DPYD IVS14+1 G>A Polymorphism in Colorectal Cancer in Western India
5-fluorouracil (5-FU) is the foundational anticancer drug used today in the treatment of colorectal cancer (CRC). Dihydropyrimidine dehydrogenase (DPYD) acts as a rate-limiting enzyme in the catabolism of 5-FU. Many reports documented that DPYD IVS14+1 G>A polymorphism has been associated with severe 5-FU toxicity. In present study, we aimed to examine the frequency of DPYD IVS14+1 G>A polymorphism in CRC patients in Western region of India. This polymorphism was examined by PCR-RFLP in 143 CRC patients as well as 25 healthy individuals. All CRC patients and healthy individuals showed 100% frequency of wild type G/G genotypes for DPYD IVS14+1 G>A polymorphism. Thus, the heterozygous variant G/A or homozygous variant A/A genotypes were not prevalent in this population. In nut shell, the study revealed the non-occurrence of variant G/A and A/A genotypes for DPYD IVS 14+1 G>A polymorphism in CRC patients as well as healthy individuals in Western region of India.
Introduction
Colorectal cancer (CRC) is the third most frequent cancer and the fourth leading cause of cancer-related deaths worldwide. 5-fluorouracil (5-FU), the first line chemotherapeutic drug, remains the corner stone of treatment used for single or combination therapy in both adjuvant and advanced settings in CRC. 5-FU is metabolized via two routes. The anabolic route gives rise to active metabolites which disrupt RNA synthesis and the action of thymidylate synthase (TS). The catabolic route inactivates 5-FU through the action of dihydropyrimidine dehydrogenase (DPYD) enzyme, leading to the elimination of the drug from the body [1]. Despite its clinical benefit, 5-FU and its pro- drugs (capecitabine and tegafur-uracile) are associated with frequent gastrointestinal and hematologic toxicities, which often lead to treatment discontinuation [2]. In the past ten years it became clear that the DPYD is an enzyme that regulates 5-FU quantities available for anabolic processes and hence affects its pharmacokinetics, toxicity and efficacy [3]. The human DPYD gene, located on chromosome 1p22 [4], consists of 23 exons and includes 3 kb in length of coding sequences. DPYD, the first key enzyme involved in the catabolism of the uracil and thymine into β-alanine [5], acts as a regulatory enzyme in the catabolism of 5-FU. More than 80% of administered 5-FU gets degraded by DPYD in the liver. DPYD catalyses the conversion of 5-FU to 5-fluorodihydrouracil (5-FDHU), which is further catabolized to 5-fluoro-β-alanine, and is excreted in the urine [6]. So far, more than 30 single nucleotide polymorphisms (SNPs) and deletion mutations have been identified within DPYD gene, although the majority of these variants have no functional consequences on enzymatic activity [2]. However, the most common DPYD IVS14+1 G>A polymorphism, known as DPYD*2A (SNP ID: rs3918290 [7]), results due to G to A transition within the 5’ splice site of intron 14, resuling in exon 14 skipping and an inactive DPYD allele [6]. This SNP leads to deletion of 165 bp in the RNA and subsequent elimination of the fluorouracil binding site in the protein, thereby giving rise to low DPYD activity and severe 5-FU toxicity [8], and thus found to play a role as a determinant of 5-FU toxicity. Wei et al. demonstrated that patients having deletion of 165-bp for this polymorphism, spanning a complete exon of the DPYD gene, have low DPYD activity and greater toxicity to administered 5-FU [9]. Many studies in CRC confirmed the association of this polymorphism with 5-FU toxicity [1, 10, 11]. Several reports have shown that the frequency of DPYD IVS14+1 G>A polymorphism is either low or absent in different racial populations in Europe. Moreover, the absence of this polymorphism in Asian and African population has also been observed [12]. Further, some studies demonstrated that this polymorphism does not exist in CRC patients [13, 14]. Present study aimed to examine the frequency of DPYD IVS14+1 G>A polymorphism in colorectal cancer patients and healthy individuals of Western region of India.
