Endoscopic and Colonoscopy Investigation in Anemia: Yield of these Procedures in Identifying a Gastrointestinal Cause
Introduction: Anemia is a common laboratory finding among patients and many inpatients are worked up during their hospital stay with either endoscopy and/or colonoscopy. An evidence-based approach is warranted to determine this course of action is likely to affect treatments and outcomes especially in the inpatient population in other types of anemia as well. Methods: In this retrospective analysis, charts were obtained for inpatients that underwent either endoscopy and/or colonoscopy with anemia during the period of over 5 years at a community hospital. These patient records were reviewed, and data was collected into a standardized collection tool for statistical analysis. Bonferroni method was used to correct for multiple testing parameters. Results: Out of 173 total patients, endoscopic/colonoscopy findings were positive in 6/5 with untyped anemia, 34/20 with anemia of chronic disease (ACD), 49/29 with iron deficiency anemia (IDA), and 34/26 with anemia due to other causes (ADOC) respectively. Positive findings in either endoscopy and/or colonoscopy 75.47%, 91.38%, 72.73%, and 100% with a p value of .026. Conclusion: In cases of anemia without signs of active gastrointestinal bleeding, inpatient examination by either endoscopy and/or colonoscopy found a probable cause in most patients irrespective of the type of anemia.
Introduction
Anemia is an extremely common problem affecting approximately one-fourth of world population [1].
Iron deficiency anemia is the most common type of anemia and is one among the top causes of anemia in 65 years and older patients in developed countries [2]. The most common cause for iron deficiency anemia in developed countries is blood loss and patients are often referred to gastroenterologists for upper gastrointestinal endoscopy and colonoscopy. There is plenty of evidence justifying endoscopic investigation in iron deficiency anemia, but there are no clear guidelines for endoscopic investigation of anemia other than iron deficiency.
Upper and lower gastrointestinal endoscopy are increasingly being done in hospitals in United states for investigating causes of anemia to rule out occult gastrointestinal bleeding [3]. Increased numbers of invasive investigations raise the concern about cost, safety of the patient, and also complications of procedure [4]. This study seeks to examine the yield of endoscopic investigations among patients who were referred for anemia of all causes in a community based hospital.
There is minimal literature on endoscopic evaluation of non-iron deficiency anemia. There was a retrospective analysis done in a tertiary hospital in Australia which showed similar results as our study.
This study showed that likely cause of anemia was found in iron deficiency anemia when compared to non-iron (21% vs 0%, p<0.001) and that significant change in management was recorded in iron deficiency anemia when compared to other two groups, tissue iron deficiency anemia and anemia of other cause (23% vs 7% vs 6.7%, p<0.0001) [4].
Methods
A single center retrospective chart review was done on all inpatients who were referred for endoscopy, colonoscopy or both, over a period of 5 years. IRB approval was obtained for the retrospective analysis. Exclusion criteria for the study included outpatients, patients with nutritional deficiencies, or unstable patients with active acute gastrointestinal bleeding. Data collected included age, sex, hemoglobin, mean corpuscular volume, Iron, Iron saturation, total iron binding capacity, Ferritin, Endoscopy/ colonoscopy results, and fecal occult blood testing.
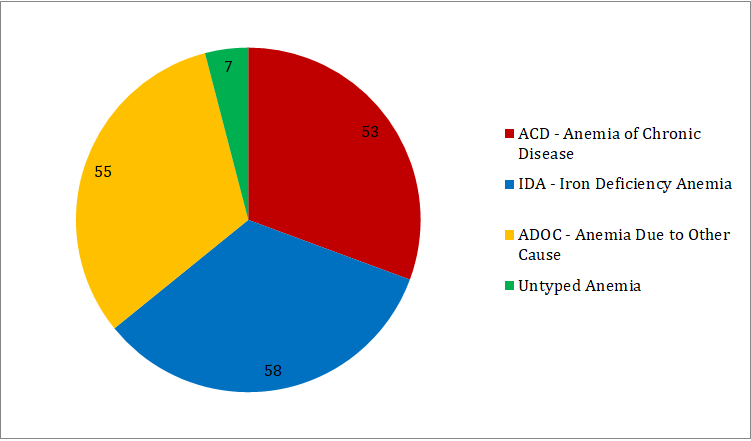
Inclusion criteria was defined as Hgb <13 for males and <12 for females with endoscopy and/or colonoscopy performed as an inpatient at this facility. Patients included in this study were categorized into Iron deficiency anemia (IDA), anemia of chronic disease (ACD) and anemia due to other causes (ADOC), or untyped based upon iron studies, (Figure 1).
