Large Cell Neuroendocrine Carcinoma of The Lung with Skin Metastasis and Multiple Metachronous Primaries
A case of large cell neuroendocrine carcinoma of the lung with multiple cutaneous metastases as the primary manifestation is presented. It was the third metachronous primary following testicular seminoma and prostate adenocarcinoma.
Introductıon
Multiple primary malignancies (MPMs) are defined as a diagnosis of two or more primary tumors that are independent from each other in a patient. Three conditions must be provided so as to define MPMs: (I) tumors should be different from each other; (II) tumors should have the features of malignancy and (III) one should not be the metastasis of the other. MPMs are divided into two groups according to the time of diagnosis. If the tumors are diagnosed within a 6-month interval, they are called synchronous. If the second primary malignancy is diagnosed 6 months after or more it is named as metachronous [1]. Both the side effects of treatment and increase in survival as a treatment successas well as other risk factors bring up other primary cancers. Our patient had the diagnosis of with triple primary metachronous malignancies consisting of testicular seminoma, prostate adenocarcinoma and large cell neuroendocrine carcinoma(LCNEC) of the lung with multiple cutaneous metastases. To the best of our knowledge, this combination of primary tumors has not previously been reported. Likewise, cutaneous metastasis of LCNEC is a rare presentation.
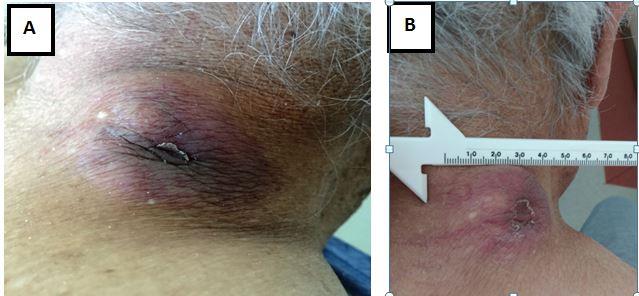
A 83-year-old man presented with a recent onset of asymptomatic skin nodules in the neck, body front and back. He had 70 pack/year of smoking history and chronic obstructive pulmonary disease. His mother had colon cancer. Past medical history dates back to 1987 when he was diagnosed as metastatic testicular seminoma following left orchiectomy and was treated with chemotherapy. In 2010 he developed prostate cancer. He had a prostate-specific antigen (PSA) level of 65 ng/ml in a routine evaluation. Abdominal CT scans demonstrated enlargement and calcification of the prostate without any evidence of nodal or visceral metastasis. Also, there was no bone metastasis on bone scan. Because he refused surgery and radiotherapy the patient received combined androgen blockade with luteinizing hormone-releasing hormone(LHRH) agonist and bicalutamide. One month later his PSA value was down to 0,6 ng/dl. He remained well and asymptomatic until March 2016 when he was admitted to urology department with multiple nodules localized in the skin of the neck, back and front of the body. He was taking bicalutamide 50 mg/day, tamsulosin 0,4 mg/day and tiotropium bromide 18 mcg/day. The firm nodule on the neck was measuring 36X48 millimeters in greatest dimension, was round and dark-colored with telangiectasias (Figure 1). Computed tomography of the thorax demonstrated multiple metastatic lesions in both lungs and a left hilar mass. Abdomen CT revealed multiple lesions measuring up to 30 millimeters in bilateral perirenal areas and mesentery as well as several subcutaneous nodules on the abdominal wall. An excisional biopsy was performed from the chest wall nodule. Pathological assessment of biopsy material revealed an infiltrative neoplasm with organized growth pattern. The tumor was composed of small to medium- sized cells with moderate amount of cytoplasm. Rosette formation has not been observed in the tumor. Microscopic necrotic foci in the tumor were evident. Mitotic activity was about 20 per ten high power field. Immunohistochemical analysis showed that TTF-1, CK7, synaptophysin, CD56 and Chromogranin were expressed on tumor cells. CK20, Napsin A, PSA and pSMA expression were not detected. Along with histological and immunohistochemical findings, current case was interpreted as “Large cell neuroendocrine carcinoma" metastasis with lung origin. A 18F-FDG PET revealed hypermetabolism in left hilar mass and skin and intra abdominal lesions(SUVmax:12.4, 8.1 and 9.2 respectively). Also there were multiple hyper metabolic lesions in the pelvis and left acetabulum(SUVmax::7.8) He subsequently underwent chemotherapy. The patient was treated at three-week intervals with 800 mg/m2 of gemcitabine (30-min intravenous infusion on days 1 and 8) plus 150 mg/m2 of carboplatin (15-min intravenous infusion on day 1) starting in March 2016. He received six cycles of this chemotherapy, ending in July 2016. Following the first 3 cycles, the nodule on his neck decreased to 29x21 mm in size, with a response in other nodules also. Likewise, a CT scan of the chest showed that left hilar mass was responding to chemotherapy. However, lesions progressed one month following the 6th cycle and the patient was crossed over to docetaxel 70 mg/m2 every 3 weeks. He is still alive and doing well in November 2016, following the third cycle of docetaxel.
