The Mesocolon, the Surgical Anatomy and Optimization of Resection, A Review of Literature
Colorectal cancer is one of the most common cancers worldwide, in this article we will discuss the history of anatomic approach of the colorectal cancer, the surgical importance of the mesentery of the colon, how to approach the surgical resection of the colon with maximizing the lymph nodes harvest targeting the lympho vascular sheet contained within the mesentery.
The Concept of Total Mesocolic Excision
Recent advances in the management of colon cancer identify TOTAL MESOCOLIC EXCISION as a potential determinant of both overall and disease specific survival following radical resection. In 2009, Prof. Hohenberger proposed complete mesocolic excision (CME) as a standardized surgical technique, in which the same principle of total mesorectal excision (TME) in rectal cancers is to be applied to the colon. He recommended that the surgery being performed using a proper anatomic plane based on an embryonic anatomy which is a high- quality radical operation harvestingan optimal oncologic pathological specimen, especially in the retroperitoneal colon (Figure 1) [1].

The Mesentery of The colon and rectum is the adult vestige of the dorsal mesentery, in which the colon was suspended from the posterior abdominal wall during intrauterine development [2].
Current embryological teaching is based on the anatomic findings of Sir Frederick Treves and Tolds that the dorsal mesentery of the right and left colon became opposed to the posterior abdominal wall by a process of ‘obliteration’ [3]. The right and left mesocolon are then ‘fused’ through a process of ‘integration’ with the retroperitoneum. Treves identified ‘a mesocolon’ on the left side in 36% and on the right side in 26% of all cadavers he examined [4].
Given that the transverse and sigmoid mesocolon persist into adulthood, the implication is that the mesocolon is thus incomplete in adulthood [5]. In keeping with this, the ascending and descending colon are frequently erroneously described as retroperitoneal [6].
In contrast, surgical mobilization of the colon relies on a continuous mesentery and entering a plane between the colon and retroperitoneum [7]. Continuing mobilization towards the midline separates a fatty structure in which vessels supplying the colon and associated lymph nodes are contained. Thus Goligher described colonic mobilization as ‘stripping the mesentery back towards the midline’ and the ‘no touch’ technique of Turnbull emphasized the same approach [8].
Surgical findings reflect those of Carl Toldt, who proposed in 1919 the mesentery of the right and left colon persist into adulthood and they remain separated from the posterior abdominal wall by a connective tissue plane he termed the lamina mesenteriapropria (later called ‘Toldt’s fascia of fusion’ by Goligher) [9].
Toldt’s findings were separately confirmed by Congdon and Zuckerandle, and conform more closely to surgical findings than the descriptions laid out by Treves [10].
An anatomical confluence was always evident between the terminal ilealmesentery and the right mesocolon, and this was termed the ileocaecalmesenteric confluence (ICMC). The ileocaecalmesenteric confluence is variable in opposition to the retroperitoneum; in some patients it is not adherent and could thus be described as ‘mobile’. In the remaining patients it was opposed to the retroperitoneum and thus ‘non- mobile [11].
In 50% of patients peritoneal adhesions occurred between the fourth part of the duodenum and adjacent areas of left and transverse mesocolon [11]. While the left mesocolon is fully adherent to the retroperitoneum, this is only the case with the medial portion of the mesosigmoid; the lateral portion being mobile. Amesenteric confluence occurred at ileocaecal and rectosigmoid junction as well as at hepatic and splenic flexure. By addressing these anatomical features through “meso-fascial” separation the entire colon and mesocolon can be mobilized intact [11].
Total mesocolic excision appears to be associated with improved survival in patients undergoing colectomy for colon cancer, when the colon and its mesentery, including the lymphovascular supply, are resected together as an intact package [1].
Importance of the Fascias Posterior to the (Non-Mobile) Colon and Associated Mesentery in Colonic Surgery
In 1982, Prof. Heald proposed TME as the standardized radical operation for rectal cancer, which involves a sharp dissection along embryological anatomical planes - namely, with a sharp separation of the visceral fascia from the parietal plane [12].
The survival rate for rectal cancer has improved and is even higher than that of colon cancer because of the development and global use of TME [12, 13].
