Correlation of P53 Expression with Different Histological Grades in Oral Squamous Cell Carcinoma Patients from Northern India
In the present study, out of the total 100 patients studied, 75 patients (75%) were males and majority of patients were in 50-75 age groups and complained of dysphagia. It was found that the most common site of incidence of oral cancer in tobacco and betel quid chewers was buccal mucosa. The aim of this study is to further examine the relationship between p53 expressions with different histological grades in oral squamous cell carcinoma (OSSC) patients from north India. It was found that there was no p53 expression in normal tissues while in oral SCC patients with tobacco and betel quid chewing habit, the percentage of positive cases as well as p53 positivity showed an increase with increasing grade of SCC. The expression of p53 was significantly associated with histological grade in oral cancer in tobacco and betel quid chewers. In case of p53 expression, statistically significant difference in p53 positivity was observed only on comparing well differentiated SCC with poorly differentiated SCC. The expression of p53 was not similar in different sites of oral cavity but was more frequently seen in gingivia, floor of mouth, tongue, and buccal mucosa.
Introduction
Oral cancer is sixth most common cancer worldwide and third most common cancer in developing countries accounting for about up to 40% of all cancers [1].
Incidence of oral cancer is increasing day by day due to more intakes of various forms of tobacco and alcohol drinking, which are considered to be the two most important etiological factors in the development of oral cancer [2]. It is estimated that 75-90% of all head and neck cancers are caused due to the tobacco use and tobacco users are between 20-40 times more likely to develop head and neck cancer than non consumers, depending upon the amount of use as well as the age, sex and race of the user [3]. Tobacco may be taken in various ways like smoking, chewing, etc. The most common form of tobacco chewing in India is betel quid. The 'quid' for chewing consists of areca nut and pieces of unripe betel fruit or areca nut wrapped in a piece of betel leaf together with white or red lime. Betel quid chewing has a strong association with oral cancer which arises predominantly from surface epithelium with evolution from early premalignant lesions. Oral Squamous Cell Carcinoma arise as a consequence of multiple molecular events induced by the effects of various carcinogens from habits such as areca nut and betel quid chewing, influenced by environmental factors, possibly viruses in some instances, against a background of inheritable resistance or susceptibility [4]. An individual difference in the susceptibility to chemical carcinogens is one of the most important factors in the estimate of risk of human cancer as some patients appear susceptible because of inherited trait(s) in their ability or inability to metabolize carcinogens or pro-carcinogens, possibly along with an impaired ability to repair DNA damage [5]. Oral carcinogenesis is a multi-step process in which 6- 10 genetic events lead to the disruption of the normal regulatory pathways that control basic cellular functions. In recent years, several alterations in the expression of tumor suppressor genes and oncogene in the development of Oral Squamous Cell Carcinoma (OSCC) have been described [6, 7, 8]. Keeping in view above facts, the present study was done to investigate the expression of p53 (product of tumor suppressor gene) and to further examine the relationship between p53 expression with different histological grades in oral squamous cell carcinoma (OSSC) patients from north Indian patients with tobacco and betel quid chewing habit.
Material and Methods
Tissue Specimens
Biopsy tissue specimens from 60 untreated primary Oral Squamous cell Carcinoma (45 men and 15 women) were obtained from Department of Otorhinolaryngology (ENT), Jawaharlal Nehru Medical College, Aligarh Muslim University, Aligarh India (Northern India) from Nov, 2004 up to May, 2007. The patients were grouped into 4 age groups: 0-25, 25-50, 50-5 and above 5 years. The tumors were classified into grades I, II, III according to their cellular differentiation which is equivalent to well, moderately and poorly differentiated tumors. Clinic pathological information including age, gender, areca nut and betel quid intake history, location and histological grade was obtained in each case. Immunohistochemical staining
Preparation of Sections
Formalin fixed, paraffin embedded sections were mounted on slides coated with poly-L-lysine solution. The sections mounted on coated slides were incubated at 56 oC overnight for better adhesion. Sections were deparaffinised in xylol and hydrated through graded alcohols to Tris buffer saline (0.005 M TRIS buffer, pH7.6). Antigen retrieval was done using citrate buffer (0.01mol/L, pH 6.0) in a pressure cooker by heating up to one whistle and then allowing cooling to room temperature before opening the lid of cooker. Endogenous peroxidise activity was blocked by treating sections with 3% hydrogen peroxide in methanol (LSAB Kit) for 10-15 min [9, 10].
