Outcome of Intra-Articular Fractures of the Distal End of the Radius Managed Using Volar Variable Angle Locking Plate
Background: Distal radius fractures are one of the most common fractures of human skeleton. Despite advances in management of these fractures a consensus regarding the best treatment protocol is still lacking. Methods: This prospective study involved 20 patients (13 males; 7 females) who presented with fractures of distal end radius. There were three B3 (29%), six C1 (35.5%) & eleven C2 (9.7%) fractures according to AO classification system. The mean age was 36.39 years and the mean follow up was 2.4 years. At the time of final evaluation outcome was assessed as per Gartland and Werley scoring system. Statistical assessment was done using Chi-square test and p values were obtained at final follow up. Results: All fractures healed within a mean period of 10 weeks ranging from 8 to 14 weeks. At the time of final follow up pronation were 81.380, supination 86.340 degrees, palmar flexion 58.030, dorsiflexion 61.930, radial deviation 19.210& ulnar deviation 31.320. Radiological parameters as measured at final evaluation were: volar tilt 5.76 degrees, radial inclination 19.10 degrees & ulnar variance -0.42 mm. As per Gartland and Werley score, 85% had excellent outcome, 5% good, 5% fair and 5% had poor outcome. Two patients had complications, one complained of screw impingement for which implant removal was done at 12 months after surgery while other patient developed Sudeck’s osteodystrophy which was managed conservatively. Conclusion: Variable angle locking plate is a reliable implant associated with good outcome in intra-articular fractures of the distal end of the radius.
Introduction
Distal radius fractures account for one sixth of all the fractures presenting in the emergency room [1]. They contribute to considerable disability, increased dependence for the injured patient and pose a major challenge to the health care system [2]. The pediatric and the elderly population are at greatest risk for this injury [3]. Described in 1814 by Abraham Colles, controversies, however still exist regarding the mode of treatment and literature has failed to create a consensus on the appropriate line of management [4, 5]. Reconstruction of articular congruity and restoration of the radial length, volar angulation and radial inclination have become prerequisite for a good clinical outcome [6, 7]. Recent advances in evaluation of fracture patterns and results of treatment have demonstrated the need for surgical intervention in fractures demonstrating instability with or without articular incongruity [5, 8, 9]. Locking compression plates in distal end radius fracture provides angular and axial stability, minimizing the possibility of screw loosening and back out which prevents the secondary displacement of unstable fractures& also avoiding possible deprivation of blood supply to the distal metaphyseal fragments [6, 7, 9, 10, 11, 12, 13]. In view of the above- mentioned advantages, the present prospective study was done to evaluate the role of Variable Angle locking compression plates in treatment of fractures of distal end of radius.
Methods
The present prospective study involved 20 patients of either sex (13 males & 7 females) more than 18 years of age presenting with fractures of distal end radius with a mean age 36.39 years between November 2013 to January 2015. Sixteen patients had involvement of left side while 4 patients had involvement of right side. Road traffic accident was observed to be the most common mode of injury accounting for 71.42% of the cases & fall on outstretched hand accounting for rest. Patients with incomplete fractures, undisplaced fractures, fracture with previous or existing infection in forearm, open fractures and patients who refused consent were excluded from the study. Standard antero-posterior and lateral x-rays of wrist were done to know the personality of fracture & fractures classified according to AO classification. There were three B3 (29%), six C1 (35.5%) & eleven C2 (9.7%) fractures according to AO classification system. The average time to surgery was 9.64 days (range 2-30 days). Associated non-bony injuries were present in one patient, who had facial injuries & other bony fractures were observed in 4 patients including fractures of olecranon in two patients and fractures of femoral shaft in other two.