Primary outcome included finding a probable cause for gastrointestinal bleed on either endoscopy and/or colonoscopy. Endoscopy was considered positive when lesion described as erosive gastritis, esophagitis, ulcerated polyp, esophageal, gastric or duodenal ulcer, duodenitis, angiodysplasia, arterio-venous malformation, ulcerated polyp, esophageal varices, mass in gastric region, were described. Colonoscopy was considered positive when the following lesions were described: colitis, arterio-venous malformations, ulcerated polyps, diverticulitis, diverticular bleeding and ulcers.
Secondary outcomes included interventions done during the index procedure including photocoagulation, clipping, banding, or epinephrine injection. After the data collection was completed, descriptive statistics were used to calculate averages for Hemoglobin, mean corpuscular volume, and age. Analysis of Variance (ANOVA) was run in all anemia patients with the four categories of IDA, Non-IDA or ADOC, ACD, and untyped to compare findings with significant results at a p-value of less than 0.05.ANOVA was also applied separately to the group in which active bleeding was found upon exam.
To correct for multiple testing, the Bonferroni correction was utilized. This correction is necessary because of the use of several statistical tests being performed at the same time to reduce the number of false positive results. Any results that do not meet the standards of this correction will not be considered significant.
Results
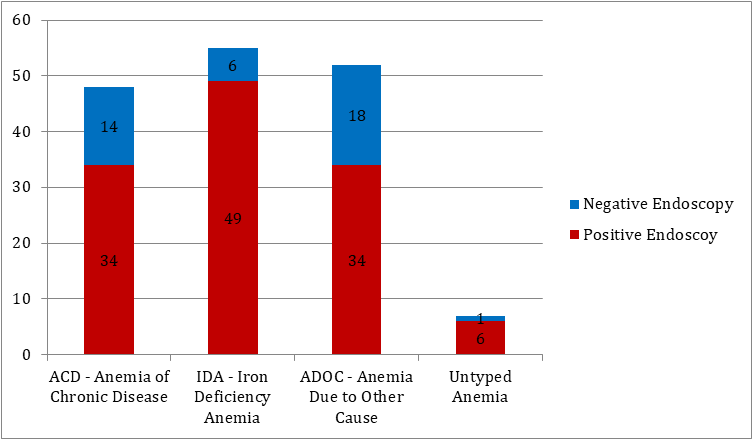
A total of 173 patients were included in the study (see Table 1). Among these there were 58 met criteria for iron deficiency anemia, 53 met criteria for anemia of chronic disease and 55 met criteria for anemia of other causes, depicted in Figure 1. Table 1 is the table that shows the demographic characteristics between the groups and positive endoscopy findings were discovered in 6 patients with untyped anemia, 34 patients with ACD, 49 patients with Iron deficiency anemia, and 34 with non-iron deficiency anemia.
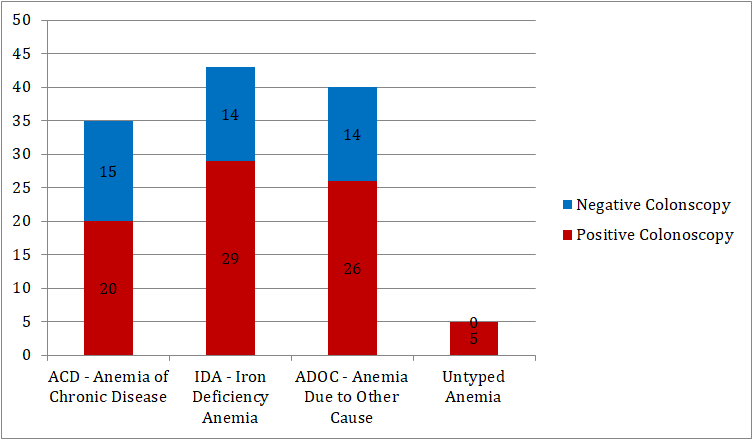
Positive colonoscopy findings were seen in 5 patients with untyped anemia, 20 patients with anemia of chronic disease, 29 patients with iron deficiency anemia, and 26 patients with non-iron deficiency anemia. Also depicted above findings on bar charts in Figures 2 and 3.