Immunostaining
Primary antibody (FL-393 antibody, Santa Cruz Biotechnology, USA for p53) was added to the sections at room temperature and incubated overnight at 38 oC in a moist chamber. The sections were then washed with three changes of TBS for 10 min. each and were incubated in biotinylated secondary (Link) antibody at room temperature for 30 minutes in a moist chamber and washed in TBS(x3) for 10 min. duration each. Sections were incubated in streptavidin at room temperature for 45 min. in moist chamber and washed in TBS and were incubated in freshly prepared 3, 3’ diaminobenzidine tetra hydrochloride (DAB) solution. This was prepared by diluting DAB chromogen (1 drop) in 1 ml of DAB substrate. DAB was then used as the substrate for localizing antibody binding Sections were washed in distilled water, counterstained in hemotoxylin (1-2 dips), dehydrated through graded alcohols, cleaned in xylol and mounted in DPX. The positive control slides were incubated with primary antibody whereas in negative controls, primary antibodies were replaced with normal mouse serum. For protein expression, only nuclear positivity (strong brown staining) was assessed quantitatively. Only the percentage was quantified and the percentage of positively stained cells in the whole layer of epithelium was determined by scanning the entire section and was recorded by assigning cases to one o the our following categories: (a) 0 = No epithelial cells stained, (b) + = up to 25% of cells positive, (c) ++ = 26 to 50% of cells positive, (d) +++ = > 50% of cells positive. This quantification of protein positivity was done according to the method recommended by already known workers [9, 10].
In the present series, patients belonged to age group of 25-100 years, out of which maximum incidence of cases (n=62) was seen in 50-75 years of age group (62% of cases). Only 20% (n=20) and 18% (n=18) cases were in the age group of 25-50 years and 75-100 years respectively (Table 1). In controls, 50-75 age group predominated with 60% (n=90) of the controls belonging to this age group. Only 6.66% (n=10), 18% (n=27) and 15.33 % (n=23) were in the 0-25, 25-50 and 75-100 age group, respectively.
Statistical Analysis
An SPSS for windows computer programme (SPSS Inc. Chicago 11, USA, version 13) was used for statistical analysis. The association between protein expression and tumor location was analyzed by the Chi-square test. The relationship between protein expression and histolopathological grade was analyzed by Kruskal-Wallis analysis of variance (ANOVA). Wilcoxon paired sample test was used to analyze the differences within the three categories of histopathological grade and protein expression. A p value of less than 0.05 was accepted as statistically significant.
Results
Age Incidence
| CATEGORY | CASES | CONTROLS | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Age Group (years) | Male | Female | Total | Male | Female | Total | ||||||
| 0-25 | 0 | 0 | 0 | 7 | 3 | 10 | ||||||
| 25-50 | 13 | 7 | 20 | 21 | 6 | 27 | ||||||
| 50-75 | 48 | 14 | 62 | 68 | 22 | 90 | ||||||
| 75-100 | 14 | 4 | 18 | 19 | 4 | 23 | ||||||
| Total | 75 | 25 | 100 | 125 | 35 | 150 |
Table 1: Occurrence of oral cancer in different age group of patients.
Sex Incidence
Out of the total 100 cases studied, 75 cases (75%) were males and rest (25%) were female, male-female ratio being 3:1 (Table 2). Out of 150 controls, 115 (76.66%) were males and rest 35 (23.33%) were females, male- female ratio being 3.28:1 (Table 2).
| Category | Cases | Controls | ||
|---|---|---|---|---|
| Sex | Number | Percentage | Number | Percentage |
| Male | 75 | 75% | 115 | 76.60% |
| Female | 25 | 25% | 35 | 23.33% |
| Total | 100 | 100% | 150 | 100% |
Table 3: Number and percentage of patients in different sex groups. Mean age of male and female cases were 58 years and 53 years,
Most of cases (68.97%) presented with some complaint within first 6 months of the start of the lesion. Only 23.72% presented after 6 months to 1 year while 5.83% and 1.45% presented symptoms after 12 months and 18 months respectively (Table 4).
| Category | Cases | Controls | ||
|---|---|---|---|---|
| Sex | Number | Mean age | Number | Mean age |
| Male | 75 | 58 | 115 | 56 |
| Female | 25 | 53 | 35 | 54 |
| Total | 100 | 56.75 | 150 | 55.53 |
Table 2: Mean age of patient in different sex groups.