All surgical interventions were done either using regional block (supraclavicular) or general anaesthesia under tourniquet control. Volar approach was used for all fractures and Fracture reduction was done and checked under image intensifier. Synthes Titanium Variable angle locking compression plate (VALCP) was used to fix all 20 fractures. Postoperative immobilization was done by giving below elbow plaster of paris (POP) back slab, if required according to per operative assessment of stability of fixation. Patient’s limb was kept elevated, watched for distal circulation and was instructed to perform active finger movements. Patients were discharged at appropriate time with the instructions to perform active finger movements and limb elevation. Stitch removal was done at 2 weeks and patients were examined for soft tissue healing and any signs of infection. Plaster of Paris back support was removed or continued subjected to stability of fixation and patients were advised to do active wrist physiotherapy exercises. Patients were followed up weekly for first two weeks and then after every two weeks for the next 3 months & on monthly basis for a minimum of 2 years. Standard antero-posterior and lateral x-rays of wrist were done at 2 weeks, 4 weeks and every month till 6 months to assess bony union and 6 monthly thereafter. At the time of final evaluation outcome was assessed as per Gartland and Werley scoring system. Radiological assessment was done at final evaluation which included measurement of volar tilt, radial inclination and ulnar variance. Statistical assessment was done using Chi-square test and p values were obtained at final follow up.

Results
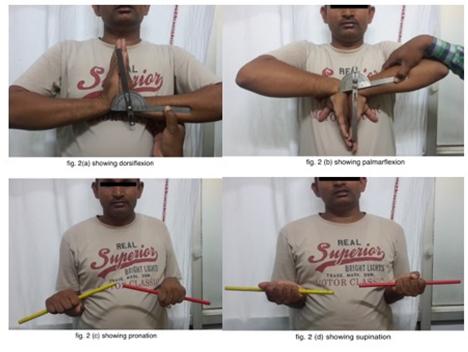
All fractures healed within a mean period of 10 weeks ranging from 8 to 14 weeks. Average Range of motion as achieved in the present study was: Pronation 81.380(p<0.001), supination 86.340 (p<0.001), palmar flexion 58.030, dorsiflexion 61.930, radial deviation 19.210& ulnar deviation 31.320. Radiological parameters as measured at final evaluation were: volar tilt 5.76 degrees, radial inclination 19.10 degrees & ulnar variance -0.42 mm. Out of 20 patients, 18 patients had final score between 0 to 5 which was statistically significant (p<0.001), one patient had score between 6 to 10 and other between 11 to 15 according to the Gartland and Werley scoring sytsem. In the present study out of 20 patients, 17 patients (85%) had excellent outcome, which was statistically significant (p<0.001), 1 patient (5%) had good outcome, 1 patient (5%) had fair outcome and 1 patient (5%) had poor outcome. Two patients (10%) developed complications in the present study. one of the patients complained of screw impingement for which implant removal was done after 12 months of surgery while other patient developed Sudeck’s Osteodystrophy which was managed conservatively. There was no case of any infection, tendon ruptures, nerve injury, vessel injury, and non-union or implant failure observed in the present study.