| ACD | IDA | ADOC | Untyped | p-value | |
|---|---|---|---|---|---|
| Totals | 53 | 58 | 55 | 7 | 173 |
| Age | 68.55 | 65.19 | 67.05 | 78.57 | 0.085 |
| % Male | 28/53 (52.83%) | 27/58 (46.55%) | 18/55 (32.73%) | 3/7 (42.86%) | |
| Hgb | 8.8321 | 8.2483 | 8.5945 | 9.3286 | 0.266 |
| MCV | 87.76 | 81.91 | 86.62 | 85.03 | 0.133 |
| Endoscopy | 48 | 55 | 52 | 7 | 162 |
| Upper Findings | 34/48 (70.83%) | 49/55 (89.09%) | 34/52 (65.38%) | 6/7 (85.71%) | 0.023 |
| Esophagitis | 5/48 (10.42%) | 5/55 (9.09%) | 6/52 (11.54%) | 1/7 (14.29%) | 0.964 |
| Stricture | 0/48 (0.00%) | 1/55 (1.82%) | 1/52 (1.92%) | 1/7 (14.29%) | 0.077 |
| Gastritis | 16/48 (33.33%) | 21/55 (38.18%) | 20/52 (38.46%) | 2/7 (28.57%) | 0.91 |
| Duodenitis | 3/48 (6.25%) | 4/55 (7.27%) | 3/52 (5.77%) | 1/7 (14.29%) | 0.865 |
| Upper Erosions | 8/48 (16.67%) | 6/55 (10.91%) | 6/52 (11.54%) | 0/7 (0.00%) | 0.589 |
| Vascular | 3/48 (6.25%) | 12/55 (21.82%) | 5/52 (9.62%) | 0/7 (0.00%) | 0.056 |
| Ulcer | 12/48 (25.00%) | 7/55 (12.73%) | 3/52 (5.77%) | 1/7 (14.29%) | 0.052 |
| Mass | 2/48 (4.17%) | 2/55 (3.64%) | 1/52 (1.92%) | 1/7 (14.29%) | 0.448 |
| Clot | 0/48 (0.00%) | 2/55 (3.64%) | 0/52 (0.00%) | 0/7 (0.00%) | 0.272 |
| H. Pylori | Jan-48 | 0/55 (0.00%) | 0/52 (0.00%) | 0/7 (0.00%) | 0.502 |
| Hernia | 0/48 (0.00%) | 4/55 (7.27%) | 0/52 (0.00%) | 1/7 (14.29%) | 0.024 |
| Colonoscopy | 35 | 43 | 40 | 5 | 123 |
| +Colon Findings | 20/35 (57.14%) | 29/43 (67.44%) | 26/40 (65.00%) | 5/5 (100%) | 0.295 |
| Diverticuli | 12/35 (34.29%) | 10/43 (23.26) | 15/40 (37.50%) | 4/5 (80.00%) | 0.066 |
| AV Malformations | 0/35 (0.00%) | 4/43 (9.30%) | 1/40 (2.50%) | 0/5 (0.00%) | 0.177 |
| Hemmorhoids | 2/35 (5.71%) | 7/43 (16.28%) | 5/40 (12.50%) | 0/5 (0.00%) | 0.427 |
| Colitis | 3/35 (8.57%) | 1/43 (2.33%) | 1/40 (2.50%) | 0/5 (0.00%) | 0.462 |
| Polyps | 4/35 (11.43%) | 6/43 (13.95%) | 8/40 (20.00%) | 2/5 (40.00%) | 0.362 |
| C. Difficil | 0/35 (0.00%) | 1/43 (2.33%) | 0/40 (0.00%) | 0/5 (0.00%) | 0.607 |
