Elderly Woman with Synchronous Triple Malignancies of Small Lymphocytic Lymphoma, Multiple Myeloma and Mucosal Malignant Melanoma
Incidence of multiple synchronous cancers in an individual was perceived to be a rare phenomenon however with improved diagnostic and therapeutic modalities more patients are being diagnosed with synchronous primaries. However these patients represent a therapeutic challenge as no standard guidelines exist; and it is the physician’s onus to correctly identify and prioritize treatment based on the expected prognosis and potential for recovery. We present the case of an elderly lady with a complicated clinical scenario where she was diagnosed with SLL/CLL; multiple myeloma and malignant mucosal melanoma; all within the space of a few months. The patient was initially started on chemotherapy for SLL that was subsequently changed to chemotherapy for multiple myeloma and then palliative therapy for melanoma. Patient unfortunately succumbed rapidly to her diseases. This case highlights the fact that that not all laboratory parameters and clinical conditions can be explained by one underlying conditions and physicians need to maintain a high level of suspicion that a patient may have not one but multiple causative etiologies.
Case Summary
A pleasant elderly 63 year old Indian woman with a long-standing history of hypertension on regular medication, presented to us with multiple enlarged lymph nodes in both sides of her neck that had been progressively increasing in size for the last 6-12 months. On physical examination she was found to have generalized lymphadenopathy involving bilateral cervical, supraclavicular, axillae and inguinal regions.
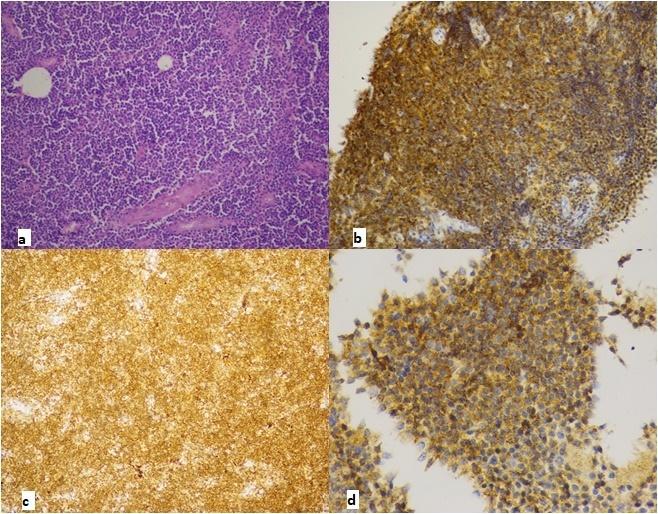
Routine blood investigations revealed hemoglobin 9gm/dL, white blood cell count of 8360 cells/mm3 (neutrophils 60%, lymphocytes 29%) and platelet count 3,46,000 cell/mm3. Serum creatinine was 1.02mg/dL. Liver function test was significant for total protein 8g/dL and albumin 2.16g/dL. M-spike on serum protein electrophoresis (SPEP) was 4.7g/dL. LDH was within normal limits. Incisional biopsy of the left supraclavicular lymph node was reported as non hodgkin’s lymphoma. Immunohistochemistry evaluation was done and showed tumor cells positive for CD20, CD43, BCL-2 with Ki-67 index less than 10% suggestive of low grade mature B-cell neoplasm favoring B cell chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL) (Figure 1). Patient underwent positron emission tomography–computed tomography (PET- CT) which was suggestive of extensive lymphadenopathy with mild FDG uptake (maximum SUV 5.63) (Figure 2). Bone marrow also had diffuse mild FDG uptake (maximum SUV 3.68) suggestive of involvement. Additional myeloma evaluation including immune-fixation electrophoresis revealed the presence of IgG kappa monoclonality. Serum free light chains showed marked elevation of kappa free light chains (423mg/L) and elevated IgG (7354mg/dL). Bone marrow aspiration and biopsy showed around 10% plasma cell and 10% of lymphoid cells. FISH analysis for multiple myeloma (MM) was negative for p53 del, 13q del, t(4;14), t(11;14) and t (14;16) (Table 1).
| Hemoglobin | 9gm/dL | ||
|---|---|---|---|
| Complete Blood Count | TLC | 8360 cells/mm3 (Neutrophils 60%, Lymphocytes 29%) | |
| Complete Blood Count | Platelets | 3,46,000 cells/mm3 | |
| Complete Blood Count | Liver Function Test | Total Protein | 8g/dL |
| Albumin | Liver Function Test | 2.16g/dL | |
| LDH | Liver Function Test | 195 U/L | |
| Renal Function | Serum Creatinine | 1.02mg/dL | |
| Immunoglobulin Level | IgG | 7354 mg/dL | |
| Immunoglobulin Level | IgM | 21 mg/dL | |
| Immunoglobulin Level | IgA | 58 mg/dL | |
| Serum Free Light Chains | Kappa | 423 mg/dL | |
| Serum Free Light Chains | Lambda | 9.5 mg/dL | |
| SPEP | M-spike | 4.7 mg/dL |
Table 1: Initial Lab reports at presentation.