Materials and Methods
Patients
A total of 143 CRC patients underwent surgical resection at the Gujarat Cancer and Research Institute,
- Ahmedabad, India between 2007 and 2014 were included in this study. The key inclusion criterion was the untreated CRC patients with histopathological confirmed adenocarcinoma without any prior history of anticancer treatment. The detailed clinical history (age, gender, anatomic site, TNM stage, histopathological findings) was noted from the case files maintained at the Medical
- Record Department of the institute. Pathologic staging was performed according to TNM classification with
- World Health Organization (WHO) Grading System. The patient and tumor characteristics are shown in Table 1.
- Additionally, 25 healthy individuals with no previous history of any disease or treatment were enrolled for the study. The age range was 31 to 70 years. Out of 25, 12 were females and 13 were males.
Table 1: Patient and tumor characteristics
| Characteristics | N (%) | |||
|---|---|---|---|---|
| Age (Range: 20-86 years) Median: 52 years | ||||
| <52 | 68 (48) | |||
| >52 | 75 (52) | |||
| Gender | ||||
| Female | 58 (41) | |||
| Male | 85 (59) | |||
| Anatomic site | ||||
| Colon | 69 (48) | |||
| Rectum | 74 (52) | |||
| TNM stage | ||||
| I | 24 (16) | |||
| II | 64 (45) | |||
| III | 51 (36) | |||
| IV | 04 (03) | |||
| Lymph node status | ||||
| Absent | 90 (63) | |||
| Present | 53 (37) | |||
| Histological type | ||||
| Adenocarcinoma | 103 (72) | |||
| Mucinous/Signet ring cell adenocarcinoma | 40 (28) | |||
| Tumor differentiation | ||||
| Well | 29 (20) | |||
| Moderate | 94 (66) | |||
| Poor | 20 (14) |
The study has been approved by Institutional Scientific and Ethical Committees and informed consent was obtained from all patients prior to sample collection. To examine DPYD IVS14+1 G>A polymorphism, primary tumor tissue samples of 143 CRC patients were collected on ice directly from the operation theatre. Tumor tissues were selected by a pathologist and divided into two portions. One portion was submitted for the routine histopathological evaluation and the other portion was immediately snap frozen in liquid nitrogen and subsequently preserved at -80°C till the extraction of DNA and subsequently for polymorphism study. Further, in order to verify the genotype difference between tumor and circulating blood samples, out of 143 CRC patients, pre-therapeutic blood samples of 25 patients were subjected to DPYD IVS14+1 G>A polymorphism analysis. In addition, peripheral blood of 25 healthy individuals was analysed in order to identify the correlation of genotype distribution between CRC patients and healthy individuals.
DNA Extraction and DPYD IVS14+1 G>A Polymorphism Study by PCR-RFLP
DNA was extracted from the frozen tumor tissues (N=143) and pre-therapeutic blood samples (N=25) of CRC patients; and from the peripheral blood of healthy individuals (N=25) by phenol-chloroform extraction method. The quantification of extracted DNA samples were performed by agarose gel electrophoresis using Lambda Hind III digest. Also, the purity of the DNA samples was checked spectrophotometrically at 260 and 280 nm. To study DPYD IVS14+1 G>A polymorphism, PCR was performed using QIAGEN Taq PCR kit and following primers sequences: Forward primer: 5’ ATC AGG ACA TTG TGA CAT ATG TTT C 3’; Reverse primer: 5’ CTT GTT TTA GAT GTT AAA TCA CAC ATA 3’ (Sigma-Aldrich). PCR was performed in a ProFlex PCR system (Applied Biosystems, Life Technologies Corporation, USA) using the following conditions: Initial denaturation at 94°C for 3 minutes followed by 35 cycles of denaturation at 95°C for 1 minute, annealing at 57.5°C for 35 seconds and extension at 72°C for 1 minute; and final extension at 72°C for 3 minutes. PCR products were then digested with Nde I restriction enzyme (Takara Bio Inc., Japan) at 37°C overnight and separated on 2.5% ethidium bromide- stained agarose gel. Then, the genotypes of the DNA samples were examined for DPYD IVS14+1 G>A polymorphism by visualizing the gel on UV transilluminator and image was captured on Gel documentation system (Alpha Innotech, USA).
