiologic development. Circ Res 45: 697-707.
-
Grossman W (1980) Cardiac hypertrophy: Useful adaptation or pathologic process. Am J Med 69(40: 576- 584.
-
Lock JE (1984) Now that we can dilate-should we. Am J Cardiol 54: 1360.
-
Rao PS (1989) Which coarctations should we balloon dilate. Am Heart J 117: 787-789.
-
Tynan M, Finley JP, Fontes V, Hess J, Kan J (1990) Balloon angioplasty for the treatment of native coarctation: results of valvuloplasty and angioplasty of congenital anomalies registry. Am J Cardiol 65(11): 790-792.
-
Rao PS (1990) Balloon angioplasty of native coarctation (Letter). Am J Cardiol 66: 1401.
-
Rao PS (1989) Balloon angioplasty of aortic coarctation: a review. Clin Cardiol 12(11): 618-628.
-
Rao PS, Chopra PS (1991) Role of balloon angioplasty in the treatment of aortic coarctation. Ann Thorac Surg 52(3): 621-631.
-
Rao PS, Thapar MK, Kutayli F, Carey P (1989) Causes of recoarctation following balloon angioplasty of unoperated aortic coarctations. J Am Coll Cardiol 13(1): 109-115.
-
Rao PS, Wilson AD, Brazy J (1992) Transumbilical balloon coarctation angioplasty in a neonate with critical aortic coarctation. Am Heart J 124: 1622-1624.
-
Rao PS (1996) Should balloon angioplasty be used as a treatment of choice for native aortic coarctations? J Invasive Cardiol 8: 301-313.
- Ramsay Hunt Syndrome Presenting as Gait Imbalance without Facial Paralysis: A Case Report
- Unveiling Hidden Culprits: An Observational Study of Upper Gastrointestinal Endoscopy Findings in Symptomatic Cholelithiasis Patients
- Assessing Health Care Providers’ Proficiency in International Patient Safety Goals: A Study to Assess the Knowledge &Practice on Patient Safety in a Tertiary Care Teaching Hospital in Gujarat
- Challenges in Diagnosing Child Language Disorders
- Stunting Service Management Model in the South-Central Timor Region, East Nusa Tenggara, Indonesia
- Acute Small Bowel Obstruction Presenting as Gangrenous Jejunal Loop Secondary to Intestinal Endometriosis – A Rare Case Report