Discussion
Testicular seminoma is a germ cell tumor is curable even at late stages [2]. Our patient remained well following chemotherapy for metastatic seminoma given 29 years ago. Later he had 2 other metachronous malignancies including prostate cancer and LCNEC of lung which presented as metastatic skin nodules. Multiple mechanisms have been involved in the pathogenesis of metachronous malignancies including hereditary, immune and environmental factors [3]. Also, chemotherapy is thought to increase the emergence of other primary tumors. This patient was a heavy smoker which may also be responsible for developing other primaries. Likewise, prostate cancer is the second most common cancer in men worldwide [4]. Neuroendocrine tumors (NET) category constitutes an important and distinct group of primary lung neoplasms. To be classified as NET, a tumor should have neuroendocrine histological features as well as ultrastructural or molecular signs of neuroendocrine differentiation. In a case of cutaneous metastasis of neuroendocrine carcinomas (NEC), the key point of histopathology is to distinguish it from Merkel cell carcinoma. This distinction is important for the patient's prognosis. For routine pathological assessment, expression of mainly CD56 (NCAM), chromogranin or synaptophysin on tumor cells are strong evidence of neuroendocrine differentiation. The current patient has strong unequivocal CD56 and chromogranin expression on tumor cells. These features provide sufficient evidence for neuroendocrine differentiation. There are four groups for NEC in current WHO classification. These are typical carcinoid, atypical carcinoids, large cell NEC and small cell lung cancer(SCLC). The distinction of these lesions is based mainly on morphological microscopic analysis since immunohistochemical expression is of limited help for differential diagnosis of neuroendocrine tumors of the lung. Tumors with small cell morphology should be categorized as SCLC whereas a tumor with non-small cell cytological features and higher mitotic activity is classified as large cell NEC as in our case. To identify the origin of a large cell neuroendocrine carcinoma metastasis, expression of tissue-specific gene related transcription factors and tissue-specific cytokeratins on tumors may be of help. Tissue-specific gene expression is usually mediated by transcription factors. Of these factors, Thyroid transcription factor (TTF-1) is present on terminal respiratory unit throughout the life span and morphogenesis of lung. In addition, the TTF-1 expression is usually maintained in primary lung neoplasms. So TTF-1 is considered as a lineage marker for lung parenchyma. Cytokeratin expression (mainly CK7 and 20) has also been utilized to identify the origin of metastatic tumors. Even though cytokeratin profile cannot give specific information as much as tissue-specific transcription factors do, they may identify broadly the epithelial tract where the tumor may be originated (such as gastrointestinal, urinary, respiratory tract etc.). Metastatic tumor in current case has TTF-1 and CK7 expression but no CK20 and PSA. We interpret these immunohistochemical findings as they are compatible with a lung primary. Life expectancy, especially in cases of distant metastasis is as short as 6 months. While most patients respond to chemotherapy, early relapse or resistance to therapy is usually observed. Even then our patient responded our patient responded he is doing well and alive after 6 cycles platinum-based chemotherapy plus 2 cycles of docetaxel regimen. Because LCNEC is scarce clinical situation, there