| Colon Erosions | 0/35 (0.00%) | 3/43 (6.98%) | 0/40 (0.00%) | 0/5 (0.00%) | 0.128 |
| Fissure | 0/35 (0.00%) | 1/43 (2.33%) | 0/40 (0.00%) | 0/5 (0.00%) | 0.607 |
| FOBT | 24/49 (48.98%) | 30/49 (61.22%) | 19/42 (45.24%) | 2/4 (50.00%) | 0.46 |
| 1 Finding | 40/53 (75.47%) | 53/58 (91.38%) | 40/55 (72.73%) | 7/7 (100%) | 0.026 |
| Bleed/Intervention | 4/53 (7.55%) | 10/58 (17.24%) | 0/55 (0.00%) | 1/7 (14.29%) | 0.011 |
| Both Upper/Lower | 32 | 40 | 38 | 5 | 115 |
| U/L Finding | 13/32 (40.63%) | 24/40 (60.00%) | 18/38 (47.37%) | 4/5 (80.00%) | 0.158 |
Table 1: Baseline Characteristics of Patients in the Different Groups of Anemia Including Primary Outcomes Endoscopy and Colonosc
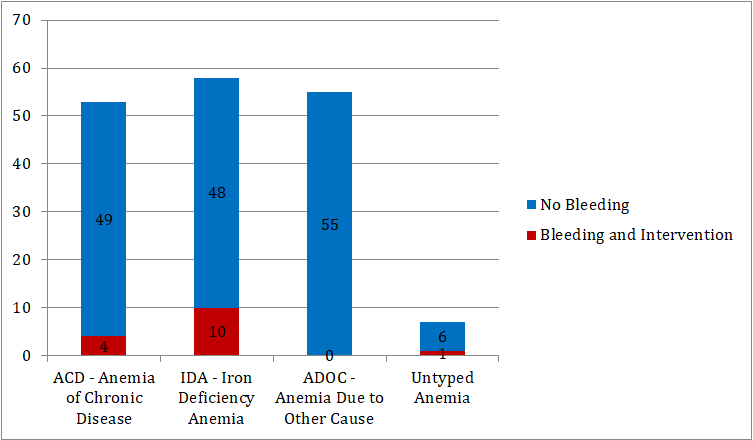
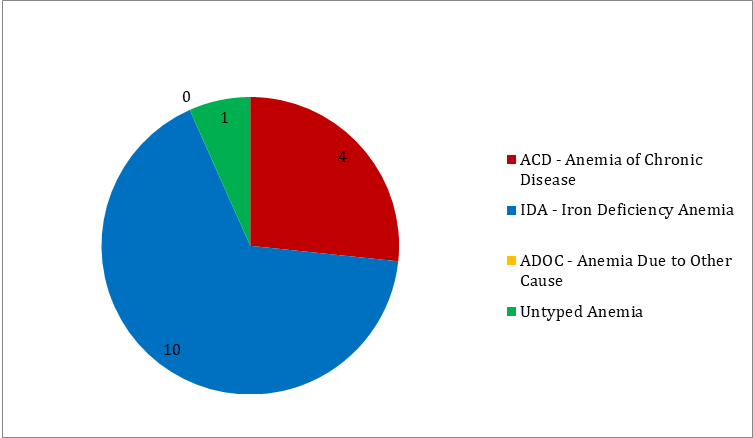
Fifteen patients had active bleeding of which 4 were diagnosed with anemia of chronic disease, 10 with iron deficiency anemia, and 1 with untyped anemia. Among these, 15 patients who needed active intervention, most were among the iron deficiency anemia patients. There were no active interventions done in anemia due to other causes. All these findings depicted in bar chart in Figure 4 and pie chart in Figure 5.
There were no statistically significant differences found in sample means of outcomes among the anemia groups except in categories. In positive endoscopy findings ACD vs IDA vs ADOC vs untyped was 70.83%, 89.09%, 65.38%, and 85.71% respectively with p = .023.For the presence of hernia in endoscopy the means were 0%, 7.27%, 0%, and 14.29% with a p = .024.The examination of positive findings in either endoscopy and/or colonoscopy was 75.47%, 91.38%, 72.73%, and 100% respectively with a p value of .026.Finally, in the presence of active bleeding with active intervention the means of 7.55%, 17.24%, 0%, and 14.29% respectively with a p = .011.
Applying Bonferroni correction adjusts our significant findings to include only the active bleeding and the positive findings. The presence of hernia and positive findings in either endoscopy/colonoscopy are considered non-significant.
