Clinical Case Reports 1992 - 94
Five interesting cases reported between 1992 and 1994 were reviewed. The first case documents successful treatment of chylothorax with balloon angioplasty of baffle obstruction following Mustard operation. The second case illustrates successful relief of supra-valvar pulmonary artery stenosis that developed after arterial switch procedure by balloon dilatation. In the third case, shock-like syndrome developed in an 11-day-old baby with severe aortic coarctation which was relieved by balloon angioplasty; the procedure was performed via the umbilical artery, sparing the femoral artery. The fourth case documents percutaneous occlusion of patent ductus arteriosus with a buttoned device in an adult patient; this was first case of using this device in an adult patient. The final case points to late clinical presentation of the origin of the anomalous circumflex coronary artery from the pulmonary artery several years following repair of aortopulmonary window in infancy. Surgical correction of this anomaly was successfully accomplished. The cases presented successful use of catheter or surgical interventional procedures to address uncommon types of cardiac problems.
Introduction
Continuing the case series published previously [1, 2, 3, 4, 5] and those in press or under review [6], this paper reviews cases published between 1992 and 1994.
Successful Treatment with Balloon Angioplasty of Chylothorax Secondary to Baffle Obstruction Following Mustard Operation
Introduction: Obstruction of vena caval return after the Mustard procedure has been reported. However, chylothorax following such obstruction is rare. We have observed an infant who developed chylothorax following the Mustard procedure that was secondary to obstruction of both superior and inferior limbs of the Mustard baffle. Both the chylothorax and the baffle obstruction were successfully relieved by balloon angioplasty. This report documents these events.
Case Report: A neonate with cyanosis was diagnosed to have transposition of the great arteries with intact ventricular septum by echo-Doppler studies, confirmed by cardiac catheterization and selective cine-angiography. Balloon atrial septostomy improved systemic arterial oxygen saturation from the mid-50s to the low-80s. Because of the origin of both right and left coronary arteries from the same sinus of Valsalva, no arterial switch procedure was recommended. Instead, the child underwent elective venous switch operation of the Mustard type at the age of 9 months. Autologous pericardium was used for the interatria1 venous diversion. The surgery and postoperative course were uneventful and the infant was discharged home on the seventh postoperative day with a chest x-ray film showing a normal-sized heart and clear lung fields (Figure 1A). Re- examination with a repeat chest film 3 weeks later revealed similar findings. Approximately 8 weeks following surgery the infant presented with tachypnea and dyspnea and a chest x-ray film revealed left hemithorax opacity (Figure 1B), interpreted as pleural effusion. A pleural tap revealed chylous effusion (triglyceride level 1000 mg/dl and chylomicrons on microscopy). A chest tube was placed and the child was started on a medium-chain triglyceride diet. There was continued drainage from this chest tube. An additional right pleural effusion (Figure 1C) developed that required a right chest tube as well.
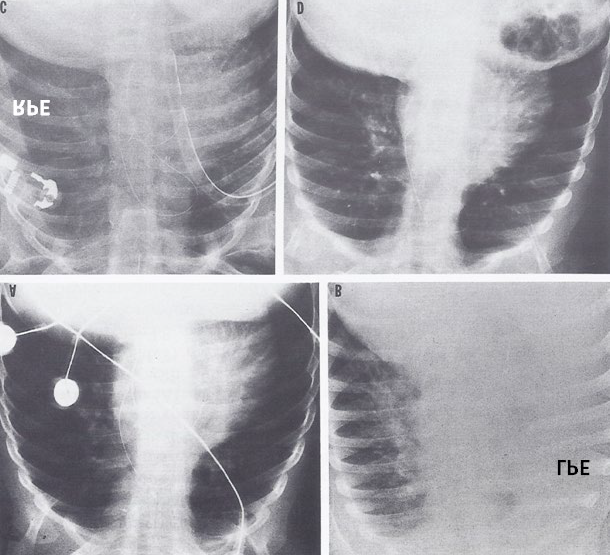
Figure 1A & Figure1B: Antero-posterior views of chest x-rays, one and eight weeks following a Mustard operation, respectively demonstrating a normal-sized heart with clear lung fields (A) a week following the Mustard operation, while the x-ray eight weeks following surgery shows left hemi thorax density (B), interpreted as a pleural effusion (LPE). Upon pleural tapping, the fluid was found to be a chylous effusion. Following chest tube drainage of the left pleural effusion, a right pleural effusion (RPE) developed (C). Three months following the balloon angioplasty of both the inferior and superior baffles of Mustard surgery (Figures 2A & Figure 3A), a chest x-ray shows clear lung fields (D). Modified from Rao PS, et al. [7].
An echo-Doppler study revealed well-functioning ventricles, no pericardial effusion, and a narrowed upper pole of the Mustard baffle with turbulent flow across it. The inferior pole of the baffle was not visualized, although the inferior vena cava appeared somewhat dilated. Because of persistent drainage from both chest tubes despite a medium-chain triglyceride diet, cardiac catheterization and angiography were performed to confirm the echo-Doppler diagnosis of baffle obstruction and to consider balloon angioplasty. Catheterization data revealed no evidence for shunts, but there were significant pressure gradients between vena cavae and the systemic venous atrium (Table 1). Angiography revealed significant obstruction of both the superior (Figure 2A) and inferior (Figure 3A) limbs of the baffle; they respectively measured 3.8 and 2.8 mm (Table 1).
| Site | Before Angioplasty | After Angioplasty | At 6-month Follow-up |
|---|---|---|---|
| Pressures (mm Hg) | |||
| SVC | a-22, v-21, m-20 | a-12, v-14, m-12 | a-6, v-7, m-6 |
| SVA | a-8, v-9, m-5 | a-9, v-13, m-8 | a-5, v-7, m-4 |
| IVC | a-12, v-13, m-12 | a-9, v-10, m-8 | a-6, v-7, m-5 |
| Gradients (mm Hg) | |||
| Superior limb | m-15 | m-4 | m-2 |
| Inferior limb | m-7 | m-0 | m-1 |
| Angiographic size (mm)* | |||
| Superior limb | 3.8 | 7.4 | 7.8 |
| Inferior limb | 2.8 | 7.1 | 8 |
Table 1: Pressure gradients across and sizes of obstructed Mustard baffle prior to and immediately after balloon angioplasty and
IVC, Inferior vena cava; SVA, systemic venous atrium; SVC, superior vena; a, ‘a’ wave; v, ‘v’ wave; m, mean. *Average of postero-anterior and lateral view diameters. Reproduced from Rao PS, et al. [7].