Duration of Symptoms
| Presenting Complaint | <6 Months | 6-12 Months | 12-18 Months | 18-24 Months | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Difficulty in swallowing | 55 | 14 | 10 | 1 | ||||||||||
| 2. Burning in mouth & throat | 35 | 8 | - | 2 | ||||||||||
| 3. Pain during swallowing | 15 | 14 | - | - | ||||||||||
| 4. Swelling in neck | 13 | 7 | - | - | ||||||||||
| 5. Change in voice | 6 | 3 | 1 | - | ||||||||||
| 6. Pain in the lesion | 36 | 11 | 2 | 1 | ||||||||||
| 7. Pain in the ear | 6 | 4 | 2 | - | ||||||||||
| 8. Difficulty in opening the mouth | 7 | - | - | - | ||||||||||
| 9. Difficulty in speech | 3 | 1 | - | - | ||||||||||
| Bleeding from the mouth | 6 | 1 | - | - | ||||||||||
| Increased salivation | 7 | 2 | 1 | - | ||||||||||
| Total | 189 | 65 | 16 | 4 | ||||||||||
| Percentage | 68.97% | 23.72% | 5.83% | 1.45% |
Table 4: Duration of initial presentation of clinical symptoms by patients.
| Presenting Complaint | No. of cases | |
|---|---|---|
| 1 | Difficulty in swallowing | 80 |
| 2 | Pain in the lesion | 50 |
| 3 | Burning in mouth & throat | 45 |
| 4 | Pain during swallowing | 29 |
| 5 | Swelling in neck | 20 |
| 6 | Pain in the ear | 12 |
| 7 | Change in voice | 10 |
| 8 | Increased salivation | 10 |
| 9 | Difficulty in opening the mouth | 7 |
| 10 | Bleeding from the mouth | 7 |
| 11 | Difficulty in speech | 4 |
Table 6: Number of cases showing occurrence of different symptoms. Relation of tobacco and betel quid chewing with oral cancer Ou
| Risk factor | Oral Cancer | Oral Cancer | Total | ||||
|---|---|---|---|---|---|---|---|
| present | absent | ||||||
| (cases) | (Controls) | ||||||
| Tobacco & betel quid | 100 | 38 | 138 | ||||
| (Exposed) | (a) | (b) | (a+b) | ||||
| Non-users | 0 | 112 | 112 | ||||
| (Not exposed) | (c) | (d) | (c+d) | ||||
| Total | 100 | 150 | 250 | ||||
| (a+c) | (b+d) |
Table 5: Chi square values of tobacco and betel quid in oral cancer in patients and control. Exposure Rates Cases= a/ (a+c) = 100
Table 6: Chi square values of tobacco and betel quid in oral cancer in patients and control. Exposure Rates Cases= a/ (a+c) = 100/100 = 100% Controls= b/ (b+d) = 38/150 = 25.3% This shows that the consumption of tobacco and betel quid is highly related with the development of oral cancer as exposure rate among cases is very high i.e. 100% in comparison to the low exposure rate of 25.3% among controls. However this cause-effect relationship is examined more scientifically on the basis of various other statistical tests like Chi-square test (χ2test). Chi square test offers an opportunity of testing the significance of difference between two proportions. This test is based on the “Null Hypothesis” viz. there is no difference between tobacco and betel quid users and non- users in the development of oral cancer. We shall now rewrite the previous table showing the observed (O) and expected (E) values in each cell (Table 7).
| Risk factor | Oral Cancer | Oral Cancer | Total | ||||
|---|---|---|---|---|---|---|---|
| Present | Absent | ||||||
| Tobacco and betel quid chewers | O=100 | O=38 | 138 | ||||
| E= 69 | E=69 | ||||||
| Non-users | O=0 | O=112 | 112 | ||||
| E=56 | E=56 | ||||||
| Total | 125 | 125 | 250 |
Table 7: Exposure of tobacco and betel quid in oral cancer patients and controls and calculation of χ2 value. The calculated valu
χ2 = Σ (o-E)2/E=135.226 Table 7: Exposure of tobacco and betel quid in oral cancer patients and controls and calculation of χ2 value. The calculated value of χ2 is 135.226 while the value of p (Probability) at 95% level of significance for 1 degree of freedom (df.) is .000. It means that p<0.001 so it is “Statistically significant”. It indicates that our "Null hypothesis" was wrong and there is definite cause-effect relationship or we can say that there is strong association between consumption of tobacco and betel quid with development of oral cancer.
Socio Economic Status and Oral Hygiene
The role of these factors in the predisposition of patients to the development of oral cancer was not studied. However it was noted that most of the sufferers belonged to the lower socio-economic status and oral hygiene was poor in most of the patients.