| ACD | IDA | ADOC | Untyped | p-value* | |
|---|---|---|---|---|---|
| Totals | 4 | 10 | 0 | 1 | 15 |
| Age | 77.75 | 68.4 | 76 | ||
| % Male | 1/4 (25.00%) | 5/10 (50.00%) | 1/1 (100%) | ||
| Hgb** | 9.9 | 9 | 8.3 | ||
| MCV** | 85.58 | 89.54 | 85.2 | ||
| Endoscopy | 3 | 10 | 1 | 14 | |
| Upper Findings | 3 (100%) | 10 (100%) | 1 (100%) | ||
| Esophagitis | 0/3 (0.00%) | 1/10 (10.00%) | 0/1 (0.00%) | ||
| Stricture | 0/3 (0.00%) | 0/10 (0.00%) | 0/1 (0.00%) | ||
| Gastritis | 2/3 (66.67%) | 1/10 (10.00%) | 0/1 (0.00%) | ||
| Duodenitis | 0/3 (0.00%) | 0/10 (0.00%) | 0/1 (0.00%) | ||
| Upper Erosions | 1/3 (33.33%) | 0/10 (0.00%) | 0/1 (0.00%) | ||
| Vascular | 0/3 (0.00%) | 5/10 (50.00%) | 0/1 (0.00%) | ||
| Ulcer | 1/3 (33.33%) | 2/10 (20.00%) | 0/1 (0.00%) | ||
| Mass | 0/3 (0.00%) | 0/10 (0.00%) | 1/1 (100%) | ||
| Clot | 0/3 (0.00%) | 1/10 (10.00%) | 0/1 (0.00%) | ||
| H. Pylori | 0/3 (0.00%) | 0/10 (0.00%) | 0/1 (0.00%) | ||
| Hernia | 0/3 (0.00%) | 0/10 (0.00%) | 0/1 (0.00%) | ||
| Colonoscopy | 3 | 6 | 0 | 9 | |
| +Colon Findings | 3/3 (100%) | 3/6 (50.00%) | 0 (0.00%) | ||
| Diverticuli | 2/3 (66.67%) | 2/6 (33.33%) | 0 (0.00%) | ||
| AV Malformations | 0/3 (0.00%) | 1/6 (16.67%) | 0 (0.00%) | ||
| Hemmorhoids | 0/3 (0.00%) | 0/6 (0.00%) | 0 (0.00%) | ||
| Colitis | 0/3 (0.00%) | 0/6 (0.00%) | 0 (0.00%) | ||
| Polyps | 0/3 (0.00%) | 0/6 (0.00%) | 0 (0.00%) | ||
| C. Difficil | 0/3 (0.00%) | 0/6 (0.00%) | 0 (0.00%) | ||
| Colon Erosions | 0/3 (0.00%) | 0/6 (0.00%) | 0 (0.00%) | ||
| Fissure | 0/3 (0.00%) | 0/6 (0.00%) | 0 (0.00%) | ||
| FOBT | 2/3 (66.67%) | 6/8 (75.00%) | 1/1 (100%) | ||
| 1 Finding | 4/4 (100%) | 10/10 (100%) | 1/1 (100%) | ||
| Both Upper/Lower | 2 | 6 | 0 | 8 | |
| U/L Finding | 2/2 (100%) | 3/6 (50.00%) | 0 (0.00%) |
Table 2: Secondary Outcome with Positive Endoscopy or Colonoscopy Findings in Patients with Bleeding.
As for the secondary outcome, in the cohort of 15 patients in which active bleeding was found, there was no statistically significant difference between the sample means for ACD, IDA, or untyped anemia See Table 2. There were no reported cases of bleeding associated with ADOC. Results that could be clinically significant include positive endoscopic findings in all patients offered endoscopy, 1 patient was not given endoscopy. Also, majority of the patients with 100% ACD and 50% IDA who were examined with colonoscopy had findings as well. In the patients where both endoscopy and colonoscopy were performed 100% ACD and 50% IDA patients had findings on both exams.
Discussion
Iron deficiency anemia is a major cause of morbidity, and a gastrointestinal tract abnormality is seen in approximately one third of men and postmenopausal women with iron deficiency anemia. There are definitive guidelines published on diagnosing and evaluation of gastrointestinal tract in iron- deficiency anemia patients, but we do not have definitive guidelines on other types of anemia where we do find significant gastrointestinal tract findings. Our retrospective review aimed at finding any gastrointestinal tract causes in other types of anemia as well [5].
Our study revealed that in anemic hospitalized patients without signs of overt gastrointestinal bleeding the likelihood for finding a positive result by endoscopy and/or colonoscopy is substantial and statistically significant between the groups irrespective of the type of anemia. The question this study cannot address is whether this examination was warranted or whether clinical decision making was altered by the results. The lower-than-expected yield of active bleeding in these patients may be an indicator that too many inpatients are offered these procedures at elevated risk and healthcare cost.
Additionally, the results from this study show that active bleeding and the possibility of intervention is very unlikely to be found in any of the anemia types. However, if bleeding is to be found it will most likely occur in iron deficiency anemia. The relationship between iron deficiency and blood loss is clear, but the low number of active bleeds found by endoscopy and/or colonoscopy was not expected. We hypothesized a higher rate of positive bleeding discovered in iron deficient patients. Our cohort examining only the patients with active bleeding seen on exam showed statistically significant results, however, the lack of sample size can be considered a weakness of this study.