![Figure 2: Selected cine frame of a superior vena caval (SVC) angiogram in postero-anterior projection, demonstrating the narrowing (arrow) of the superior limb of the Mustard baffle (A). Note the opacification of the azygos vein (Az) partly decompressing the SVC. This narrowing improved significantly following balloon angioplasty (B). Note that the Az is no longer seen, indirectly indicating the relief of SVC obstruction. c, catheter; LV, left ventricle; PA, pulmonary artery. Reproduced from Rao PS, et al. [7].](/fulltextimages/12060/fig_2.png)
Figure 2: Selected cine frame of a superior vena caval (SVC) angiogram in postero-anterior projection, demonstrating the narrowing (arrow) of the superior limb of the Mustard baffle (A). Note the opacification of the azygos vein (Az) partly decompressing the SVC. This narrowing improved significantly following balloon angioplasty (B). Note that the Az is no longer seen, indirectly indicating the relief of SVC obstruction. c, catheter; LV, left ventricle; PA, pulmonary artery. Reproduced from Rao PS, et al. [7].
![Figure 3: Selected cine frame of an inferior vena caval (IVC) angiogram in postero-anterior projection demonstrating the narrowing (arrow) of the inferior limb of the Mustard baffle (A). This narrowing improved significantly following balloon angioplasty (B). PA, pulmonary artery; SVA, systemic venous atrium. Reproduced from Rao PS, et al. [7].](/fulltextimages/12060/fig_3.png)
A 15 mm diameter, 3 cm long balloon on a #8F catheter (Meditech Devices Inc., Apple Valley, Calif.) was chosen and was initially positioned across the superior pole of the baffle (Figure 4A); balloon angioplasty (Figure 4B) was performed with three successive inflations at 4, 5, and 6 atm of pressure of 10-second duration each. Ten minutes following the procedure, superior vena caval angiography (Figure 2B) and pressure pullback (Table 1) across the dilated baffle obstruction were recorded. Balloon angioplasty of the inferior limb of the baffle (Figure 5A & Figure 5B), a pressure pullback recording (Table 1), and inferior vena caval angiography (Figure 3B) were performed in a similar manner. A guide wire was always left in position across the area of freshly dilated lesion so that the tips of the catheter or guide wires were not manipulated in these areas. Arterial pressure was monitored throughout the procedure; the pressure did not change significantly during balloon angioplasty.
![Figure 4: Selected cineradiographic frames of a balloon angioplasty catheter positioned across the narrowed superior limb of the Mustard baffle, demonstrating waisting of the balloon (A) during the initial phases of balloon inflation, which was completely abolished (B) on further inflation of the balloon. No residual waisting was noted during the second and third balloon inflations (not shown). Reproduced from Rao PS, et al. [7].](/fulltextimages/12060/fig_4.png)
Figure 4: Selected cineradiographic frames of a balloon angioplasty catheter positioned across the narrowed superior limb of the Mustard baffle, demonstrating waisting of the balloon (A) during the initial phases of balloon inflation, which was completely abolished (B) on further inflation of the balloon. No residual waisting was noted during the second and third balloon inflations (not shown). Reproduced from Rao PS, et al. [7].
![Figure 5: Selected cineradiographic frames of a balloon angioplasty catheter positioned across the narrowed inferior limb of the Mustard baffle, demonstrating waisting of the balloon (A) during the initial phases of balloon inflation, which was completely abolished (B) on further inflation of the balloon. No residual waisting was noted during the second and third balloon inflations (not shown). Reproduced from Rao PS, et al. [7].](/fulltextimages/12060/fig_5.png)
Figure 5: Selected cineradiographic frames of a balloon angioplasty catheter positioned across the narrowed inferior limb of the Mustard baffle, demonstrating waisting of the balloon (A) during the initial phases of balloon inflation, which was completely abolished (B) on further inflation of the balloon. No residual waisting was noted during the second and third balloon inflations (not shown). Reproduced from Rao PS, et al. [7].
Chest tube drainage stopped over the next 24 hours and the chest tubes were removed. There was no further accumulation of pleural fluid. Repeat chest films 3 (Figure 1D) and 6 months following angioplasty did not reveal any recurrence of chylothorax. Cardiac catheterization performed
6 months following angioplasty revealed continuing relief of pressure gradient across the balloon-dilated baffle obstruction (Table 1) and no restenosis was observed on angiography Figures 6 & Figure 7 [7, 8].
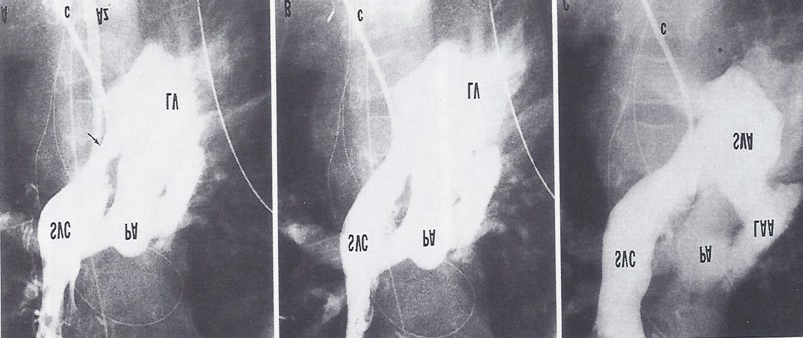
Figure 6A & B: Selected cine frames of a superior vena caval (SVC) angiogram in postero-anterior projection, demonstrating the narrowing (arrow) of the superior limb of the Mustard baffle and its improvement following balloon angioplasty, as shown in Figure 2. C. Repeat angiography six months after balloon angioplasty shows the continued improvement of the superior limb of the Mustard baffle. Az, azygos vein; c, catheter; LAA, left atrial appendage; LV, left ventricle; PA, pulmonary artery; SVA, systemic venous atrium. Reproduced from Rao, et al. [8].
