Screening for Colorectal Cancer: Thoughts of a Surgeon
Image Article
Colorectal cancer is the second leading cause of cancer-related deaths in the world after lung and breast cancer [1]; in Spain every week 500 new cases are diagnosed and it is estimated that 1/20 men and 1/30 women will develop colorectal cancer before 75 years age [2].
Image Article
In the Basque Country, 1700 new cases are diagnosed every year and the average incidence is 46,3/100.000 hab in colon cancer and 28,4/100.000 in rectum, and 60% of them are detected in stages III-IV. The screening program for colorectal cancer fulfills the Wilson and Jungner screening criteria:
![Figure 1: Work flow of the Basque Colorectal Cancer Screening Programme [4].](/fulltextimages/6594/fig_1.jpeg)
Different authors correlate the screening programs with a descent in mortality and morbidity rates [3]; thus, screening for colorectal cancer (CCR) is widely accepted; however, there are significant differences among the numerous programs led in the world. The population targeted, the faecal blood test and the extension of the endoscopy (colonoscopy or flexible sigmoidoscopy) are the main estrategic variabilities. But there is also another important factor to take into account that can make a change in the results of the screening program: the participation rate. Despite the unquestionable benefits of these programs, people still find the CCR screening strange, distant, and dispensable from their health care. Furthermore when the program includes an invasive and not without risks procedure as an endoscopy.
The main objective of the CCR screening program is the reduction in mortality rates; but not only is this benefit found. In fact, subclinical benign diseases are diagnosed and it is possible to detect and treat simultaneously premalignant lesions. The population-based Basque Colorectal Cancer (CRC) Screening Programme started in 2009 with a biennial immunochemical quantitative test (FIT) (Image 2). A complex and multidisciplinary coordinating office selected the target population; individuals with a previously-diagnosed CRC, terminal illness and reported colonoscopy in the past five years were excluded. The population target of 586,700 residents was from 50 to 69 years old and the total coverage was reached at the beginning of 2014.
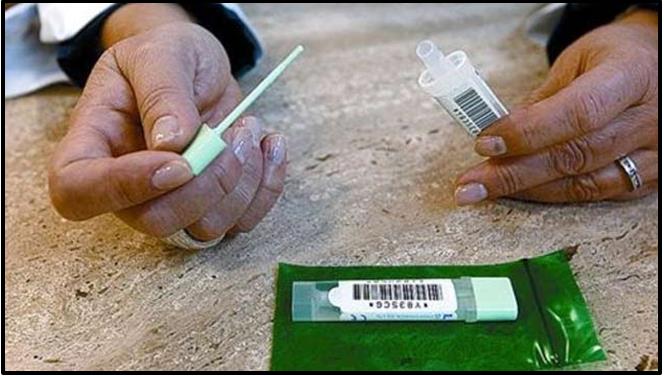
Image 2: FIT test.
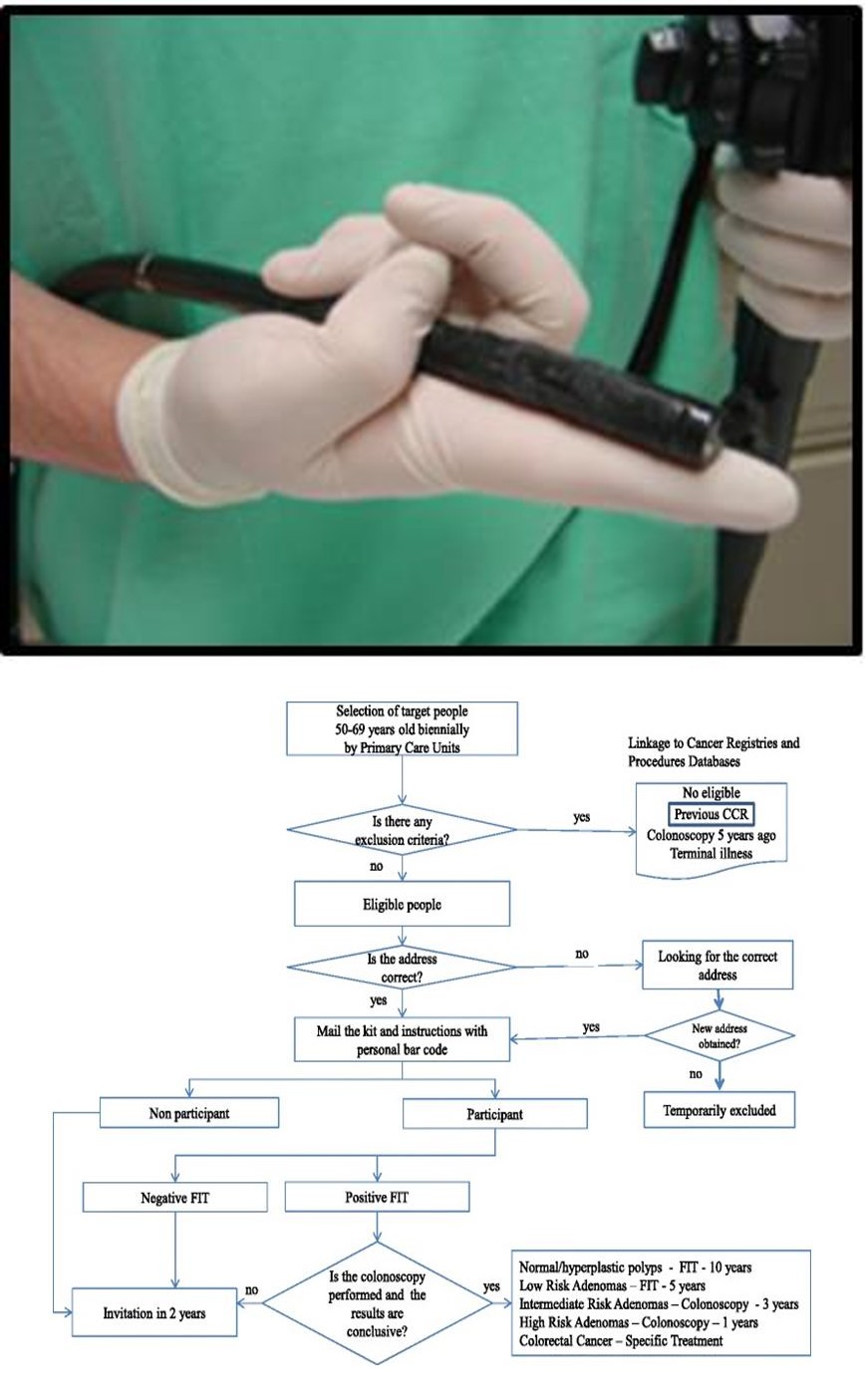
Image 3: Flexible Colonoscope. The coordinating office individualized posts invitations providing information about the Programme (figure 1).