is limited experience in the treatment approach. It is usually treated as small-cell lung carcinoma (SCLC) [5]. The response of platinum-based treatment compared to non-platinum-based chemotherapy was found to be superior by Sun, et al. [6]. They also examined that the agents used in the treatment of SCLC should be preferred in the treatment of advanced LCNEC. Both Tokito and Igawa reported that chemotherapy effectiveness was similar between extended SCLC and advanced LCNEC [7, 8]. As mentioned before we used relatively low dose of platinum-based chemotherapy. The treatment was well tolerated and the patient's performance status improved. Progression occurred shortly after the last cycle of chemotherapy which indicated a poor prognosis. However, there was a response to docetaxel treatment observed before administration of the second one with reduction of the dimentions of left hilar mass and skin lesions. Our patient had three metachronous primary malignancies and the last one is very rare. Only two cases of multiple cutaneous metastases of LCNEC have been reported in the literature [9, 10]. Also, this is first case of three primary malignancies which include pulmonary LCNEC with multiple cutaneous metastases in the literature which makes it intersting. Further studies using new drugs are required to find out treatments with higher activitity in metastatic LCNEC
References
-
Bhamidipati PK, Ribbeck A, Liaghati-Nasseri G, Kumar R, Paidipaty BB, et al. (2011) An atypical presentation with diagnostic challenge of a large cell neuroendocrine cancer of lung: a case report and review of the literature. Lung Cancer Int 912098.
-
Testicular cancer. Midline Plus.
-
Warren S (1932) Multiple primary malignant tumors. Am J cancer 16: 1358-414.
-
Humphrey P, Schuz J (2014) Cancers of the male reproductive organs. World Cancer Report Lyon: World Health Organization 453-464.
-
Graziano SL, Mazid R, Newman N, Tatum A, Oler A, et al. (1989) The use of neuroendocrine immunoperoxidase markers to predict chemotherapy response in patients with non-small-cell lung cancer. J Clin Oncol 7(10): 1398-1406.
-
Sun JM, Ahn MJ, Ahn JS, Um SW, Kim H, et al. (2012) Chemotherapy for pulmonary large cell neuroendocrine carcinoma: similar to that for small cell lung cancer or non-small cell lung cancer? Lung Cancer 77(2): 365-370.
-
Tokito T, Kenmotsu H, Watanabe R, Watanabe R, Ito I, et al. (2014) Comparison of chemotherapeutic efficacy between LCNEC diagnosed using large specimens and possible LCNEC diagnosed using small biopsy specimens. International journal of clinical oncology 19(1): 63-67.
-
Igawa S, Watanabe R, Ito I, Murakami H, Takahashi T, et al. (2010) Comparison of chemotherapy for unresectable pulmonary high-grade non-small cell neuroendocrine carcinoma and small-cell lung cancer. Lung Cancer 68(3): 438-445.
-
Mestre T, Rodrigues AM, Cardoso J (2015) Pulmonary large-cell neuroendocrine carcinoma presenting as multiple cutaneous metastases. J Bras Pneumol 41(3): 289-291.
-
Pajaziti L, Hapçiu SR, Dobruna S, Hoxha N, Kurshumliu F, et al. (2015) Skin metastases from lung cancer: a case report. BMC research notes 8: 139.
- Cancer Diagnosis from RNA Sequence of Blood Cells by Using AI
- Field Cancerization in Oral Cavity, Case Report and Review of Literature. Oncologic Program Salud Integral Hospital, Managua, Nicaragua
- Identification of B Lymphocytes in Cancer Patient’s Blood
- A Case Report of a Breast Cancer Patient Developing Pneumonitis as a Result of Abemaciclib Therapy
- Immune Checkpoint Therapeutics for Today’s Fight and Beyond
- The Amalgamated Sophomore-Gonadoblastoma