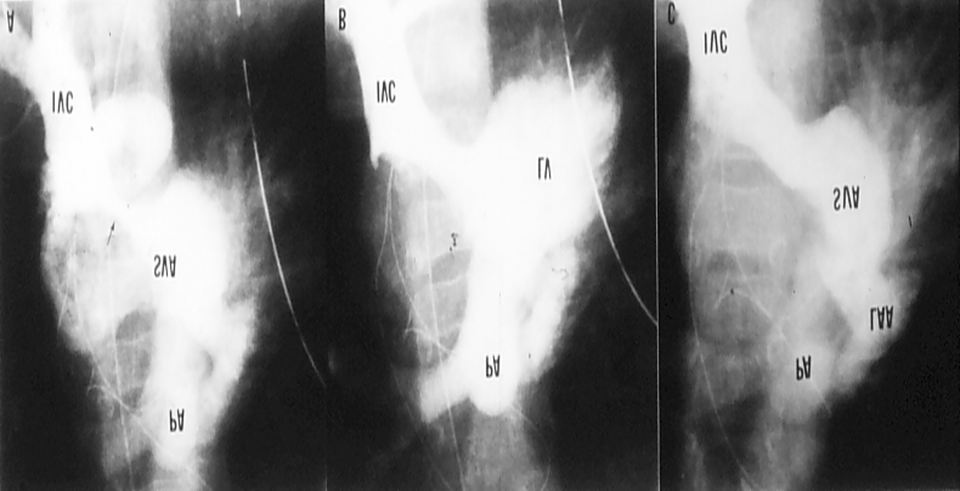
Figure 7A & B: Selected cine frames of an inferior vena caval (IVC) angiogram in postero-anterior projection, demonstrating the narrowing (arrow) of the inferior limb of the Mustard baffle and its improvement following balloon angioplasty, as shown in Figure 3. C. Repeat angiography six months after balloon angioplasty shows the continued improvement of the inferior limb of the Mustard baffle. LAA, left atrial appendage; LV, left ventricle; PA, pulmonary artery; SVA, systemic venous atrium. Reproduced from Rao, et al. [8].
Subsequent to the above report, we encountered another patient who had obstructed inferior baffle following Mustard operation (Figure 8A) [8]. Balloon angioplasty with a 15mm diameter balloon reduced the mean pressure gradient (from
5 mmHg to 3 mmHg) with angiographic improvement (Figure 8B). Follow-up echo-Doppler studies revealed continued improvement (Figure 9).
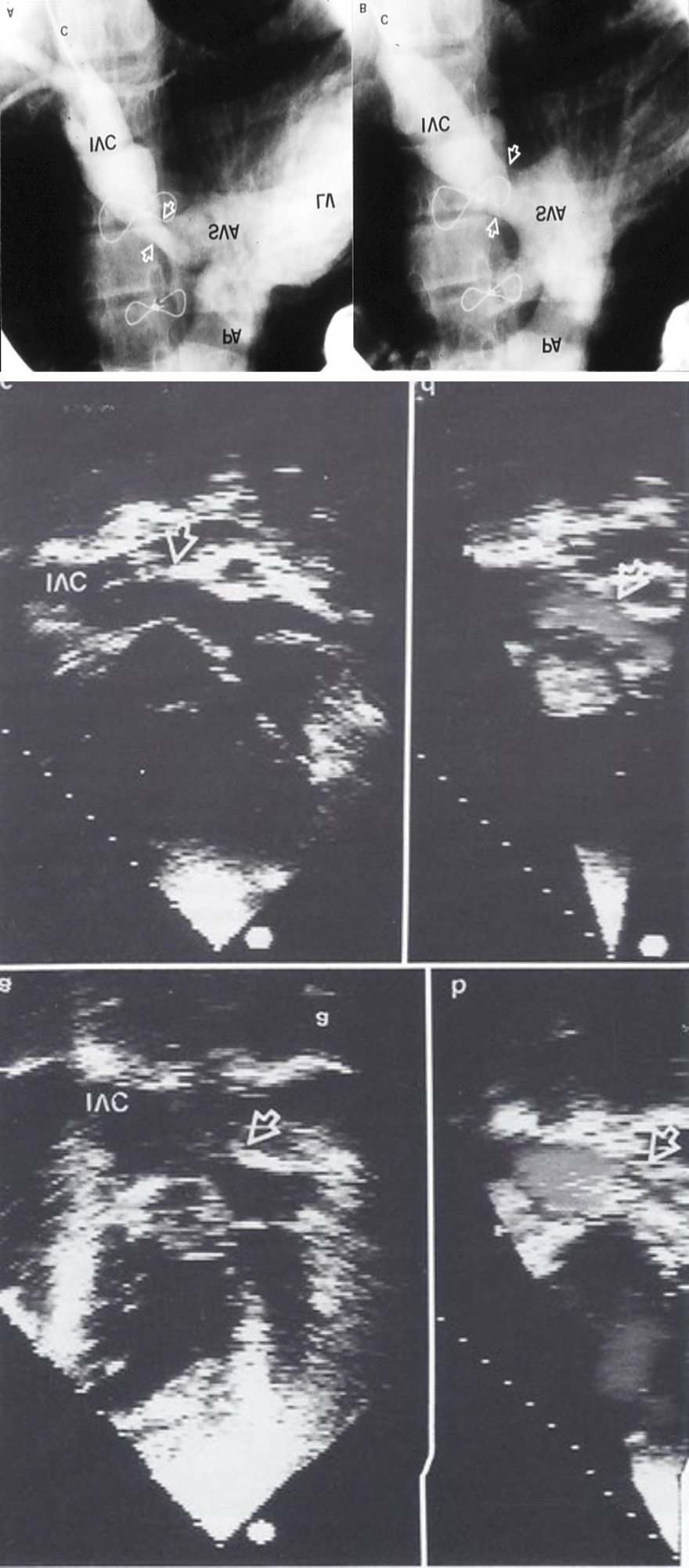
Figure 8A: Selected cine frame of an inferior vena caval (IVC) angiogram in postero-anterior projection, demonstrating narrowing (arrow heads in A) of the inferior limb of the Mustard baffle. B. The narrowing improved significantly (arrow heads in B) following balloon angioplasty. c, catheter; LV, left ventricle; PA, pulmonary artery; SVA, systemic venous atrium. Reproduced from Rao, et al. [8].