an upper gastrointestinal endoscopy that revealed the presence of a growth in the mid esophagus which was biopsied (Figure 3). This biopsy was positive for malignant mucosal melanoma which was confirmed by immunohistochemistry (the tumor cells were positive for HMB45, S100, Melan A with Ki-67 proliferation index of 70%) (Figure 4). Re-imaging was done with a contrast enhanced CT scan of thorax that showed a large subcarinal mass causing compression and narrowing of esophageal lumen (Figure 5). Cervical, supraclavicular, mediastinal and axillary lymph nodes had decreased in size as compared to previous PET-CT scan. Repeat serum protein electrophoresis showed an increase in M-spike to 6.52g/dL which suggested no response to the current myeloma treatment protocol.


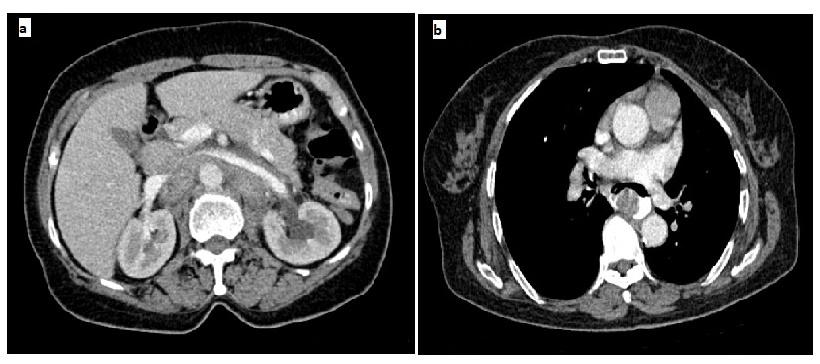
b) While stable esophageal lesion in subcarinal region.
Patient at this time refused further intravenous chemotherapy and opted for best supportive care. She was started on palliative temozolamide, and received two cycles of the same. After two cycles the M-spike increased to 6.96g/dl. Her swallowing function did not worsen further and restaging CT scans showed stable esophageal lesion but increase in size of gastrohepatic node. The lymph nodes in the axillary, mediastianum and reteroperitoneum had decreased in size. She was continued on best supportive care thereafter but passed away within a month of the last staging scans.
Discussion
The presence of multiple synchronous primary malignancies in an individual is rare. Even rarer is the simultaneous presence of both hematological and solid tumors. To our knowledge there has only been one previous report in literature of a patient with B-cell CLL, malignant melanoma and multiple myeloma [1]. However with improved diagnostic and therapeutic modalities more patients are being diagnosed with synchronous primaries.
SLL/CLL is often an incidental diagnosis and most of these cases do not require treatment upfront. However patients with SLL/CLL have an increased risk of secondary cancers [2, 3]. The relationship between these cancers is poorly understood. Patients with CLL have a higher incidence of melanoma and those with melanoma who have CLL have a higher mortality as compared to those who do not have underlying CLL [4]. The association of multiple myeloma and CLL is complex as they represent separate driver mutations at the hematopoietic stem cell level, resulting in a different set of B cell clonal expansion.
Determining a therapeutic strategy that would target the co-existing malignancies is a formidable task as the pathophysiology leading to development of concurrent malignancies is poorly understood. The preference would be to select a regimen that would be efficacious for all the existing cancers; however there are very few drugs that can claim such an efficacy. In our patient it was difficult to ascertain whether her progressive anemia, hypoalbuminemia and general malaise could be attributed to the SLL/CLL or the MM as there is a general overlap in the signs and symptoms of both these diseases. We opted initially to treat SLL/CLL due to her B- symptoms, but we had to shift to the treatment of MM as there was a rapid increase in the M-protein. Despite the use of standard chemotherapy regimens she did not respond to therapy. Once we diagnosed her to with esophageal malignant mucosal melanoma and started her on palliative temozolamide she stabilized temporarily before succumbing to the disease.
Several molecular mechanisms and genetic alterations resulting in primary resistance to bortezomib and lenalidomide have been proposed [5, 6, 7]. One common association noted in both MM and CLL patients is the increased concentration of hepatocyte growth factor (HGF) [8, 9] and harnessing the HGF/MET pathway by using a MET kinase inhibitor may be a potential target to overcome bortezomib/lenalidomide resistance [10]. Serum HGF levels are also elevated in metastatic melanoma and correlate with progression free and overall survival, and hence there may also a potential role for MET inhibitors in metastatic melanoma. There is also data to suggest that MEK inhibitors may co-target the HGF/MET pathway in mucosal melanoma [11, 12].