Discussion
The fractures of distal end radius are among the most common fractures. However, the management has always been a debatable and challenging issue for orthopaedic surgeons. The ultimate goal is to achieve proper reconstruction of disrupted anatomy and allow quick return of function without complications. The results of conservative management of these fractures have historically been unsatisfactory and many studies have reported better results with operative management. As a result conservative treatment is generally reserved for patients with minimally displaced fractures or for those who could not bear the stress of surgery. Also, the conventional fixation techniques like K-wires and external fixators have their own share of problems. Locking plates offer an attractive alternative for management of these fractures due to possibility of a more stable construct on account of angular stability of locking screws. Additional possible advantages of these plates include, decreased soft tissue complications and absence of secondary displacement of fracture fragments even in the absence of adequate contouring of plates [14, 15, 16]. The present study was therefore conducted in a prospective manner to evaluate the role of locking compression plates in distal end radius fractures. Volar approach was used in the present study for the fixation of fractures in all the patients. Volar approach has decreased risk of inducing soft tissue complications, as the dorsal approach often needs dissection of the extensor retinaculum and sometimes resection of the Lister’s tubercle leading to mechanical attrition of the extensor tendons by plates and screws. On the other hand, volar anatomy of the wrist offers an advantage over the dorsal aspect, as there is more space between the volar cortex and the flexor tendons and pronator quadratus acts as a hedge to prevent soft tissue complications [14]. Minegishi et al have also used the volar approach in all their cases while Kwan et al used dorsal approach in only 9% of cases where the articular reduction could not be achieved through volar approach [14, 16]. In the present study, mean ulnar variance was - 0.42 mm (p=.066). In the study conducted by Kilic, et al. ulnar variance was equalized in 21 patients (77.8%), and in 6 patients (22.2%), a mean positive ulnar variance of 0.4 mm (range 0-3) was observed [17]. Mean radial inclination as observed in the present study was 19.10 degrees (p<.001) and was statistically significant & comparable to the study done Kilic, et al. [17]. Mean volar tilt in the present study was 5.76 degrees (p=.066), which is comparable to the mean volar tilt of 5 degrees in the study done by Kwan, et al. [15]. In the present study at final follow up the mean dorsiflexion was 61.93 degrees (p=.078) and the mean palmarflexion was 58.03 degrees (p=.056) similar to reported by Minegishi et al and Kwan et al [14, 16]. Mean supination was 86.34 degrees (p<.001) and mean pronation was 81.38 degrees (p<.001), which were statistically significant and similar to the study done by Kwan, et al. [16]. The mean ulnar deviation as observed in the present study was 31.32 degrees (p=.009) and the mean radial deviation was 19.21 degrees (p<.001), which were statistically significant. In the study done by Kilic, et al. they reported statistically significant difference between pre and post operative radial tilting angles, inclination angles and radial height with the use of volar locking plates and reported that poor functional outcomes were associated with poor radiological outcomes as measured by Stewart radio graphical scores [17]. Similarly in the present study, better radiological outcomes were associated with good functional outcomes and there was a trend towards decreased improvement in range of motion activities with increasing age as reported by Kwan, et al.[16] Complications were reported in 2 of the patients (10%) in the present study. No nonunion, loss of reduction or infection was reported in the present study. Minegishi et al reported complications in 3 of their patients managed with volar locking plates, which included slight finger contraction in 2 patients and attrition rupture of flexor tendon in 1 patient, which was managed with tendon repair [14]. Kwan13 et al reported complications in 10 of their patients managed with volar locking plates [16]. Final results as reported by Kilic et al in their study were excellent to good in 89.9% patients and moderate to poor in 11.1% patients according to Gartland and Werley system [17]. Similar results were obtained in the study done by Kwan, et al. [16]. In the present study excellent to good results were obtained in 85% of the patients. One of the patients had a fair outcome while the other patient had poor outcome due to decreased range of motion and persistent pain in the distal radio-ulnar joint. Both the patients were managed conservatively and reported improvement in symptoms. Therefore, results obtained in the present study are similar to the results reported in the studies mentioned above. The observations of the present study therefore do indicate that use of variable angle locking compression plates in the management of distal end radius fractures provides stable fixation for early mobilization of patient, leading to early resumption to pre-trauma functional level of an individual. It is likely to provide angular stability thereby preventing risk of secondary displacement. Minor deficiency in anatomic reduction may not result in significant functional compromise; however, significant variation in anatomy (post reduction) may result in possible osteoarthritis at an early stage beside cosmetic deformity being unacceptable. However, it goes without saying that there is no doubt of desirability of anatomic reduction of these fractures. Therefore, a comparative study involving comparison of these implants with conventional techniques may put possible advantages of these implants on a firmer footing. Long term follow up studies may also be required to evaluate the long-term effects of these plates. Despite this our results are encouraging and add to the growing body of evidence in favor of open reduction and internal fixation of distal radius fractures using a volar locking plate construct.