Figure 9: Selected video frames of a two-dimensional echocardiogram of the inferior limb of the Mustard baffle (a) in a 15-year- old child, showing the obstructed area (arrow). Color flow mapping (b) shows that flow acceleration and the turbulence starts at this point, confirming the hemodynamic significance of the two-dimensionally visualized narrowing. Also, note the dilated inferior vena cava (IVC). The second row of video frames (c and d) are from the same patient, and were obtained six months after balloon dilatation. Note the wider opening on the two-dimensional echocardiographic frame (c) and the lack of flow acceleration and turbulence (d). Reproduced from Rao, et al. [8].
Discussion: Vena caval obstruction after Mustard operation for transposition of the great arteries has been well documented in the literature as references in our publications [7, 8]. Systemic venous obstruction is more likely to be present than pulmonary venous obstruction. The systemic venous obstruction appears to occur more frequently when Dacron was used for atrial baffle than when an autologous pericardial patch was used. Superior vena caval obstruction appears to occur more frequently than inferior vena caval obstruction. Occurrence of both superior and inferior venae caval obstructions together appears to be even less common. Symptoms from obstruction are more likely to manifest when both venae cavae are obstructed than when only one vena cava is obstructed because of decompression of the segment proximal/distal to the obstruction by the azygos venous system. The occurrence of chylothorax is uncommon; at the time of submitting the above reports for publication [7, 8] we have been able to find only one such case reported with chylothorax [9]. The causes of development of chylothorax are not known. Injury of the major lymphatic channels and high superior vena caval pressure are possible explanations. Prompt clearing of the chylothorax following balloon angioplasty also favors high vena caval pressure as a cause of chylothorax in our case. Although surgical relief of baffle obstruction, when severe, has been the procedure of choice in the past, balloon angioplasty has been employed more recently [10, 11, 12, 13, 14]. While the initial experience of balloon dilatation of obstructed Mustard baffle obstruction in a single patient was not encouraging [11], subsequent experience has shown promise [10, 12, 13, 14]. Relief of pressure gradient and angiographic improvement were documented in most cases. The report from the Valvuloplasty and Angioplasty of Congenital Anomalies Registry listed 22 baffle obstructions that were dilated; 15 (68%) were categorized as successful [14]. It is also interesting to note that pulmonary venous obstruction following the atria1 switch operation can also be successfully balloon-dilated [15, 16]. There is inadequate data to evaluate causes of failure of balloon angioplasty. Dynamic nature of the obstruction, perhaps the use of small balloons or very compliant venous structures that will stretch and not tear the obstructed scar tissue during angioplasty, are possible causes. Based on our experience with balloon angioplasty in other lesions [17, 18], we would be in favor of using balloons that are at least three to four times the size of the obstructed segment; sometimes this may necessitate the use of two balloons [7, 8].
Balloon Dilatation of Supravalvar Pulmonary Artery Stenosis after Arterial Switch Procedure
Introduction: Saxena and her colleagues reported poor results of balloon dilatation of supravalvar pulmonary stenosis after arterial switch procedure [19]. The lesions that they attempted to dilate appear to be diffuse in nature.
In response to this paper, I presented the results of balloon angioplasty of discrete obstructive supravalvar pulmonary artery lesion [20].
Case Report: Supravalvar pulmonary artery stenosis (Figure 10A) that was discovered nearly one year following Jatene procedure was successfully balloon dilated (Figures 10B & Figure 11) [17, 20].
![Figure 9: Selected video frames of a two-dimensional echocardiogram of the inferior limb of the Mustard baffle (a) in a 15-year- old child, showing the obstructed area (arrow). Color flow mapping (b) shows that flow acceleration and the turbulence starts at this point, confirming the hemodynamic significance of the two-dimensionally visualized narrowing. Also, note the dilated inferior vena cava (IVC). The second row of video frames (c and d) are from the same patient, and were obtained six months after balloon dilatation. Note the wider opening on the two-dimensional echocardiographic frame (c) and the lack of flow acceleration and turbulence (d). Reproduced from Rao, et al. [8].](/fulltextimages/12060/fig_9.png)
Discussion: Development of supravalvar pulmonary artery stenosis following Jatene procedure has been documented. Balloon dilatation of the stenotic segment is feasible in patients who have discrete narrowing [17, 20] while it is not possible to relieve the obstruction if the obstructive segment is diffuse and involves a long segment of the pulmonary artery [19, 21].
![Figure 10: Selected cine frames in lateral view of pulmonary artery angiogram demonstrating narrowing (arrow in A) of the pulmonary artery that developed following Jatene operation. Frame B illustrates (arrow in B) improvement in the obstruction. The pressure gradient improvement is shown in Figure 11. Reproduced from Rao [17].](/fulltextimages/12060/fig_10.png)
Figure 11A: Pressure pullback tracings across supravalvar pulmonary artery stenosis demonstrating significant gradient across this region. B. The gradient disappeared following balloon dilatation. Aortic (Ao) pressure is recorded in B. DPA, distal pulmonary artery; PPA, proximal pulmonary artery. Reproduced from Rao [17].
Trans-umbilical Balloon Coarctation Angioplasty in a Neonate with Critical Aortic Coarctation
Introduction: While balloon angioplasty of native aortic coarctation is successful in relieving aortic obstruction, because of high rate of recurrence, surgery is most commonly used for aortic coarctations in neonates and young infants. We have used balloon angioplasty for native coarctation in a neonate who presented with shock-like syndrome; the procedure was performed via an umbilical artery approach, which spares the femoral arteries [22].