A similar process could now be implicated with the greater understanding of colon cancer treatment using complete mesocolicexcision (CME). Prof. Hohenberger proposed the colon and its mesentery, like mesorectum are surrounded by visceral fascia, with the sharp separation of the visceral fascia from the parietal plane leading to a ‘properly resected’ specimen with intact coverage, including the majority of the regional lymph nodes, the lymph vessels, and the surrounding fat tissue lying within the mesocolon [1].
The classic anatomy definitions stated the interperitoneal colon had no mesocolon, since the posterior lobe of the mesocolon (visceral fascia) integrated with a deep structure (parietal fascia) during embryonic development. However, in the era of modern surgical anatomy, more attention has been paid to the sharp dissection of spaces composed of loose connective tissue following the embryological anatomical planes in the abdominal and pelvic cavity. As early as 100 years ago, Prof. Gerota described the presence of a prerenal fascia in the rear of the colonic adipose by examining frozen sections of corpses for the first time [14].
A study done by Zhidong and colleagues showed that the original visceral and parietal fascias could be recovered by sharp separation, despite the fusion of these fascias during embryonic development. The fascia structure became composed of collagen fibers in the retrocolon and formed the posterior lobe of the mesocolon during this developmental period Figure 2 [15].

This layer of the fascia and the prerenal fascia constitute the retrocolic space, which is filled with loose connective tissue such as angel’s hair, and can serve as a surgical level for CME. Meanwhile, the in vitro transwell assays showed that the visceral fascia was a natural barrier to the migration of tumor cells [15]. Therefore, surgery at this level of the visceral and parietal fascia could ensure the maximum possible removal of the regional lymphnodes [15].
The anatomical and histopathological findings showed that the fascias posterior to the interperitoneal colon and its associated mesocolon were composed of two independent layers: the visceral and parietal fascias. These two fascias were primarily composed of collagen fibers, with the parietal fascia containing a small amount of muscle fiber [15].
After the sharp incision at Toldt’s line, the potential surgical plane formed between the mesocolon and the underlying retroperitoneum was easy to find. By a sharp dissection following the areolar tissue ‘angel’s hair’ and complete mobilization of the entire mesocolon, the intact fascias were clearly seen, covering the posterior mesocolon (visceral fascia layer) and the retroperitoneal organs, including the vena cava, aorta, ureter, and genital vasculature (parietal fascia layer). No vascular, lymphatic, or nerve distribution was evident in this plane. The visceral fascia became gradually denser laterally and inferiorly Figure 3 [15].
There is a great deal of discussion and debate regarding whether the CME concept is new. The CME technique was introduced in the West in 2008, but Japanese, Chinese, Korean and Taiwanese surgeons have used D3 lymphadenectomy resections for colon cancer for decades. The D3 lymphadenectomy is defined as the dissection of the paracolic, intermediate and central lymph nodes, a procedure equivalent to CME [16].
Complete Mesocolic Excision as a Laparoscopic Procedure
CME is a more extensive operation than a standard procedure. Originally CME was described as an open procedure [1], although many centers prefer performing laparoscopic surgery, with its associated benefits [17] and similar oncological outcomes, as the standard treatment for colonic cancer.
A small comparison study between laparoscopic and open CME approaches concluded that laparoscopy offers specimens of similar quality to the open CME approach in terms of lymph node harvest, rate of achievement of an intact mesocolic plane, and distance from high tie to tumor and high tie to nearest bowel wall in proximal right- and left-sided resections. However, for transverse and hepatic fexure tumors, the open CME group had better outcomes in distance from tumor to high tie and nearest bowel wall to high tie compared to the laparoscopic group [18]. Similar oncological results were found in a prospective study from Norway that compared laparoscopic to open CME. The 3-year overall survival rate (80.4% vs 88.2%, P = 0.152) and disease free survival rate (74.8% vs 80.0%, P = 0.405) were similar [19].
CME is a longer operation [20], which may lead to increased morbidity, but it does reduces the efficiency of an operating theater and influence the health economy [16]. The duration of surgery remains one of the largest obstacles for laparoscopic CME [20]. The operative duration learning curve reveals an initial duration of approximately 250 min, which is more than double the duration reported for a conventional laparoscopic right hemicolectomy performed by experienced laparoscopic surgeons [21].
Even though CME is a more extensive procedure, mortality and complication rates are in acceptable ranges. In a systematic review [22], overall morbidity, 30-d mortality and re-operative intervention for vascular complications were 19.4%, 3.2% and 1.1% respectively and mean blood loss was 150 mL, all comparable to the reported contemporary series for “standard” resections [23]. However, unusual complications, such as chyle leakage [24], duodenal injury [25] and major vascular injury [26] have been reported.