Site of Lesion
Oral cancer most commonly occurred in buccal mucosa in cases. The incidence of oral cancer in different sites of oral cavity is given below (Table 8).
| S. No. | Site of Lesion | No. of Cases | Percentage | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. | Tongue | 22 | 22% | ||||||||
| 2 | Buccal mucosa | 45 | 45% | ||||||||
| 3 | Lip | 6 | 6% | ||||||||
| 4 | Hard palate | 5 | 5% | ||||||||
| 5 | Floor of mouth | 17 | 17% | ||||||||
| 6 | Gingivia | 3 | 3% | ||||||||
| 7 | Retromolar region | 2 | 2% |
Table 8: The incidence of oral cancer in different sites of oral cavity. Oral cancer most commonly involved buccal mucosa and occ
Histological Type of Lesion
All the biopsy samples of the patients were found to be having squamous cell carcinoma on histopathological examination (Table 9).
| Histological type | No. of cases | Percentage | ||||||
|---|---|---|---|---|---|---|---|---|
| Squamous cell carcinoma | 60 | 100 | ||||||
| Adenocarcinoma | 0 | 0 | ||||||
| Lymphoepithelioma | 0 | 0 |
Table 9: Distribution of oral cancer lesion in different histological types.
Immunohistochemical Studies (P53 Protein Expression)
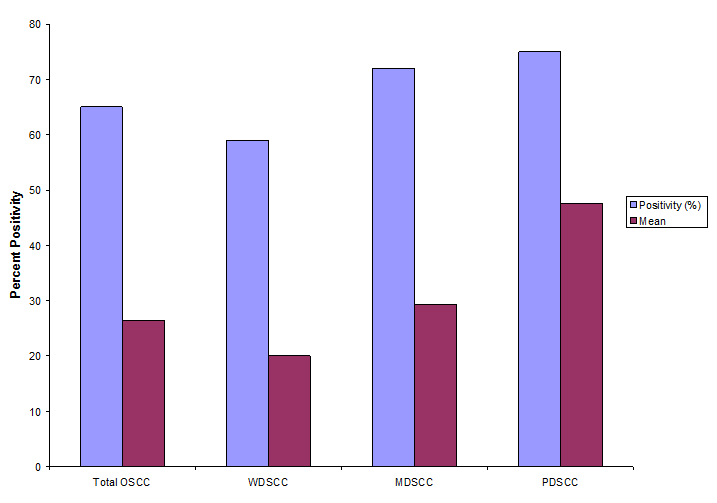
Tissues of oral SCC patients with tobacco and betel quid chewing habit (60 specimens) and 10 normal oral tissues were subjected to Immunohistochemical staining for expression of p53 using FL-393 antibody. Only strong brown nuclear staining of epithelial cells was considered positive. Those histological sections with uniform and good intensity were assessed for p53 scoring. The scores obtained were expressed as: Positive cases (%) gives the percentage of cases showing positive staining with IHC. p53 positivity (%) gives the percentage of cells showing a positive staining reaction with p53 IHC. The p53 was expressed in 65% (n=39) of the cases but was not expressed in controls. The (Figure 1A-D) shows the expression of p53 in tobacco and betel quid chewers as well as in controls. There were 34(56.6%) cases of well differentiated SCC.
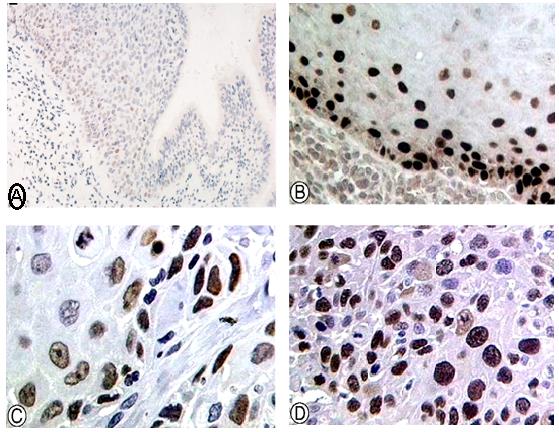
- Figure 1 (A-D): Immunohistochemical detection of p53 using p53 antibody in tissues obtained from oral cancer patients. (A) Representative Figure Showing Expression of p53 in Normal Tissue (magnification x 200) (B)
- Representative Figure Showing Expression of p53 in Well Differentiated Oral SCC (magnification x 400) (C)
- Representative Figure Showing Expression of p53 in Moderately Differentiated Oral SCC (magnification x 400) (D)
- Representative Figure Showing Expression of p53 in Poorly Differentiated Oral SCC (magnification x 400).