Case Report: An 11-day-old infant who weighed 3.9 kg was first seen in the local physician’s office with a 3-day history of upper respiratory tract infection. He was found to be grunting, cyanotic, and poorly perfused. He was immediately ventilated manually and rushed to a local emergency room. There he was intubated, given volume expansion, and started on vasopressor agents; only a transient improvement in color and perfusion was observed. The initial pH was 7.1 with a base deficit of -12.8. Chest x-ray films showed cardiomegaly and evidence of pulmonary venous congestion. Pediatric cardiology consultation along with an echo-Doppler study was obtained immediately. This examination showed evidence of severe aortic coarctation, mild aortic stenosis, no ventricular septal defect, and poor left ventricular shortening fraction. Because severe aortic coarctation was diagnosed, intravenous prostaglandin E1 (PGE1) infusion was started, and significant improvement occurred over the next 30 minutes of observation. The infant was transferred to the University of Wisconsin Children’s Hospital. After further stabilization in the pediatric intensive care unit, the infant was taken to the cardiac catheterization laboratory. Percutaneous right heart catheterization and antegrade left ventricular angiography, which was performed via the right femoral vein, revealed severe aortic coarctation with a 35 mmHg gradient across the aortic coarctation. The coarcted aortic segment measured 2 mm, and the descending aorta at the level of the diaphragm measured 6 mm. Because the need for relief of aortic coarctation was indicated, the previously placed #3.5F umbilical arterial catheter was exchanged for a #5F umbilical artery catheter over a guide wire, and the tip of the catheter was advanced proximal to the aortic coarctation. Four hundred units of heparin were administered. Then a 0.032 inch extra-stiff Amplatz guide wire (Cook Inc., Bloomington, Ind.) was positioned within the #5F catheter, and the tip of the guide wire was positioned proximal to the coarctation. The catheter was exchanged for a #5.3F Proflex 5 balloon dilatation catheter (Peripheral Systems Group, Mountainview, Calif.), which carried a 6 mm balloon. This is a very low profile balloon catheter that is coated with a silicone-based material so that it can be easily advanced over the umbilical artery-iliac artery-aorta junctions without difficulty. The deflated balloon was positioned across the aortic coarctation, and the balloon was inflated twice at 6 atm of pressure for a 5-second duration with a 5-minute interval in between dilatations. Waisting of the balloon was seen during the initial phases of balloon inflation, which abated on further balloon inflation. The Proflex catheter was removed and replaced with a 5F Multi A-2 catheter (Cordis Corp., Miami Lakes, Fla.). Fifteen minutes after the procedure, angiography was repeated, and a pressure pullback tracing across the dilated aortic coarctation was recorded. The peak systolic pressure gradient across the aortic coarctation decreased from 35 mm Hg to 3 mm Hg, and the coarcted aortic segment increased from 2 mm to 5.5 mm. Because it was concluded that there was excellent relief of aortic coarctation, the Multi A-2 catheter was replaced with a 5F umbilical artery catheter and its tip was positioned at the third lumbar vertebra, below the level of renal arteries. The PGE1 infusion was discontinued in the catheterization laboratory. The infant improved markedly, and there was no blood pressure difference between arms and legs. The infant was weaned from the respirator over the next several hours and extubated 20 hours after balloon angioplasty. The infant was discharged 2 days later. Reexamination in the outpatient clinic 2 weeks after discharge revealed good weight gain, no signs of heart failure, and no significant arm-to-leg blood pressure difference. Similar technique was used in a 10-day old infant with severe coarctation [22] with equally gratifying result.
Discussion: Hemodynamic, angiographic, and clinical improvement after balloon angioplasty was achieved by the trans-umbilical artery approach. The method that we have used is similar to that used by Beekman, et al. [23] for balloon aortic valvuloplasty. Availability of low-profile catheters that are coated with silicone-like material (Proflex 5) made this procedure possible. However, more recently, low-profile catheters such as Tyshak II and mini-Tyshak became available which may be used in place of Proflex 5. Development of femoral artery complications, namely poor perfusion, and thrombosed femoral artery after use of the femoral artery for balloon dilatation procedure is well documented in the literature. To avoid arterial complications, alternative umbilical artery for balloon angioplasty is one such approach and can be employed safely and successfully in the neonate while the umbilical arteries are patent. Use of the umbilical artery spares the use of the femoral artery and thus avoids potential arterial complications. On the basis of this experience, we highly recommend the umbilical artery route to relieve aortic coarctation.
Transcatheter Closure of Patent Ductus Arteriosus with an Adjustable Buttoned Device in an Adult Patient
Introduction: While transcatheter occlusion of patent ductus arteriosus (PDA) with buttoned device in children has been reported by Rao, et al. [24, 25], its use in adults has not been documented. In this report [26] percutaneous closure of PDA in an adult patient was presented.
Case Report: A 65-year-old woman had had shortness of breath and palpitations for the previous 2 months, and she had New York Heart Association (NYHA) class II symptoms. She also had long-standing bronchial asthma with mild obstructive disease. On examination, her blood pressure and pulses were normal. There was no cardiomegaly and heart sounds were normal. A grade III/VI continuous murmur was auscultated at the upper left sternal border. Her ECG showed left ventricular volume overload pattern. Chest x-ray was normal. Two-dimensional echocardiography with Doppler color flow imaging was suggestive of small-sized PDA with normal pulmonary artery pressure. In view of the age of the patient and possibly other contributory factors for her symptoms, percutaneous closure of the defect was preferred. Hospital Internal Review Board approval was obtained for the newer nonsurgical approach, and informed consent was obtained from the patient. Cardiac surgery stand-by was available. Oral diazepam was given as premeditation. Diagnostic cardiac catheterization was performed before the nonsurgical closure. Oximetry demonstrated a step up in oxygen saturation from the right ventricle to the pulmonary artery. Pulmonary artery pressure was 25/10 with a mean of 15 mm Hg. Calculated pulmonary to systemic flow ratio was 1.5:1. Aortography in the left anterior oblique view revealed a small ductus arteriosus, with a contrast jet streaming into the pulmonary artery (Figure 12a). Her coronary arteries, left ventricular wall motion, and ejection fraction were normal. Heparin was given as a bolus of 5,000 U initially, then 1000 U/hr throughout the procedure. A 20 mm adjustable buttoned device was chosen after the assessment of the ductus and ampular size.