Results
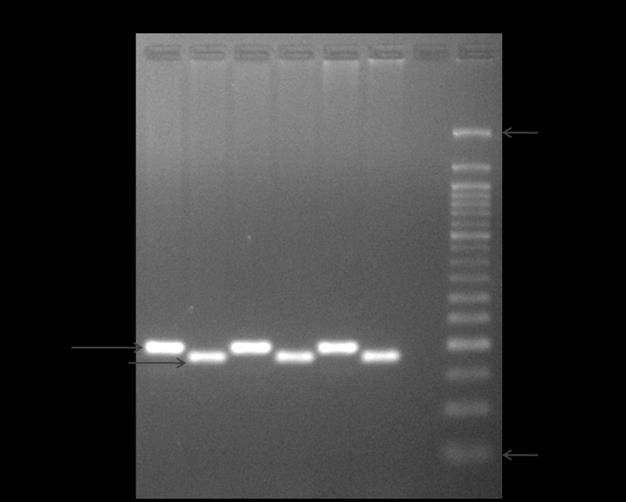
Typically, three types of genotypes have been identified for DPYD IVS14+1 G>A polymorphism after restriction digestion: G/G homozygous wild type at 181 and 17 bp;
G/A heterozygous variant at 181, 154, 27 and 17 bp; and A/A homozygous variant at 154, 27 and 17 bp. However, in present study, when DPYD IVS14+1G>A polymorphism was examined in primary tumor tissues of CRC patients, G/G homozygous wild type genotype was observed in all 100% (143/143) of patients, while the frequencies of both G/A heterozygous variant and A/A homozygous variant genotypes were 0%. Representative gel image of DPYD IVS14+1 G>A polymorphism in CRC patients is shown in Figure 1. Further, when 25 pre-therapeutic blood samples of CRC patients were subjected to DPYD IVS14+1 G>A polymorphism analysis, the distribution of genotypes was observed to be similar between tumor and pre-therapeutic blood samples. Additionally, this polymorphism was evaluated in peripheral blood of healthy individuals (N=25) and the frequency of wild type G/G genotypes was 100% in all healthy individuals. Thus, present study could not identify any of the heterozygous variant G/A genotype or homozygous variant A/A genotype for DPYD IVS14+1 G>A polymorphism in both CRC patients and healthy individuals.
Discussion
DPYD is a powerful liver enzyme to catabolize >80 % of the administered 5-FU in liver. About 8% of the population has what is termed DPYD deficiency, since they have a genetic inability to metabolize 5-FU. The SNPs of DPYD is one of the major reasons for DPYD deficiency [13]. One such exon 14-skipping mutation of DPYD (IVS14+1 G>A polymorphism) provokes a changed splice site leading to an aberrant protein sequence and a loss of the catalytic activity of DPYD. This gene variant accounted for 28% of all patients suffering from severe 5-FU toxicity [15]. This is the first study to investigate the prevalence of DPYD IVS14+1 G>A polymorphism in CRC patients in West India. Current study showed that all the CRC patients as well as healthy individuals showed only G/G wild type genotypes. Accordingly, Li et al. in Chinese population showed 100% of G/G genotypes for DPYD IVS14+1 G>A polymorphism in CRC patients [14]. Zhang et al. also evaluated this SNP by TaqMan real time PCR in 60 CRC patients and observed that all patients were negative for detection of polymorphic variants [13]. Further, Uzunkoy et al. reported that the frequency of wild type G/G was 100% in CRC patients and 98.8% in healthy individuals in Turkish population and no individuals showed homozygous variant A/A genotype among CRC patients or healthy individuals [12]. In addition, the frequency of G/A heterozygous genotype was 2%, while homozygous variant A/A was not detected in CRC patients [1]. Similarly, Botticelli et al. observed only 0.8% G/A genotypes and 99.2% wild type G/G genotypes in mCRC patients [16]. The population based studies in Asia reported that the variant A allele of DPYD IVS14+1 polymorphism was not detected in Koreans [17] and Taiwanese [18]. The frequency of variant A allele has been found to be rare ranging between 0.75% to 0.98% in Turkish, French, Dutch, and German and not detected in African population [12]. All these studies are in accordance with the present results. Furthermore, studies have shown that variant A allele of the DPYD IVS14+1 G>A polymorphism linked with severe 5-FU toxicity. Sulzyc-Bielicka et al. showed that out of 252 studied CRC patients, only one