Splenic Angle Intussusception – Successful Minimally Invasive Surgery with Intracorporeal Anastomosis
In adults intussusception is rare and accounts for 1% of all bowel obstructions. Colo-colic are less frequent representing less than 25% of all intussusceptions and are more likely to have an underlying malignancy as there is higher prevalence of colonic carcinoma. Less than 10% of intussusceptions in adults are idiopathic. Most of the patients present in the emergency setting with nonspecific symptoms consistent with a partial bowel obstruction. A high index of suspicion is of paramount importance to timely diagnosis and treatment. Although the standard treatment involves surgery, there are controversies regarding reduction of intussusception prior to surgery. Here authors summarize current indications for surgery and describe the first case in the literature of laparoscopic high left colectomy with intracorporeal anastomosis for splenic angle intussusception.
Monteiro EV¹*, Martins M¹, Gaspar B² and Coutinho E³
¹Assistent at General Surgery Service, ULS Póvoa de Varzim-Vila do Conde, Portugal ²Resident at General Surgery Service, ULS Póvoa de Varzim-Vila do Conde, Portugal ³Graduated Assistant and Director of General Surgery Service, ULS Póvoa de Varzim-Vila do Conde, Portugal
Introduction
Intestinal intussusception has been described first in 1674 by Barbette. It is most common in male children from 6 to 18 months and usually is idiopathic in this population and managed nonoperatively [1, 2, 3, 4, 5, 6, 7, 8, 9].
In adults it is rare and accounts for 1% of all bowel obstructions. Mean age is 50 and there is no gender predominance. Of all intussusceptions only 5 % occur in adults [1, 2, 3, 4, 5, 6, 7, 8, 9].
The telescope of a proximal segment of bowel into a distal segment results in bowel obstruction. The exact mechanism is unknown but the lead point alters normal peristaltic bowel activity [1, 2, 3, 4, 5, 6, 7, 8, 9].
Upper gastrointestinal tract is rarely involved in intussusception due to its lack of mobility and fixation.
The most common sites are junctions between freely moving segments and those fixed by adhesions or at the retroperitoneum [3, 9].
Intussusceptions were first classified by location in 1956 by Dean. et al. and usually are divided into entero-enteric 25% , entero-colic 65% and colo-colic 10% [6, 7, 8, 9, 10].
In opposite to children, 90% of adult intussusceptions are caused by an identifiable cause. Virtually any lesion in the bowel wall or lumen that alters peristaltic movements is capable of initiate the invagination [3, 6, 7, 8, 9]. Less frequently intussusceptions are idiopathic (10%) [1, 2, 3, 8, 10].
In small bowel most common lesions are Meckel diverticulum and adhesions; benign tumors such as lymphoid hyperplasia, lipomas, leiomyomas hemangiomas and polyps and other conditions such as anorexia nervosa, infections, supratherapeutic anticoagulation, foreign bodies, malabsorptive, functional, autoimmune and neuroenteric disorders. Less commonly malignant tumors with metastasis (peritoneal carcinomatosis, melanoma) and primary tumors of small bowel such as leiomyosarcoma, adenocarcinoma, GIST, carcinoid, neuroendocrine tumors and lymphoma can act as a lead point [3, 6, 7, 8, 9].
Colo-colic intussusceptions are less frequent representing less than 25% of all and are more likely to have an underlying malignancy (50-75%) as there is higher prevalence of colonic carcinoma. Hemoglobin inferior to 12 g/dl is also an independent predictor of malignancy [5, 6, 9].
Considering colo-colic, colonic adenocarcinoma accounts for 60% of the cases, whereas lipomas are the most common among benign etiology. In ileocolic intussusceptions nearly 100% of the patients have a malignant lead point, cecal adenocarcinoma involving the ileocecal valve [9]. In Central and Western Africa is also described Ibadan or tropical cecocolic intussusception due to dietary habits, microbiome and genetics [9].
Case Report
A 57-year-old otherwise healthy female patient presented to the emergency department with cramping abdominal pain in the lower quadrants, unrelated to meals, lasting about 2 weeks. She described maintained bowel transit but with fluctuations. Laboratory tests showed no significant abnormalities and an abdominal-pelvic CT scan with contrast revealed signs of intestinal intussusception at the splenic flexure of the colon (Figures 1 & 2). An incomplete large bowel obstruction was assumed and the patient was discharged with diet and medical prescription.
She was reevaluated in ambulatory in the same week and submitted to colonoscopy that showed a polypoid, diffusely ulcerated lesion at the splenic flexure occupying the entire lumen. Tattoo was made and biopsies were taken; histology was negative for malignancy.