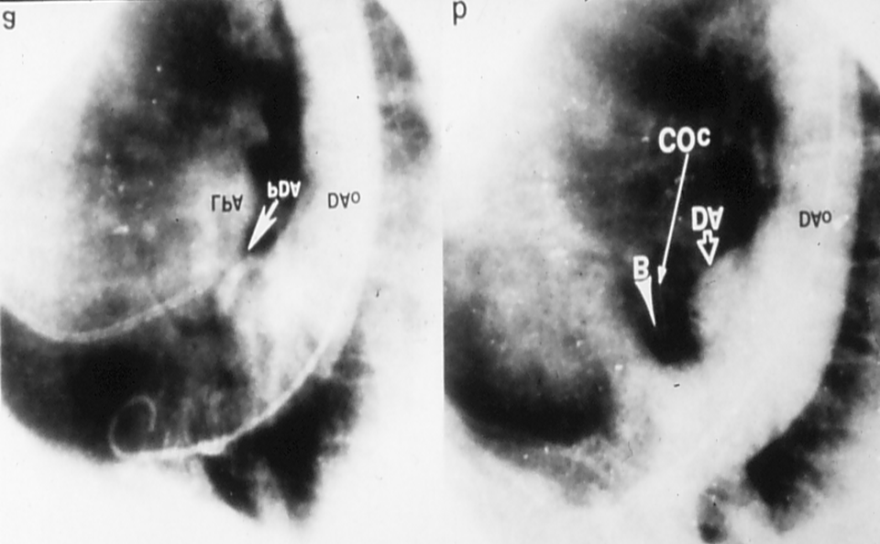
Figure 12A: Aortography in left anterior oblique view showing filling of the pulmonary artery via a patent ductus arteriosus (PDA). Descending aorta (DAo) and left pulmonary artery (LPA) are shown. B. Aortography in left anterior oblique view 15 minutes after implantation of button device showing complete occlusion of left-to-right shunt through ductus. Ductal ampulla (DA), counter-occluder (COc), and button (B) are shown. Reproduced from Lochan, et al. [26].
An end-hole catheter was advanced from the main pulmonary artery through the ductus into the descending aorta. A 0.035-inch exchange guide wire was advanced through this catheter. A long #8F Cordis sheath was inserted over the guide wire and positioned in the descending aorta. The occluder component of the buttoned device was inserted into the sheath after folding it and was advanced with the help of a pusher catheter under fluoroscopic control. After confirming the position of the tip of the sheath in the aorta, the device was extruded into the aorta, which did spring open after delivery. It was kept in position with the help of delivery guide wire. The pusher catheter was removed and a counter occluder was advanced over the wire but within the sheath and extruded into the pulmonary artery, the sheath was withdrawn into the pulmonary artery while maintaining the occluder in position. The counter occluder was advanced over the knot with the help of the tip of the sheath while gentle countertraction was applied on the occluder. Once the radiopaque component of the counter occluder passes beyond the radiopaque button, the process of buttoning the occluder with the counter occluder is deemed to have taken place. It was then further buttoned across the second knot. The wire and nylon thread were cut and withdrawn, and subsequently the sheath was removed. Post deployment repeat aortogram showed minimal leak through the ductus but it disappeared completely 15 minutes later (Figure 12b). We administered three doses of cephazolin (50 mg/kg) intravenously. The first dose was given during the procedure. Second and third doses were given 8 and 16 hours after the first dose. We also gave aspirin 325 mg daily beginning 24 hours after the procedure for 3 months to prevent excessive deposition of platelets. Patient was kept 24 hours in the hospital for observation. Chest x-ray film showed the device in place, and there was no evidence of shunt by Doppler color flow mapping after 24 hours of procedure. At the end of 3 months’ follow-up, the patient had no symptoms, there was no murmur on auscultation, her chest x-ray film showed the device in place, and Doppler color flow mapping did not show any shunt across the ductus.
Discussion: PDAs in patients >60 years of age are uncommon. Similar to our patient, most PDA patients surviving to old age have relatively small left-to-right shunts of borderline hemodynamic significance. We preferred percutaneous closure of ductus with the buttoned device because it needs a small-sized sheath (#7 to 8F) for introduction and flexibility of use in a wide variety of PDAs. After follow-up for three months, the patient had no symptoms, the device was in place on chest x-ray film, and there was no evidence of left-to-right shunt by color Doppler study, indicating that it was a corrective procedure. This appears to be the first adult case of successful PDA closure with the adjustable buttoned device, following reports of successful closure in children [24, 25]. We commented that transcatheter closure with the adjustable buttoned device is a safe, simple, and effective procedure for the closure of PDAs in adults and suggested that long-term follow up data and more experience are necessary before the wider clinical application of this procedure. Indeed, subsequent experience in a large series of PDA in adults was found to be excellent [27]. However, the device is not currently available for clinical use because the inventor of the device did not seek premarket approval from the FDA.
Delayed Presentation of the Origin of the Anomalous Circumflex Coronary Artery From the Pulmonary Artery After Repair of Aortopulmonary Window In Infancy
Introduction: Anomalous origin of the coronary arteries is a well described clinical condition that encompasses a range of presentations from asymptomatic to florid congestive heart failure and myocardial infarction. Origin of the left coronary artery from the pulmonary artery (PA) is generally associated with a high mortality in the first year of life. When the anomaly is associated with other congenital malformations, the initial presentation may be often unrecognized. Surgical correction of associated malformations may unmask the coronary anomaly, resulting in acute, unexpected cardiac decompensation. Failure to anticipate this lesion has resulted in cardiogenic shock and death. Rarely, the coronary artery anomaly presents in a subacute or chronic fashion. We report a late presentation of a circumflex coronary artery arising from the PA following repair of an aortopulmonary window (APW) 14 years previously.