showed heterozygote G/A genotype for IVS14+1 DPYD mutation and it was related to grades 3–4 myelotoxicity upon 5-FU chemotherapy, while the rest 251 patients were homozygous for wild type G/G allele [11]. Several reports also showed the association between DPYD IVS14+1G>A polymorphism and 5-FU toxicity in CRC [1, 10]. Contrary, one study reported that DPYD polymorphism was not associated with increased risk for toxic response to 5-FU in CRC [17]. In a small number (N=25) of Bosnian patients treated with 5-FU, 2% frequency was identified for DPYD IVS14+1 G>A mutation with the presence of only one heterozygote which was also associated with severe 5-FU toxicity [3]. Further, in 100 patients with colon cancer, DPYD IVS14+1 mutation was detected in 14% of patients and the incidence of adverse effects in mutation type was significantly higher than that in wild type [19]. In South Indian population, heterozygous variant G/A genotype was observed in 5.3% and homozygous variant A/A genotype was observed in 1.7% in breast cancer patients treated with 5-FU and most of these patients were found to be poor responders [20]. These studies suggest the role of DPYD IVS 14+1 G>A polymorphism in the screening of patients before administration of 5-FU. However, the present study could not correlate DPYD IVS14+1 polymorphism with 5-FU toxicity due to absence of the variant form in studied population. Additionally, literature survey till date has shown that DPYD IVS14+1 G>A polymorphism in CRC patients has not been extensively studied in Western Indian population. Hence, in order to confirm whether genetic screening for the presence of this polymorphism would be helpful before the administration of 5-FU, it necessitates to explore in a larger number of CRC patients.
Conclusion
This is the first study conducted in Western India which focused mainly on the frequency of DPYD IVS14+1 G>A polymorphism and found the non-occurrence of variant G/A and A/A genotypes in CRC patients as well as healthy individuals.
Acknowledgement
This study was financially supported by The Gujarat Cancer & Research Institute/ Gujarat Cancer Society.
References
-
Rayan Ahmed YMA, Hind MA (2015) Association of dihydropyrimidine dehydrogenase gene polymorphism with toxicity of 5-flurouracil in colorectal cancer in khartoum state. World Journal of Pharmaceutical Research 4(12): 22-34.
-
Catapano O, Barletta O, Di Paolo M, Faioli D, Di Francia R (2014) Impact of DPYD variants in Fluoropyrimidine based-therapy: the state of the art. WCRJ 1(3): e279.
-
Cerić T, Obralić N, Kapur-Pojskić L, Macić D, Beslija S, et al. (2010) Investigation of IVS14+ 1G> A polymorphism of DPYD gene in a group of Bosnian patients treated with 5-Fluorouracil and capecitabine. Bosnian Journal of Basic Medical Sciences 10(2): 133- 139. [INLINE_TABLE:3:0] mutations and polymorphism in various cancers. World Journal of Pharmacy and Pharmaceutical Sciences 2(5): 3779-3789.
-
Bandres E, Zarate R, Ramirez N, Abajo A, Bitarte N, et al. (2007) Pharmacogenomics in colorectal cancer: the first step for individualized-therapy. World J Gastroenterol 13(44): 5888-5901.
-
Panczyk M (2014) Pharmacogenetics research on chemotherapy resistance in colorectal cancer over the last 20 years. World J Gastroenterol 20(29): 9775- 9827.
-
Jennings BA, Loke YK, Skinner J, Keane M, Chu GS, et al. (2013) Evaluating predictive pharmacogenetic signatures of adverse events in colorectal cancer patients treated with fluoropyrimidines. PloS One 8(10): e78053.