After 6-8 weeks from the initial invitation, the kit (FIT) is sent along with instructions and individualized bar code. This bar code allows the sample and person to be identified when processing the result. Samples are collected at primary health centers and processed in centralized public laboratories under strict and total quality management systems; all results are reviewed by primary care physicians and introduced in “ad hoc” CRC prevention software. Letters are posted with results. In positive cases, participants are recommended to visit their general practitioner, who refers them to the hospital for colonoscopy. Our hospital, Asuncion Klinika, is one of the centers in which colonoscopies (diagnostic and therapeutic if needed) are performed under deep sedation by specialists. All cases are followed-up with close coordination between primary care and specialized units; interval cancer and complications are identified and monitored by registries linkage before invitation and after colonoscopy performance.
Asuncion Klinika is the referral hospital of a region with about 48000 habitants. The department of General Surgery is part of the screening program for CCR with the collaboration and surveillance of the Health Department of the Basque Country. In our experience, the proximity, feasibility and accessibility to the hospital has been an important factor to develop the program. Different countries have developed the CCR screening program with low participation rates as Croatia with 19,9%, Ireland with 51%, , England 52% or France 34,3% [1]. Our participation rates were 65% when first implanted in 2012, until today, with 75%. Our latest colonoscopy acceptance rate has been over 90% and about 60% of the cancers detected in our program were stage I-II. These outcomes are not only based on a good strategy or design of the program; the intense effort of the primary care physicians, the continuous work on acculturating the population, spreading information and getting the hospital closer to the people have been the key to our success. Another peculiarity of our hospital is that the colonoscopies are performed by surgeons with wide experience in endoscopy. We not only contribute to the accomplishment of the CCR prevention, but also gain quickness in case surgery is needed. At the time the colonoscopy is performed, if an endoscopically non- removable tumour is detected, the patient is referred to our outpatient visit in a maximum time frame of 72 hours. If histology is malignant, the patient undergoes surgery within 20 to 27 days after the initial colonoscopy. This short period of time rests anxiety to the patient. Another benefit is that many times, the same surgeon that performs the colonoscopy is the one to examine the patient in the medical visit, explains the diagnose and does the surgery, what brings security, reliability and familiarity to the patient. Some authors have analyzed the quality of the colonoscopy when performed by gastroenterologists or colorectal surgeons, reaching the conclusion that the adenoma detection rate (ADR) was not significantly different between both specialities [5]. So, why not offering these patients a colonoscopy with the point of view of a surgeon?
References
-
Navarro M, Nicolas A, Ferrandez A, Lanas A (2017) Colorectal cancer population screening programs worlwide in 2016: an update. World J Gastroenterol 23(20): 3632-3642.
-
Morillas JD, Castells A, Oriol I, Pastor A, Pérez-Segura P, et al. (2012) The Alliance for the Prevention of Colorectal Cancer in Spain. A civil commitment to society. Gastroenterol Hepatol 35(3): 109-128.
-
Portillo I, Arana-Arri E, Idigoras I, Bilbao I, Martínez- Indart L, et al. (2017) Colorectal and interval cancers of the colorectal cancer screening program in the Basque Country (Spain). World J Gastroenterol 23(15): 2731-2742.
-
Idigoras I, Arrospide A, Portillo I, Arana-Arri E, Martínez-Indart L, et al. (2017) Evaluation of the colorectal cancer screening Programme in the Basque Country (Spain) and its effectiveness based on the Miscan-colon model. BMC Public Health 18(1): 78.
-
Lee AHH, Lojanapiwat N, Balakrishnan V, Chandra R (2018) Is there a difference in adenoma detection rates between gastroenterologists and surgeons? World J Gastrointest Endosc 10(6): 109-116.
- Cancer Diagnosis from RNA Sequence of Blood Cells by Using AI
- Field Cancerization in Oral Cavity, Case Report and Review of Literature. Oncologic Program Salud Integral Hospital, Managua, Nicaragua
- Identification of B Lymphocytes in Cancer Patient’s Blood
- A Case Report of a Breast Cancer Patient Developing Pneumonitis as a Result of Abemaciclib Therapy
- Immune Checkpoint Therapeutics for Today’s Fight and Beyond
- The Amalgamated Sophomore-Gonadoblastoma