Case Report: A 13-day-old female infant was hospitalized with cyanosis and a heart murmur following an unremarkable pregnancy and delivery. Echocardiography and cardiac catheterization showed a large APW. She was discharged home from the hospital on a regimen of digoxin and furosemide. Over the ensuing year, she required a single hospital admission for control of congestive heart failure. At 13 months, she underwent operative correction. The aortic side of the APW was repaired primarily and the pulmonary artery was closed with a pericardial patch. She was discharged home from the hospital on the tenth postoperative day after an uneventful postoperative course.
She was well until age 15 years, when she began to note exercise-induced chest pain. There was no cyanosis, palpitation, dizziness, or syncope. Results of physical examination were unremarkable. ECG demonstrated right axis deviation and an incomplete right bundle branch block pattern. Graded exercise test with thallium showed stress-induced reversible ischemia of the anterolateral wall of the left ventricle. Her exercise tolerance was normal, and there were no arrhythmias. Echocardiography failed to demonstrate any residual shunt, mitral regurgitation, or pulmonary insufficiency. Cardiac catheterization and angiography demonstrated satisfactory closure of the AP window with no evidence of any septal defect or PDA. Despite this, there was a step-up in oxygen saturation in the PA. A left ventricular angiogram demonstrated paradoxical motion in the posterior wall of the left ventricle again without evidence of mitral insufficiency. Coronary angiography demonstrated a normal course for the right, left main, and left anterior descending (LAD) coronary arteries. The course of the circumflex coronary was quite unusual in that it filled in a retrograde direction by way of collaterals from the LAD, septal, and diagonal branches (Figures 13 & Figure 14). The ostium of the circumflex coronary artery originated from the posterior wall of the PA.
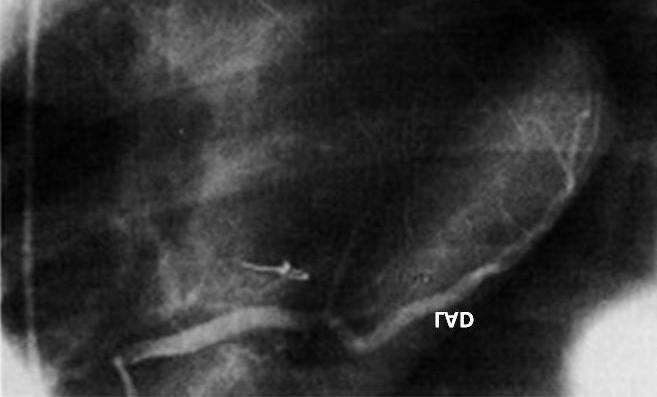
![Figure 13: Coronary angiogram of the left main coronary artery demonstrating a normal left anterior descending artery (LAD) with an absence of the circumflex coronary artery. The distal circumflex is seen filling in a retrograde fashion from the LAD. Reproduced from Chopra et al. [28].](/fulltextimages/12060/fig_13.png)
She underwent reoperation. A coronary artery bypass graft was placed from the aorta to the second obtuse marginal of the circumflex coronary artery using a segment of autologous saphenous vein. The internal mammary arteries appeared to be of inadequate size to perform bypass due to incorporation into sternal closure carried out 14 years previously. The PA was opened, and ostium of the anomalous circumflex coronary artery was suture ligated to preclude any further “coronary steal.” She was discharged from the hospital on the fifth postoperative day. On follow-up 4 months postoperatively, she has resumed an active life-style without further discomfort or physical limitations.
Discussion: Anomalous origin of the circumflex coronary artery is extremely rare and may cause serious perioperative myocardial injury associated with correction of coexisting congenital malformations. We describe a 15-year-old female patient who underwent surgical correction of an aortopulmonary window at 13 months. Fourteen years later, she presented with dyspnea on exertion associated with angina. On cardiac catheterization, she was noted to have a step-up in oxygen saturation in the pulmonary artery and retrograde filling of the circumflex coronary artery from the left anterior descending coronary artery, with drainage into the pulmonary artery. The patient underwent surgical bypass of the anomalous circumflex coronary artery and ligation of its anomalous origin in the pulmonary artery. Her postoperative course was uneventful, with complete relief of symptoms. We have reviewed the features of this rare congenital anomaly and its therapeutic options [28].
Summary and Conclusions
This paper reviews five different case scenarios. In the first case, we report the occurrence of baffle obstruction following Mustard operation which produced chylothorax; balloon angioplasty of both superior and inferior baffles was performed resulting in complete resolution of chylothorax. On the basis of this experience and that with balloon angioplasty in other vascular stenotic lesions, we recommend using balloons that are at least three to four times the size of the obstructed segment. The second case illustrates successful relief of supra-valvar pulmonary artery stenosis that developed after arterial switch procedure by balloon dilatation. These data led us to conclude that balloon angioplasty is successful in relieving discrete obstructive lesions and that diffuse and long segment narrowing of the pulmonary artery are not amenable to balloon dilatation. In the third case, a neonate developed shock-like syndrome secondary to severe aortic coarctation. The aortic obstruction was successfully relieved by trans- umbilical balloon coarctation angioplasty. Using umbilical artery for the procedure spares the femoral artery, avoiding potential arterial complications. Based on this experience, we recommend the trans-umbilical artery approach to relieve aortic obstruction. The fourth case demonstrates transcatheter closure of patent ductus arteriosus with an adjustable buttoned device in an adult patient. This was first case documenting buttoned device closure of PDA in an adult patient. In the final case, delayed manifestation of the origin of the anomalous circumflex coronary artery from the pulmonary artery several years following repair of aortopulmonary window in infancy was documented. Bypass graft was surgically inserted to perfuse the anomalous circumflex coronary artery along with concurrent ligation of the entry into the pulmonary artery. The rarity of this congenital vascular anomaly was pointed out and the available therapeutic options were reviewed. The cases presented were uncommon and were successfully addressed with catheter interventional or surgical procedures as deemed appropriate.
References
-
Rao PS (2023) Clinical Case Reports – 1970. Jour of Clin Cas Rep, Med Imag and Heal Sci 5(5).
-
Rao PS (2023) Clinical Case Reports 1971-1974. Jour of Med Case Stud 1(1): 000105.