- 18(30%) cases of moderately differentiated SCC and
- 8(13.3%) cases of poorly differentiate SCC. (Table 10) depicts the positive cases (%) and mean p53 positivity
- Histological Diagnosis
- +ve cases
- -ve cases
- Total Cases
- Category
- Mean + SD
- Range
- (%)
- (%)
- Oral SCC
- 60
- 39(65%)
- 21(35%)
- 26.46 ± 23.90
- 0-75 a) Well differentiated
- 34
- 20(58.8%)
- 14(41.2%)
- 20.0+19.32
- 0-55 b) Moderately differentiated
- 18
- 13(72.22%)
- 05(27.77%)
- 29.33+23.50
- 0-70 c) Poorly differentiated
- 8
- 06(75%)
- 02(25%)
- 47.5+31.38
- 0-75
- Controls
- 10
- 0
- 10
- 0
- 0
Table 10: p53 Expression in oral SCC’s in tobacco and betel quid chewers.
It was found that expression of p53 was significantly associated with histological grade in oral cancer in tobacco and betel quid chewers (χ2=7.077, df=2, p=0.029). Statistically significant difference in p53 positivity was observed on comparing well differentiated SCC (p53 positivity = 20+19.32) with poorly differentiated SCC (p53 positivity=47.5+31.38, p=0.001) but no statistical significance (p=0.27) was observed in p53 positivity between poorly differentiated SCC (p53 positivity=47.5+31.38) and moderately differentiated SCC (p53 positivity= 29.33+23.50), as well as between well differentiated SCC (p53 positivity= 20+19.32) with moderately differentiated SCC (p53 positivity=29.33+23.50, p value =0.27). Expression of p53 in various sites of oral cavity was investigated and it was found that p53 was more frequently expressed in sites like gingivia (1/1, 100%), floor of mouth (5/7, 71%) buccal mucosa (20/31, 64.5%), tongue (7/10, 70%) and lip (3/5, 60%) while less frequently in sites like hard palate ( % 50 ,4 / 2 ) and retro molar region (1/2, 50%). Further the association between expression of p53 and site of incidence of oral cancer was evaluated. It was found that there is no significant association between p53 expression and primary site of incidence of oral cancer (χ2 =1.427, df=6, p=0.964).
Discussion
Age and Sex Incidence
In this study the highest number was between 50-75
years of age group i.e. 62 individuals (62%) suffering from cancer. Peak age incidence in Wahi’s series was 50- 54 years while in another study by 45% of oral cancer cases were between 5th & 6th decade [11, 12]. There was no significant difference in age incidence between the age groups of patients of our series and that of other workers. The average age in this study was 56.75 years in patients in comparison to 54.8 years in the study of Nandakumar A, et al. [13] and 50.35 years in the study of Rao DN, et al. [14]. Oral cancer is more common in males as compared to females. A study by G. Krihna et al., reported the incidence of males to be 77.6% while the study by R. Mehrotra et al. have reported about 74% of oral cancer in males [15, 16]. In our series, also, males constituted about 75% of the total cases. In Wahi’s series, the male female ratio was 2:1 [11]. In case control study by G. Krishna et al., there were 552 males and 224 females’ i.e. 2.5:1 ratio [15]. In Mehrotra series, the female ratio was 2.3:1 and in our series, it was 3:1. The mean age of male and female cases in our series was 58 and 53 years, respectively while the mean age was found to be 63.5 years for males and 60.6 years for females in study by Langdon JD, et al. [17].
Relation of Tobacco and Betel Quid Chewing With Oral Cancer
In our study we have observed that tobacco and betel quid chewing is significantly associated with development of oral cancer. In India, correlation of tobacco and betel quid chewing and smoking with oral cancer has been demonstrated in earlier studies [12, 18, 19, 20]. The observations made by all of them pointed that the habit of tobacco and betel quid chewing is important risk factor in development of oral cancer. Our findings are in accordance with observation made by earlier studies. Habit of Paan chewing is common in India in both genders. Paan generally includes calcium hydroxide, areca nut (from the areca catechu tree) and betel leaf (from the piper betel vine). Sankaranarayanan R, et al. showed that paan-tobacco chewing is major risk factor for cancers of buccal and labial mucosa [12]. Similarly Nandakumar, et al. confirmed that paan tobacco chewing is a major risk factor in the occurrence of cancers of the oral cavity [13]. In the study by Balaram P, et al. 591 oral cancer cases (309 males and 282 women) with 584 hospital controls were taken. They found that most cases of oral cancer in both genders were attributed to habit of paan tobacco intake [21].