-
Ashavaid TF, Raghavan R, Shah S, Kapadia A, Almel S, et al. (2009) TPMT and DPD polymorphisms: Efficient screening method for Indian patients considering taking Thiopurine and 5-FU drugs. Dis Markers 27(5): 231-238.
-
Wei X, McLeod HL, Mc Murrough J, Gonzalez FJ, Fernandez-Salguero P (1996) Molecular basis of the human dihydropyrimidine dehydrogenase deficiency and 5-fluorouracil toxicity. J Clin Invest 98(3): 610- 615.
-
Salgueiro N, Veiga I, Fragoso M, Sousa O, Costa N, et al. (2004) Mutations in exon 14 of dihydropyrimidine dehydrogenase and 5-Fluorouracil toxicity in Portuguese colorectal cancer patients. Genet Med 6(2): 102-107.
-
Sulzyc-Bielicka V, Binczak-Kuleta A, Pioch W, Kladny J, Gziut K, et al. (2008) 5-Fluorouracil toxicity- attributable IVS14+1G>A mutation of the dihydropyrimidine dehydrogenase gene in Polish colorectal cancer patients. Pharmacol Rep 60(2): 238- 242.
-
Uzunkoy A, Dilmec F, Ozgonul A, van Kuilenburg AB, Akkafa F (2007) Investigation of IVS14+ 1G> A polymorphism of DPYD gene in a group of Turkish patients with colorectal cancer. Anticancer Res 27(6B): 3899-3902.
-
Zhang X, Sun B, Lu Z (2013) Evaluation of clinical value of single nucleotide polymorphisms of dihydropyrimidine dehydrogenase gene to predict 5- fluorouracil toxicity in 60 colorectal cancer patients in China. Int J Med Sci 10(7): 894-902.
-
Li GY, Duan JF, Li WJ, Liu T (2016) DPYD*2A/*5A/*9A and UGT1A1*6/*28 polymorphisms in Chinese colorectal cancer patients. J Can Res Ther 12(2): 782- 786.
-
Van Kuilenburg AB, Meinsma R, Zoetekouw L, Van Gennip AH (2002) High prevalence of the IVS14+ 1G> A mutation in the dihydropyrimidine dehydrogenase gene of patients with severe 5-fluorouracil-associated toxicity. Pharmacogenetics 12(7): 555-558.
-
Botticelli A, Borro M, Onesti CE, Strigari L, Gentile G, et al. (2016) Degradation Rate of 5-Fluorouracil in Metastatic Colorectal Cancer: A New Predictive Outcome Biomarker? PloS one. 11(9): e0163105.
-
Cho HJ, Park YS, Kang WK, Kim JW, Lee SY (2007) Thymidylate synthase (TYMS) and dihydropyrimidine dehydrogenase (DPYD) polymorphisms in the Korean population for prediction of 5-fluorouracil-associated toxicity. Ther Drug Monit 29(2): 190-196.
-
Hsiao HH, Yang MY, Chang JG, Liu YC, Liu TC, et al. (2004) Dihydropyrimidine dehydrogenase pharmacogenetics in the Taiwanese population. Cancer Chemother Pharmacol 53(5): 445-451.
-
Sun W, Yan C, Jia S, Hu J (2014) Correlation analysis of peripheral DPYD gene polymorphism with 5- fluorouracil susceptibility and side effects in colon cancer patients. Int J Clin Exp Med 7(12): 5857-5861.
-
Kumar CK, Murthy S, Jamil K (2007) Possible associations of splice site mutation of dihydropyrimidine dehydrogenase (IVS14+ 1G> A) in adverse drug reactions in some invasive ductal carcinoma patients. Int J Pharmacol 3(2): 130-136.
- Cancer Diagnosis from RNA Sequence of Blood Cells by Using AI
- Field Cancerization in Oral Cavity, Case Report and Review of Literature. Oncologic Program Salud Integral Hospital, Managua, Nicaragua
- Identification of B Lymphocytes in Cancer Patient’s Blood
- A Case Report of a Breast Cancer Patient Developing Pneumonitis as a Result of Abemaciclib Therapy
- Immune Checkpoint Therapeutics for Today’s Fight and Beyond
- The Amalgamated Sophomore-Gonadoblastoma