-
Rao PS (2023) Clinical Case Reports 1976-1979. Jour of Med Case Stud 1(1): 000109.
-
Rao PS (2024) Clinical Case Reports 1980 - 84 (Contrast Echocardiography). Jour of Med Case Stud 2(1): 000113.
-
Rao PS (2024) Clinical Case Reports 1983 - 87. Jour of Med Case Stud 2(1): 000114.
-
Rao PS (2024) Clinical Case Reports 1990 - 91. Jour of Med Case Stud 2(1): 000120.
-
Rao PS, Wilson AD (1992) Chylothorax, an unusual complication of baffle obstruction following Mustard operation: Successful treatment with balloon angioplasty. Am Heart J 123(1): 244-248.
-
Rao PS, Thapar MK (1993) Balloon dilatation of other congenital and acquired stenotic lesions of the cardiovascular system. In: Rao PS (Eds.), Transcatheter Therapy in Pediatric Cardiology. Wiley-Liss, New York, USA, pp: 275-320.
-
Cumming GR, Ferguson CC (1975) Obstruction of superior vena cava after the Mustard procedure for transposition of the great arteries: Conservative management of chylothorax. J Thorac Cardiovasc Surg 70(2): 242-247.
-
Kirk CR, Gibbs JL, Wilkinson, Wilson N, Dickinson DF, et al. JL (1988) Protein-losing enteropathy caused by baffle obstruction after Mustard’s operation. Br Heart J 59(1): 69- 72.
-
Waldman JD, Waldman J, Jones MC (1983) Failure of balloon dilatation in mid-cavity obstruction of the systemic venous atrium after the Mustard operation. Pediatr Cardiol 4(2): 151-154.
-
Lock JE, Bass JL, Castaneda-Zuniga W, Fuhrman BP, Rashkind WJ, (1984). Dilatation angioplasty of congenital or operative narrowings of venous channels. Circulation 70(3): 457-64.
-
Benson LN, Yeatman L, Laks H (1985) Balloon dilatation for superior vena caval obstruction after Senning procedure. Cathet Cardiovasc Diagn 11(1): 63-68.
-
Mullins CE, Latson LA, Neches WH, Colvin EV, Kan J (1990) Balloon dilation of miscellaneous lesions: results of valvuloplasty and angioplasty of congenital anomalies registry. Am J Cardiol 65(11): 802-803.
-
Cooper SG, Sullivan ID, Bull C, Taylor JFN (1989) Balloon dilation of pulmonary venous pathway obstruction after Mustard repair for transposition of the great arteries. J Am Co11 Cardiol 14(1): 194-198.
-
Coulsen JD, Jennings RB, Johnson JD. Pulmonary venous obstruction after Senning procedure: relief by catheter balloon dilatation. Br Heart J 64(2): 160-162.
-
Rao PS (1989) Balloon angioplasty and valvuloplasty in infants. children and adolescents, Year Book Med Publishers, Curr Probl Cardiol Chicago, pp: 417-500.
-
Rao PS (1989) Balloon dilatation in infants and children with cardiac defects. Cathet Cardiovasc Diagn 18(3): 136-149.
-
Saxena A, Fong LV, Ogilvie BC, Keeton BR (1990) Use of balloon dilatation to treat supravalvar pulmonary stenosis developing after anatomical correction for complete transposition. Br Heart J. 64(2): 151-5.
-
Rao PS (1992) Balloon dilatation of supravalvar pulmonary stenosis after arterial switch procedure for complete transposition (Letter). Br Heart J 67(2): 204- 205.
-
Zeevi B, Keane JF, Perry SB, Lock JE (1989) Balloon dilation of postoperative right ventricular outflow obstructions. J Am Coll Cardiol 14(2): 401-408.
-
Rao PS, Wilson AD, Brazy J (1992) Transumbilical balloon coarctation angioplasty in a neonate with critical aortic coarctation. Am Heart J 124(6): 1622-1624.
-
Beekman RH, Rocchini AP, Andes A (1991) Balloon valvuloplasty for critical aortic stenosis in the newborn: influence of new catheter technology. J Am Coll Cardiol 17(5): 1172-1176.
-
Rao PS, Wilson AD, Sideris EB, Chopra PS (1991) Transcatheter closure of patent ductus arteriosus with buttoned device: First successful clinical application in a child. Am Heart J 121(6): 1799-1802.
-
Rao PS, Sideris EB, Haddad J, Rey C, Hausdorf G, et al. (1993) Transcatheter Occlusion of Patent Ductus Arteriosus with Adjustable Buttoned Device: Initial Clinical Experience. Circulation 88(3): 1119-1126.
-
Lochan R, Rao PS, Samal AK, Khanna AR, Mani GK, et al. (1994) Transcatheter closure of patent ductus arteriosus with an adjustable buttoned device in an adult patient. Am Heart J 127(4): 941-943.
-
Rao PS, Kim SH, Rey C, Onorato E, Sideris EB (1998) Results of Transvenous Buttoned Device Occlusion of Patent Ductus Arteriosus in Adults. Am J Cardiol 82(6): 827-829.
-
Chopra PS, Reed WH, Wilson AD, Rao PS (1994) Delayed presentation of anomalous circumflex coronary artery arising from pulmonary artery following repair of aortopulmonary window in infancy. Chest 106(6): 1920- 1922.
- Ramsay Hunt Syndrome Presenting as Gait Imbalance without Facial Paralysis: A Case Report
- Unveiling Hidden Culprits: An Observational Study of Upper Gastrointestinal Endoscopy Findings in Symptomatic Cholelithiasis Patients
- Assessing Health Care Providers’ Proficiency in International Patient Safety Goals: A Study to Assess the Knowledge &Practice on Patient Safety in a Tertiary Care Teaching Hospital in Gujarat
- Challenges in Diagnosing Child Language Disorders
- Stunting Service Management Model in the South-Central Timor Region, East Nusa Tenggara, Indonesia
- Acute Small Bowel Obstruction Presenting as Gangrenous Jejunal Loop Secondary to Intestinal Endometriosis – A Rare Case Report