Incidence of Site of Lesion
In our series, maximum 45 cases (45%) were of cheek carcinoma (Buccal mucosa) followed by malignancy of tongue (22%) and the floor of mouth (17%). In Wahi’s series, cases of carcinoma cheek were maximum in the oral cancer patients (53.91%). In a study conducted by Rao et al. the frequency of carcinoma cheek was maximum i.e. 44.4%. In study conducted by Agarwal et al. buccal mucosa was predominant site in betel related oral cancer [14, 21]. Ranasingh, et al. have also shown that buccal mucosa cancer is predominant site of oral cancer in tobacco and betel quid chewers while Chang et al., found 57.8% cases of oral cancer to be cheek carcinomas in betel and tobacco related oral cancer [22, 23]. Our findings about incidence of site of lesion are in accordance with earlier studies. p53 Expression The Immunohistochemical detection of p53 in biopsy specimen as a potential marker is of immense interest to researchers, as it is most commonly identified mutated gene in various human cancers like lung, breast, prostate and oral cancer. The gene coding for p53 protein i.e. TP53 is located on human chromosome 17 P 13:1 and encodes a 53 KDa nuclear phosphor protein that plays an important role in regulation of normal cell proliferation [24, 25]. The wild type p53 protein has a half life time of 6- 20 min [10]. while the mutant form has a half life of several hours and can be detected Immunohistochemical. The p53 mutations are often associated with the development and/or progression of malignant neoplasm [26]. About 90% of mutations at p53 locus were found to be mis-sense mutations, within the region of exon 5 to 8 [27]. Immunohistochemical studies of p53 expression in SCC of oral mucosa have shown over expression of p53 protein. In the present study, Immunohistochemical studies for p53 expression was done on formalin fixed and paraffin embedded tissue sections, using FL-393 antibody (Santa Cruz Biotechnology) on biopsy specimens of 60 oral SCC patients with tobacco and betel quid chewing habit and 10 controls. Only strong brown nuclear staining was considered positive and p53 scoring was done in accordance to literature [9, 10]. The scores were expressed as the percentage of positive cases in each category and the percentage of p53 positivity in each case. In control specimens who were taken from normal individuals, there was no expression of p53 protein. This can be attributed to fact that p53 in its wild form has very short life time (16-20 min) and cannot be detected by immunohistochemistry. In present study, increased percentage of positive cases as well as mean p53 percent positivity was observed with increasing grade of differentiation in oral squamous cell carcinoma (oral SCC) patients with tobacco & betel quid chewing habit. The 39 OSCC cases (65%) showed positive p53 expression and mean positivity was 26.46 + 23.90. Many previous studies have reported similar positivity in oral SCC patients with tobacco and betel quid chewing habit. Agarwal et al. reported that 65.3% of cases of oral SCC with tobacco and betel quid chewing habit showed p53 positivity while Pande et al., reported 65% positivity [28], Jie Xu, et al. reported 59% positivity, respectively in patients with tobacco and betel quid chewing habit. However lower values were observed by Kuttan et al. and Thongsukai et al., who reported 56.5% and 38.5% positivity, respectively but all researchers reported increase in number of positive cells [29, 30, 31]. In our study, we further investigated the expression of p53 in various sites of oral cavity. The p53 expression was more frequently seen in gingivia (100%), floor of mouth (71%), tongue (70%) and buccal mucosa (64.5%). There are only few studies which have correlated the expression of p53 with site of incidence in oral cavity. Kaur et al., found that there was no association between p53 expression and primary site of cancer (p=0.08) [32]. Similarly Claudia et al., found no association between p53 expression and different oral sites (p=0.53) [33]. In our study, expression of p53 was not found to be associated with site of oral cancer (p=0.964) thus supporting the earlier studies that p53 expression is independent of site of incidence of oral cancer. The complete absence of p53 positivity in some squamous cell carcinomas was explained by Nylander et al. as the tumors completely lacking detectable p53 could either comprise of wild tumor protein or have a change in function in TP53 gene resulting in production of a truncated, non-functional and non detectable protein [34]. The relationship between p53 expression and tumor grade was also evaluated in our study. An increased positivity with increasing grade was observed in the present study. The difference was found to be significant between well differentiated (20.0 ± 19.32) and poorly differentiated (47.5 ± 31.38) oral SCC, p=.001. However no statistical significance (p=0.27) was observed in p53 positivity among poorly differentiated SCC (p53 positivity = 47.5 ± 31.38) and moderately differentiated SCC (p53 positivity = 29.33 ± 23.50), as well as between well differentiated SCC (p53 positivity = 20 ± 19.32) and moderately differentiated SCC (p53 positivity = 29.33 ± 23.50), p value =0.27. Although most of the known literature have not any shown positive relationship between p53 expression and histological grading of oral SCC [35, 36, 37]. However, some studies have demonstrated a positive correlation between p53 expression and high grade of malignancy [38]. In our study, significant association was found between p53 positivity and degree of differentiation of tumors (p=0.029). Similar to results in our study, some researchers have found a tendency towards higher incidence of p53 positivity in poorly differentiated oral carcinomas [38, 39].