References
-
Walencamp M, Bentohami A, Beerekamp M, Peters R, Heiden R, et al. (2013) Functional outcome in patients with unstable distal radius fractures, volar locking plate versus external fixation: a meta-analysis. Strat Traum Limb Recon 8(2): 67-75.
-
Dillingham C, Horodyski M, Struk A, Wright T (2011) Rate of improvement following volar plate open reduction and internal fixation of distal radius fractures. Adv Orthop 1-4.
-
Nellans K, Kowalski E, Chung K (2012) The epidemiology of distal radius fractures. Hand Clin 28(2): 113-125.
-
Phadnis J, Trompeter A, Gallagher K, Bradshaw L, Elliot D, et al. (2012) Mid-term functional outcome after the internal fixation of distal radial fractures. J Orthop Surg Res 7: 4-11.
-
Ilyas AM, Jupiter JB (2007) Distal radius fractures- classification of treatment and indications for surgery. Orthop Clin North Am 38(2): 167-173.
-
Wong KK, Chan KW, Kwok TK, Mak KH (2005) Volar fixation of dorsally displaced distal radial fracture using locking compression plate. J Orthop Surg (Hong Kong) 13(2): 153-157.
-
Gogna P, Selhi HS , Singla R, Mohindra M, Batra A, et al. (2013) Osteosynthesis with long volar locking plates for metaphyseal-diaphyseal fractures of the distal radius. Chin J Traumatol 16(6): 339-343.
-
Knirk JL, Jupiter J (1986) Intra articular fractures of the distal end of the radius in young adults. J Bone Joint Surg Am 68(5): 647-659.
-
Trumble TE, Schmitt S, Veddar NB (1994) Factors affecting functional outcome of displaced intra articular distal radius fractures. J Hand Surg A 19: 325-340.
-
Smith WR, Ziran BH, Anglen JO, Stahel PH (2007) Locking Plates: Tips and Tricks. J Bone Joint Surg Am 89(10): 2298-2307.
-
Sommer C, Gautier E, Muller M, Helfet DL, Wagner M (2003) First clinical results of the Locking Compression Plate (LCP). Injury 34(2): B43-54.
-
Wagner M (2003) General principles for the clinical use of the LCP. Injury 34(2): 31-42.
-
Martineau PA, Berry GK, Harvey EJ (2007) Plating for Distal Radial fractures. Orthop Clin N Am 38(2):193- 201.
-
Minegishi H, Dohi O, An S, Sato H (2011) Treatment of unstable distal radius fractures with the volar locking plate. Ups J Med Sci 116(4): 280-284.
-
Gogna P, Selhi HS, Singla R, Devgan A, Magu NK, et al. (2013) Dorsally Comminuted Fractures of the Distal End of the Radius: Osteosynthesis with Volar Fixed Angle Locking Plates. ISRN Orthop 2013: 131757.
-
Kwan K, Lau T, Leung F (2011) Operative treatment of distal radial fractures with locking plate system-a prospective study. IntOrthop 35(3): 389-394.
-
Kilic A, Kabukcuoglu Y, Ozkaya U, Gul M, Sokucu S, et al. (2009) Volar locking plate fixation of unstable distal radius fractures. Acta Orthop Traumatol Turc 43(4): 303-308.
- Return to Work Among Manual Workers After the Latarjet Procedure: A Cohort Study of 43 Patients
- Refractory Pelvic Collection Following Modified Stoppa Approach for Both-Column Acetabular Fracture Fixation: A Case Report
- Comparative Study of Dynamic Knee Phenotypes Under Loaded and Unloaded Conditions: Clinical Impact
- Locked Intramedullary Nailing of the Tibia Using a Humeral Nail: A Care Case Report
- Subtalar Dislocation: About a Case Report
- Surgical Site Infection in Orthopedics in a Country with LimitedResources: Indications, Treatment and Results