Surgical Opinion
Complete Mesocolic Excision is not a new concept, and many surgeons are doing it in their daily surgeries by approaching the mesentry in a smooth anatomically identified plane. The oncologic benefit from maximizing the lymph nodes harvest is the target which is well established finding.
Surgeons have observed the presence of loose areolar connective tissues between the interperitoneal colon and the prerenal fascia (Gerota’s fascia) covering the ureters and the kidneys. The colon and its associated mesentery could be resected completely by performing the operation at this anatomic potential plane by sharp dissection assisted by traction and counter-traction way.
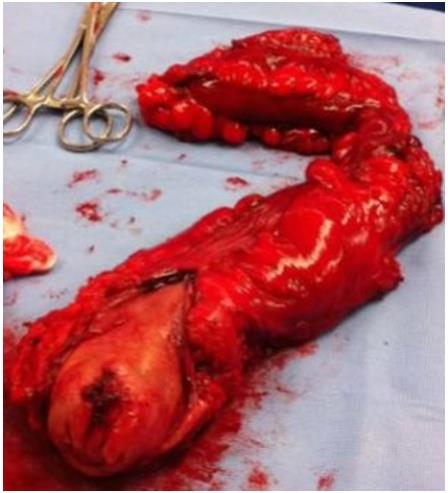
The gross picture of the postoperative specimen should show an intact, smooth, thin, and transparent fascia (visceral fascia) covering the posterior surface of the right or left colon with its mesentery, by this way , we can identify the completeness of the resection of the colonic part harboring the tumor.
Conclusion
Thorough understanding of the relationship between the Colon, rectum and the surrounding fasciae, professional identification of the embryological origin and anatomic variations of these structures are of great benefit to improve oncologic outcomes in resecting cancers of the colon and rectum. The visceral and parietal fasciae have been extensively identified and described in embryological studies, by keeping updated on the latest advances in the treatment and approaching colorectal cancers, surgeons are able to maximize their oncological resection outcomes when operating on patients with colorectal cancer.
The concept of CME and the new anatomical characteristics of the mesocolon, as described by Culligan et al [5], offer a great opportunity to re-evaluate colon cancer surgery. The principles under-lying CME are anatomical and logical, and the results published from the Far East, reporting an 80% 5 year survival rate for stage III disease [24], should guide us. Further determination of the benefits of the complete mesocolic excision in comparison with the standard colon surgery need to be further evaluated by RCTs.
References
-
Hohenberger W, Weber K, Matzel K, Papadopoulos T, Merkel S (2009) Standardized surgery for colonic cancer: complete mesocolicexcision and central ligation--technical notes and outcome. Colorectal Dis 11: 354-365.
-
Brookes M, Zietman A (2000) Alimentary tract. In: Clinical Embryology, a Color Atlas and Text. Brookes M, Zietman A (Eds.), CRC press, Florida, pp: 148-152.
-
Gallot D (2008) Anatomie chirurgical educoˆlon. In: Techniques Chirurgicales-Appareil Digestif. pp: 40- 535.
-
Treves SF (1885) Lectures on the anatomy of the intestinal canal and peritoneum in man. Br Med J 1(1264): 580-583.
-
McMinn RH (1994) The gastrointestinal tract. In: Last‘s Anatomy: Regional and Applied, 9th (Edn.), McMinn RH (Eds.), Langman Group Ltd, London, pp: 331-342.
-
Agur AMR (1998) The abdomen. In: Grant‘s Atlas of Anatomy, Agur AMR (Eds.), Williams and Wilkins, New York, pp: 77-147.
-
Standring S (2008) Large intestine. In: Gray’s Anatomy: The Anatomical Basis of Clinical Practice, 40th (Edn.), Standring S (Eds.), Churchill Livingstone, Philadelphia, pp: 1137.
-
Goligher J. Treatment of carcinoma of the colon. In: Surgery of the Anus, Rectum and Colon, 5th (Edn.), Goligher J (Eds.), Balliere Tindall, London, pp: 485-589.
-
Toldt C (1919) An Atlas of Human Anatomy for Students and Physicians. Rebman Company, New York, pp: 407-409.