After complete staging and discussion in an oncology group consultation, it was decided to proceed with surgical treatment. It was performed a laparoscopic high left colectomy with intracorporeal anastomosis. The postoperative period was uneventful, and the patient was discharged.
Histological examination revealed, macroscopically, a prominent formation in the lumen measuring 2.2 x 2.1 x 2 cm with the appearance of invagination and microscopically, a colo-colic intussusception of the mucosa and submucosa, with ulceration and necrosis of the mucosa, but no dysplasia or malignancy (Figure 3).
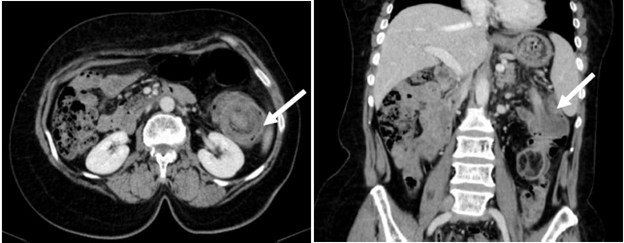
Figures 1 & 2: Pre-Operative CT Showing Colo-Colic Intussusception (White Arrows).

Discussion
Intussusception is uncommon in adults and few clinicians have seen one in their surgical career; a high index of suspicion is of paramount importance as most of the diagnosis are made only intraoperative [6, 7].
In adults, most patients present in the emergency setting with nonspecific symptoms consistent with partial obstruction. Symptoms are usually acute from days to weeks but might be chronic, with years of duration [9].
The most common presentation includes abdominal pain, nausea, vomiting, change in bowel habits and gastrointestinal bleeding. Abdominal masses are palpable in less than 40% of adult patients and the identification of a mass during the episode is suggestive of intussusception [1, 2, 3, 5, 9].
The classic triad of abdominal pain, palpable mass and bloody stool in children is very rare in adults and even in children is only present in 15-50% [3, 7, 8, 9, 10].
If patient presents late in the course of the disease there might be signs of bowel ischemia or peritonitis and patient presents with signs of septic shock [9]. Complementary diagnostic studies are extremely helpful in diagnosis.
Laboratory tests usually show elevated white blood cell count and nonspecific inflammatory markers such as thrombocytosis and elevated C reactive protein [9].
Workup includes plain films of the abdomen that might show signs of bowel obstruction and its level or perforation; unfortunately they lack sensitivity and specificity for the diagnosis of intussusception [9]. Ultrasound sensitivity and specificity is almost 100% in experienced hands however accuracy might be reduced because of dilated bowel loops and in the morbidly obese patients [8, 9, 10].
The gold standard in diagnosis is CT scan that has a diagnostic accuracy of 58-100% [2, 4, 5, 10]. CT provides information about intussusception location and status and width of the intestinal segment involved. Besides this it might not provide enough information about the presence and characteristics of an organic lesion [4, 6, 8].
In adults the safety of CT leads to nowadays most commonly seen nonpathological transient short segment intussusception [1, 9, 10]. Classic findings include “target”, “bull-eye” or “sausage” shaped lesions characterized by a hyperdense double ring; additionally there can be signs of thickened segment of bowel, impaired perfusion and ischemia [8, 9].
Although rarely used, MRI enterography has similar accuracy as CT and is useful in pregnant patients [3, 4, 9, 10].
Barium or water soluble contrast enema often reveals a “cup shaped” filling defect and has therapeutic potential particularly in idiopathic intussusceptions; it is contraindicated if there is suspicion of ischemia or perforation. In children since most intussusceptions are ileo-colic, pneumatic or hydrostatic decompression can be successful in 80-90% of patients [7, 9, 10].
Timely diagnosis and treatment are essential to prevent progression of the disease and complications.
In adults, as the presentation is vague and nonspecific, preoperative diagnosis and treatment is difficult and most diagnosis are established in the operating room during surgery [1, 4, 5].
In the era of the accidental non pathological CT intussusceptions there are three main indications for surgery: bowel obstruction, lead point on the CT and ileocolic or colo- colic intussusceptions; also non reducible intussusceptions and progression of the disease to ischemia and perforation are indications for emergent surgery [9].
The laparoscopic approach seems safe and effective in confirming the diagnosis and treatment [4, 7, 9].
Although the standard treatment involves surgery, there are controversies regarding reduction of intussusception prior to surgery [4].