There are several lessons that we learnt from this patient. In medicine we are usually taught that one unifying diagnosis should be sought to explain all the clinical scenarios in an individual patient. However this did not apply to our patient and had we been more aggressive we may have identified all the cancers upfront immediately, instead of diagnosing them sequentially over the course of a few months which was demoralizing for both the patient and the treating team. It would therefore serve us well in the future to maintain a high level of suspicion for the possibility of multiple cancers especially if the presenting signs and symptoms, laboratory findings and diagnostic imaging do not correspond to our knowledge of what is the usual pattern for that disease.
In retrospect, with a diagnosis of multiple primary malignancies where standard of care does not exist we could have utilized next generation sequencing to identify underlying genetic mutations that may not only have elucidated the reason for this rare phenomenon but may also have provided us rationale therapeutic targets. Precision medicine therefore should be incorporated upfront for these challenging and unusual cases as this would help us to personalize systemic therapy by improving efficacy without increasing toxicity for best clinical outcome.
References
-
(1975) Multiple malignancies: Chronic lymphocytic leukemia, malignant melanoma, multiple myeloma and acute myelomonocytic leukemia. The American Journal of Medicine 58(3): 408-416.
-
Royle JA, Baade PD, Joske D, Girschik J, Fritschi L (2011) Second cancer incidence and cancer mortality among chronic lymphocytic leukaemia patients: a population-based study. Br J Cancer 105(7): 1076- 1081.
-
Wiernik PH (2004) Second neoplasms in patients with chronic lymphocytic leukemia. Curr Treat Options Oncol 5(3): 215-223.
-
Famenini S, Martires KJ, Zhou H, Xavier MF, Wu JJ (2015) Melanoma in patients with chronic lymphocytic leukemia and non-Hodgkin lymphoma. J Am Acad Dermatol 72(1): 78-84.
-
Amatangelo MD, Neri P, Ortiz M, Bjorklund CC, Gandhi AK, et al. (2015) Resistance to Lenalidomide in Multiple Myeloma Is Associated with a Switch in Gene Expression Profile. Blood 126 (23): 1789.
-
Nikesitch N, Ling SCW (2016) Molecular mechanisms in multiple myeloma drug resistance. J Clin Pathol 69(2): 97-101.
-
Shiqiao Ye, Wei Qiang, Yu Chen, Bo Hu, Qing Zhang, et al. (2013) MAF Protein Elicits Innate Resistance to Bortezomib in Multiple Myeloma. Blood 122 (21): 281.
-
Giannoni P, Pietra G, Travaini G, Quarto R, Shyti G, et al. (2014) Chronic lymphocytic leukemia nurse-like cells express hepatocyte growth factor receptor (c- MET) and indoleamine 2,3-dioxygenase and display features of immunosuppressive type 2 skewed macrophages. Haematologica 99(6): 1078-1087.
-
Seidel C, Børset M, Turesson I, Abildgaard N, Sundan A, et al. (1998) Elevated Serum Concentrations of Hepatocyte Growth Factor in Patients with Multiple Myeloma. Blood 91(3): 806-812.
-
Zaman S, Stellrecht CM, Orlowski RZ, Gandhi V (2014) Bortezomib and lenalidomie resistant myeloma cells overexpress the hepatocyte growth factor/MET signaling axis and respond to MET kinase inhibitors. Cancer Res 74(19): 1710.
-
Hügel R, Muendlein A, Volbeding L, Drexel H, Richtig E, et al. (2016) Serum levels of hepatocyte growth factor as a potential tumor marker in patients with malignant melanoma. Melanoma Res. 26(4): 354-360.
-
Cheng H, Chua V, Liao C, Purwin TJ, Terai M, et al. (2017) Co-targeting HGF-cMET signaling with MEK inhibitors in metastatic uveal melanoma. Mol Cancer Ther 16(3): 516-528.
- Cancer Diagnosis from RNA Sequence of Blood Cells by Using AI
- Field Cancerization in Oral Cavity, Case Report and Review of Literature. Oncologic Program Salud Integral Hospital, Managua, Nicaragua
- Identification of B Lymphocytes in Cancer Patient’s Blood
- A Case Report of a Breast Cancer Patient Developing Pneumonitis as a Result of Abemaciclib Therapy
- Immune Checkpoint Therapeutics for Today’s Fight and Beyond
- The Amalgamated Sophomore-Gonadoblastoma