-
Congdon ED, Blumberg R, Henry W (1942) Fasciae of fusion and elements of the fused enteric mesenteries in the human adult. Am J Anat 70: 251-279.
-
Culligan K, Coffey JC, Kiran RP, Kalady M, LaveryI C, et al. (2012) The mesocolon: a prospective observational study. Colorectal Dis 14(4): 421-428.
-
Heald RJ, Husband EM, Ryall RD (1982) The mesorectumin rectal cancer surgery – the clue to pelvic recurrence. Br J Surg 69(10): 613-616.
-
Siegel R, Naishadham D, Jemal A (2012) Cancer Statistics, 2012. CA Cancer J Clin 62(1): 10-29.
-
Gerota D (1895) Beitrage zur Kenntnis des Befestigungsapparates der Niere. Arch Anat Entwicklungsgesch 19: 265-286.
-
Gao Z, Ye Y, Zhang W, Shen D, Zhong Y, et al. (2013) An anatomical, histopathological, and molecular biological function study of the fascias posterior to the interperitoneal colon and its associated mesocolon: their relevance to colonic surgery. J Anat 223(2): 123- 132.
-
Chow CF, Kim SH (2014) Laparoscopic complete mesocolic excision: West meets East. World J Gastroenterol 20(39): 14301-14307.
-
Sun YW, Chi P, Lin HM, Lu XR, Huang Y, et al. (2012) Comparison of efficacy between laparoscopic versus open complete mesocolic excision for colon cancer. Zhonghua Weichang Waike Zazhi 15(1): 24-27.
-
Gouvas N, Pechlivanides G, Zervakis N, Kafousi M, Xynos E (2012) Complete mesocolic excision in colon cancer surgery: a comparison between open and laparoscopic approach. Colorectal Dis 14(11): 1357- 1364.
-
Storli KE, Søndenaa K, Furnes B, Eide GE (2013) Outcome after introduction of complete mesocolic excision for colon cancer is similar for open and laparoscopic surgical treatments. Dig Surg 30(4-6): 317-327.
-
Melich G, Jeong DH, Hur H, Baik SH, Faria J, et al. (2014) Laparoscopic right hemicolectomy with complete mesocolic excision provides acceptable perioperative outcomes but is lengthy--analysis of learning curves for a novice minimally invasive surgeon. Can J Surg 57(5): 331-336.
-
Senagore AJ, Delaney CP, Brady KM, Fazio VW (2004) Standardized approach to laparoscopic right colectomy: outcomes in 70 consecutive cases. J Am Coll Surg 199(5): 675-679.
-
Bertelsen CA, Neuenschwander AU, Jansen JE, Wilhelmsen M, Tenma JR, et al. (2015) Disease- free survival after complete mesocolic excision compared with conventional colon cancer surgery: a retrospective, population- based study. Lancet Oncol 16(2): 161-168.
-
Ma Y, Yang Z, Qin H, Wang Y (2011) A meta-analysis of laparoscopy compared with open colorectal resection for colorectal cancer. Med Oncol 28(4): 925- 933.
-
Shin JW, Amar AH, Kim SH, Kwak JM, Baek SJ, et al. (2014) Complete mesocolic excision with D3 lymph node dissection in laparoscopic colectomy for stages II and III colon cancer: long-term oncologic outcomes in 168 patients. Tech Coloproctol 18(9): 795-803.
-
Feng B, Sun J, Ling TL, Lu AG, Wang ML, et al. (2012) Laparoscopic complete mesocolic excision (CME) with medial access for right-hemi colon cancer: feasibility and technical strategies. Surg Endosc 26(12): 3669-3675.
-
Han DP, Lu AG, Feng H, Wang PX, Cao QF, et al. (2013) Long-term results of laparoscopy-assisted radical right hemicolectomy with D3 lymphadenectomy: clinical analysis with 177 cases. Int J Colorectal Dis 28(5): 623-629.
- Cancer Diagnosis from RNA Sequence of Blood Cells by Using AI
- Field Cancerization in Oral Cavity, Case Report and Review of Literature. Oncologic Program Salud Integral Hospital, Managua, Nicaragua
- Identification of B Lymphocytes in Cancer Patient’s Blood
- A Case Report of a Breast Cancer Patient Developing Pneumonitis as a Result of Abemaciclib Therapy
- Immune Checkpoint Therapeutics for Today’s Fight and Beyond
- The Amalgamated Sophomore-Gonadoblastoma