In idiopathic intussusception reduction can be attempted to limit the extent of bowel resected however if the patient does not have a prior total colonoscopy with ileoscopy it is difficult to categorize the intussusception as idiopathic; also colonoscopy is useful to biopsy and to exclude synchronous lesions.
Reduction can be considered if there is evidence of benign etiology in colonoscopy and with less evidence in pediatric patients, entero-enteric intussusception and posttraumatic or postoperative intussusception regarding the lower risk of malignancy [3, 4, 5]. As a matter of fact, in patients with a pathological lead point reduction exposes the patient to perforation, dissemination of malignancy and increased anastomotic complications so it should be decided case by case [2, 3, 5, 9]. In adults since there is a 65% risk of malignancy regardless of the anatomic site, en bloc resection is often recommended [2, 5, 6].
Surgical approach varies according to the location of the intussusception, status of the bowel and presence or absence of an organic lesion. 4,8 Advantages of laparoscopic approach include reduced patient surgical stress and ileus, improved cosmetic appearance, shorter hospital stay and quick return do daily routine [4].
To data there are few case series about laparoscopic treatment of intussusception and in none is described high left colectomy with complete mesocolic excision and central vascular ligation with intracorporeal anastomosis to treat splenic angle intussusception [4, 11].
Conclusion
Intussusception is a rare cause of large bowel obstruction, and it is even rarer when due to a benign cause, as in this case. Considering this, surgeons must be familiar with etiology and diagnosis as a thorough history, appropriate investigation and timely intervention can ensure safe patient outcomes.
Continued research and case documentation will be essential to further understand this uncommon condition and refine treatment protocols. Our successful experience with minimally invasive surgery and intracorporeal anastomosis demonstrates that these advanced techniques can be effectively employed.
References
-
Frazier A, Mbah R, Williams JT (2022) Rare Idiopathic Adult Intussusception: A Case Report. Cureus 16(1): e52022.
-
Salam A, Chikr B, Barghash M, Mansour M (2024) 1044 Colo-Colic Intussusception with Large Bowel Obstruction in Adults. British Journal of Surgery 111(6).
-
Amoruso M, D’Abbicco D, Praino S, Conversano A, Margari A (2013) Idiopathic adult colo-colonic intussusception: Case report and review of the literature. Int J Surg Case Rep 4(4): 416-418.
-
Yüksel A, Coşkun M (2021) Laparoscopic surgery for adult intussusception: Case Series. Turkish J Gastroenterol 32(8): 611-615.
-
Wilson A, Elias G, Dupiton R (2013) Adult colocolic intussusception and literature review. Case Rep Gastroenterol 7(3): 381-387.
-
Frazão J, Silva C, Almeida F, Calado J, Mira P (2023) Adult Colocolic Intussusception: A Rare Case of Intestinal Obstruction. Cureus 15(5): e39526.
-
Gange ER, Grieco MA, Myers SD, Guenther TM (2020) Idiopathic adult intestinal intussusception: A rare cause of an acute surgical abdomen. J Surg Case Reports 2020(12): 1-3.
-
Deshpande S, Satarkar R, Kulkarni D (2022) Intussusception in Adults : Rare but Grievous Disease. Annals of Clinical Case Reports 7(2124): 1-3.
-
Marsicovetere P, Ivatury SJ, White B, Holubar SD (2017) Intestinal Intussusception: Etiology, Diagnosis, and Treatment. Clin Colon Rectal Surg 30(1): 30-39.
-
Stefano CD, Salvatori E, Savino L, Forte V, Paoletti S, et al. (2024) Colo-colic intussusception in an adult caused by lipoma: Case report of a rare condition. Radiol Case Reports 19(2): 665-670.
-
Hakim T (2022) Adult intussusception due to ileal polyp-A case report. Int J Surg Case Rep 99: 107554.
- Ramsay Hunt Syndrome Presenting as Gait Imbalance without Facial Paralysis: A Case Report
- Unveiling Hidden Culprits: An Observational Study of Upper Gastrointestinal Endoscopy Findings in Symptomatic Cholelithiasis Patients
- Assessing Health Care Providers’ Proficiency in International Patient Safety Goals: A Study to Assess the Knowledge &Practice on Patient Safety in a Tertiary Care Teaching Hospital in Gujarat
- Challenges in Diagnosing Child Language Disorders
- Stunting Service Management Model in the South-Central Timor Region, East Nusa Tenggara, Indonesia
- Acute Small Bowel Obstruction Presenting as Gangrenous Jejunal Loop Secondary to Intestinal Endometriosis – A Rare Case Report