Acknowledgements
Authors thank Department of Medical Biochemistry, JNMC, Aligarh Muslim University, for the research support and successful completion of work.
References
-
Parkin SM, Laara E, Muir CS (1988) Estimates of the worldwide frequency of sixteen major cancers in 1980. Int J Cancer 41(2): 184-197.
-
Cawson RA, Langdon JD, Eveson JW (1996) Surgical Pathology of the Mouth and Jaws. Oxford: Wright
-
Graham S, Dayal H, Rohrer T, Swanson M, Sultz H, et al. (1977) Dentition, diet, tobacco and alcohol in the epidemiology of oral cancer. J Natl Cancer Inst 59(6): 1611-1618.
-
Vogelstein B, Kinzler KW (1993) The multistep nature of cancer. Trends Genet 9(4): 138-141.
-
Sankaranarayanan R, Duffy SW, Day NE, Nair MK, Padmakumary G (1989) A case-control investigation of cancer of the oral tongue and the floor of the mouth in southern India. Int J Cancer 44(4): 617-621.
-
Balaram P, Sridhar H, Rajkumar T, Vaccarella S, Herrero R, et al. (2002) Oral cancer in southern India: the influence of smoking, drinking, paan-chewing and oral hygiene. Int J Cancer 98(3): 440-445.
-
Williams HK (2000) Molecular pathogenesis of oral squamous carcinoma. Mol Pathol 53(4): 165-172.
-
Lee WH (1993) Tumor suppressor genes-the hope. FASEB J 7(10): 819-823.
-
Hall PA, Lane DP (1994) p53 in tumour pathology: can we trust immunohistochemistry? J Pathol 172(1): 1-4.
-
Chiang CP, Lang MJ, Liu BY, Wang JT, Leu JS, et al. (2000) Expression of p53 protein in oral submucous fibrosis, oral epithelial hyperkeratosis, and oral epithelial dysplasia. J Formos Med Assoc 99(3): 229- 234.
-
Wahi PN, Saxena SN, Pashpati N (1958) Carcinoma of the oral cavity. J Indian Med Assoc 31(8): 309-19.
-
Khuri FR, Lippman SM, Spitz MR, Lotan R, Hong WK (1997) Molecular epidemiology and retinoid chemoprevention of head and neck cancer. J Nat Cancer Inst 89(3): 199-211.
-
Nandakumar A, Thimmasetty KT, Sreeramareddy NM, Venugopal TC, Rajanna, et al. (1990) A population- based case-control investigation on cancers of the oral cavity in Bangalore India. Br J Cancer 62(5): 847- 851.
-
Rao DN, Ganesh B, Rao RS, Desai PB (1994) Risk assessment of tobacco, alcohol and diet in oral cancer--a case-control study. Int J Cancer 58(4): 469- 473.
-
Gopal K, Saxena ON, Singh AK (1967) Oral Carcinoma. Indian J Surgery 29: 229-235.
-
Mehrotra R, Singh M, Kumar D, Pandey AN, Gupta RK, et al. (2003) Age specific incidence rate and pathological spectrum of oral cancer in Allahabad. Indian J Med Sci 57(9): 400-404.
-
Langdon JD, Harvey PW, Rapidis AD, Patel MF, Johnson NW, et al. (1977) Oral cancer: the behaviour and response to treatment of 194 cases. J Maxillofac Surg 5(4): 221-237.
-
Jayant K, Balakrishnan V, Sanghvi LD, Jussawalla DJ (1977) Quantification of the role of smoking and chewing tobacco in oral, pharyngeal and oesophageal cancers. Br J Cancer 35(2): 232-235.
-
Notani PN (1988) Role of alcohol in cancers of the upper alimentary tract: use of models in risk assessment. J Epidemiol Community Health 42(2): 187-92.
-
Nawroz H, van der Riet P, Hruban RH, Koch W, Ruppert JM, et al. (1994) Allelotype of head and neck squamous cell carcinoma. Cancer Res 54(5): 1152- 1155.
-
Sandhya A, Meera M, Anurag S, Ranju R (1999) MDM2/p53 co-expression in oral premalignant and malignant lesions: potential prognostic implications. Oral Oncology 35(2): 209-216.