In patients that did have active bleed, all patients had positive endoscopic findings whereas only all ACD patients had positive colonoscopy findings. IDA patients with active bleed only had findings on colonoscopy at a rate of 50%.These numbers do not provide the strength of evidence needed to reach any solid conclusions but do hint that active bleeding is more likely on endoscopy in the population studied here.
Endoscopic or colonoscopy findings for different anemias showed no statistically significant difference between the groups except in the case of hernias and untyped anemia. The low number of hernia cases found in this study, make this finding clinically suspect. It is likely that if any statistically significant difference exists between the types of anemia a larger population would be required to find these results.
These findings suggest that the utility of endoscopy and/ or colonoscopy in these patients is limited in the non-urgent inpatient setting. Active intervention is rare and therefore these tests serve little therapeutic value during the inpatient stay. However, if the diagnosis is uncertain, the likelihood of discovering a possible cause is very high in all anemias. We conclude that testing for these patients is warranted only in instances requiring an accurate diagnosis or in cases with a very high suspicion of active bleeding.
This study is not without areas for improvement. Future work on this topic would benefit from a completed analysis including only patients with completed iron studies and hence the removal of the untyped anemia class. The presence of patients that received only one procedure also complicates the ability to generalize the results to the population at large. Additionally, a bigger sample size would provide the needed statistical power to appropriately screen for significant differences of the means between the groups.
Ideally, a prospective study with patients who are screened with iron studies before colonoscopy and endoscopy would provide further information about the likelihood to find probable causes for anemia.
Studies between cohorts of patient demographics including age, race, and gender would also be useful in the future.
Conclusion
In conclusion, analysis of this study shows that a majority of patients with anemia receiving either endoscopy and/or colonoscopy as inpatients have at least one positive finding. However, there is no statistical difference for having positive findings between the different types of anemia. Rates of bleeding in these patients are low and the question of whether to scope these patients must be addressed with further literature.
Acknowledgements
The authors would like to thank and acknowledge the participation and input of Douglas Y. Rowland, Ph.D. of Case Western Reserve University School of Medicine, Department of Population and Quantitative Health Sciences, Cleveland, Ohio regarding the statistical calculations used in this research.
The author reports no conflicts of interest associated with the writing of this article.
Conflict of Interest
Authors declare no conflict of interest
References
-
McLean E, Cogswell M, Egli I, Wojdyla D, De Benoist B (2009) Worldwide prevalence of anemia, WHO Vitamin and Mineral Nutrition Information System, 1993-2005. Public Health Nutrition 12(4): 444-454.
-
Clere-Jehl R, Sauleau E, Ciuca S, Schaeffer M, Lopes A, et al. (2016) Outcome of endoscopy-negative iron deficiency anemia in patients above 65: A longitudinal multicenter cohort. Medicine (Baltimore) 95(47): e5339.
-
Powell N, McNair A (2008) Gastrointestinal evaluation of anemic patients without evidence of iron deficiency. European Journal of Gastroenterology and Hepatology 20(11): 1094-1100.
-
Mogilevski T, Smith R, Johnson D, Charles PGP, Churilov L, et al. (2016) Endoscopic investigation in non-iron deficiency anemia: a cost to the health system without patient benefit. Endoscopy International Open 4(2): E198-E201.
-
Snook J, Bhala N, Beales ILP, Cannings D, Kightley C, et al. (2021) British Society of Gastroenterology guidelines for the management of iron deficiency anemia in adults. Gut 70(11): 2030-2051.
- Ramsay Hunt Syndrome Presenting as Gait Imbalance without Facial Paralysis: A Case Report
- Unveiling Hidden Culprits: An Observational Study of Upper Gastrointestinal Endoscopy Findings in Symptomatic Cholelithiasis Patients
- Assessing Health Care Providers’ Proficiency in International Patient Safety Goals: A Study to Assess the Knowledge &Practice on Patient Safety in a Tertiary Care Teaching Hospital in Gujarat
- Challenges in Diagnosing Child Language Disorders
- Stunting Service Management Model in the South-Central Timor Region, East Nusa Tenggara, Indonesia
- Acute Small Bowel Obstruction Presenting as Gangrenous Jejunal Loop Secondary to Intestinal Endometriosis – A Rare Case Report