-
Ranasinghe AW, Warnakulasuriya KA, Johnson NW (1993) Low prevalence of expression of p53 oncoprotein in oral carcinomas from Sri Lanka associated with betel and tobacco chewing. Eur J Cancer B Oral Oncol 29B(2): 147-150.
-
Chang KC, Su IJ, Tsai ST, Shieh DB, Jin YT (2002) Pathological features of betel quid-related oral epithelial lesions in taiwan with special emphasis on the tumor progression and human papillomavirus association. Oncology 63(4): 362-369.
-
Raybaud-Diogène H, Tétu B, Morency R, Fortin A, Monteil RA (1996) p53 overexpression in head and neck squamous cell carcinoma: review of the literature. Eur J Cancer B Oral Oncol 32B (3): 143- 149.
-
Lane DP, Benchimol S (1990) p53: oncogene or anti- oncogene? Genes Dev 4(1): 1-8.
-
Allred DC, Clark GM, Elledge R, Fuqua SA, Brown RW, et al. (1993) Association of p53 protein expression with tumor cell proliferation rate and clinical outcome in node-negative breast cancer. J Nat Cancer Inst 85(3): 200-206.
-
Lane DP (1998) Killing tumor cells with viruses-a question of specificity. Nat Med 4(9): 1012-1013.
-
Pande P, Soni S, Kaur J, Agarwal S, Mathur M, et al. (2002) Prognostic factors in betel and tobacco related oral cancer. Oral Oncol 38(5): 491-499.
-
Kuttan NA, Rosin MP, Ambika K, Priddy RW, Bhakthan NM, et al. (1995) High prevalence of expression of p53 oncoprotein in oral carcinomas from India associated with betel and tobacco chewing. Eur J Cancer B Oral Oncol 31B(3): 169-173.
-
Xu J, Gimenez-Conti IB, Cunningham JE, Collet AM, Luna MA, et al. (1998) Alterations of p53, cyclin D1, Rb, and H-ras in human oral carcinomas related to tobacco use. Cancer 83(2): 204-212.
-
Thongsuksai P, Boonyaphiphat P (2001) Lack of association between p53 expression and betel nut chewing in oral cancers from Thailand. Oral Oncol 37(3): 276-281.
-
Kaur J, Srivastava A, Ralhan R (1998) Prognostic significance of p53 protein overexpression in betel- and tobacco-related oral oncogenesis. Int J Cancer 79(4): 370-375.
-
Cláudia T, Linaena MSF, Sérgio VC, Maria CFA, Maria AV, et al. (2006) p53 Immunoexpression in Oral Squamous Cell Carcinomas from Different Anatomical Sites: A Comparative Study. Int J Morphol 24(2): 231- 238.
-
Nylander K, Dabelsteen E, Hall PA (2000) The p53 molecule and its prognostic role in squamous cell carcinomas of the head and neck. J Oral Pathol Med 29(9): 413-425.
-
Chiang CP, Huang JS, Wang JT, Liu BY, Kuo YS, et al. (1999) Expression of p53 protein correlates with decreased survival in patients with areca quid chewing and smoking-associated oral squamous cell carcinomas in Taiwan. J Oral Pathol Med 28(2): 72- 76.
-
Saranath D, Tandle AT, Teni TR, Dedhia PM, Borges AM, et al. (1999) p53 inactivation in chewing tobacco- induced oral cancers and leukoplakias from India. Oral Oncol 35(3): 242-250.
-
Kerdpon D, Sriplung H, Kietthubthew S (2001) Expression of p53 in oral squamous cell carcinoma and its association with risk habits in southern Thailand. Oral Oncol 37(7): 553-557.
-
Zariwala M, Schmid S, Pfaltz M, Ohgaki H, Kleihues P, et al. (1994) p53 gene mutations in oropharyngeal carcinomas: a comparison of solitary and multiple primary tumours and lymph-node metastases. Int J Cancer 56(6): 807-811.
-
Shintani S, Yoshihama Y, Emilio AR, Matsumura T (1995) Over expression of p53 is an early event in the tumorigenesis of oral squamous cell carcinomas. Anticancer Res 15(2): 305-308.
- Cancer Diagnosis from RNA Sequence of Blood Cells by Using AI
- Field Cancerization in Oral Cavity, Case Report and Review of Literature. Oncologic Program Salud Integral Hospital, Managua, Nicaragua
- Identification of B Lymphocytes in Cancer Patient’s Blood
- A Case Report of a Breast Cancer Patient Developing Pneumonitis as a Result of Abemaciclib Therapy
- Immune Checkpoint Therapeutics for Today’s Fight and Beyond
- The Amalgamated Sophomore-Gonadoblastoma