Acute Renal Failure Due to Vitamin C: Case Report and Review of the Literature
1.1. Background: Vitamin C is an essential dietary nutrient that is necessary for normal growth and development. The endpoint product of vitamin C metabolism, oxalate, is excreted by the kidney and is nephrotoxic. Deposition of oxalate crystals in renal tubules can cause tubular necrosis and result in acute renal injury. 1.2. Case Presentation: This article presents an 80-year-old patient with acute renal failure due to oxalate nephropathy associated with oral vitamin C intake and reviews oxalate nephropathy. Our case emphasizes renal function monitoring in patients receiving long-term vitamin C especially with a history of renal disease. Over consumption of vitamin C can lead to acute kidney injury. Patients under nephrotoxic treatments are at risk for acute kidney injury from a high vitamin C diet and should be suspected in unexplained renal insufficiency. 1.3. Conclusion: Careful review of diets and all medications is necessary when confronted with unexplained renal insufficiency. Closely monitoring renal function is recommended in patients on high vitamin C.
Introduction
Vitamin C (ascorbic acid) is a water-soluble essential nutrient identified in the 1930s as a consequence of the search for a substance, the deficiency of which causes scurvy. It has been hypothesized that Vitamin C may reduce the incidence of most malignancies in humans [1] probably through its antioxidant properties including the neutralization of free radicals [2, 3]. First studies showed that high-dose intravenous vitamin C increased the average survival of advanced cancer patients [4, 5, 6]. However, subsequent studies didn’t reproduce that benefit [7, 8]. Oxalate is a major end product of ascorbic acid metabolism, which is excreted in urine [9, 10, 11]. Previous reports have described the acute oxalate nephropathy in association with excessive vitamin C intake of greater than 2 grams/day. Here we present a cancer patient with oxalate-induced acute renal failure that was attributable to consumption of vitamin C supplement. We discuss the cause of calcium oxalate nephropathy following a review of the literature.
Case Report
An 80-year-old Caucasian man with past medical history of metastatic cholangiocarcinoma presented to our emergency department with complaints of nausea, vomiting, and inability to orally intake over the past several days. His disease was stable with no active treatment for his cancer for the last year. He had elevated bilirubin which was related to a biliary stent malfunction. He underwent stent exchange with improvement. On physical examination, he appeared volume depleted. Body temperature, blood pressure, pulse rate, respiratory rate, and SpO2 on room air were 36.5 °C, 163/69 mmHg, 50 beats/min, 18 breaths/min, and 99%, respectively. His buccal mucosa was dry. There was a mild tenderness with deep palpation of the epigastric region. The physical examination was otherwise unremarkable. His family history was unremarkable. The rest of his medical history included coronary artery disease with the history of CABG, previous upper respiratory infection, and right rotator cuff injury. The patient never had any prior kidney disease. His medication included thyroid supplementation, multivitamin, vitamin B and vitamin C two grams daily.
On admission, his laboratory tests showed WBC count 6.0 k/ul, hemoglobin 10.3g/dl, platelet count 250K/ul, BUN
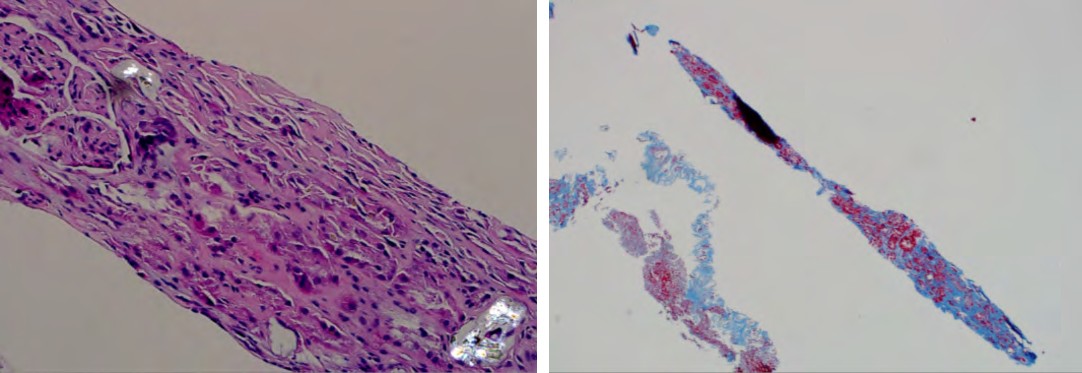
88mg/dl, and creatinine 7.03mg/dl (baseline creatinine 0.65mg/dl), Sodium 122meq/L, potassium 6meq/L, chloride 91meq/L, carbon dioxide 20meq/L, magnesium 2.6meq/L, total bilirubin 2.5mg/dl, indirect bilirubin 1.5mg/dl, direct bilirubin 1mg/dl, alkaline phosphatase 575 IU/L, LDH 615IU/L, and ALT 54IU/L, AST 44IU/L, total protein 6.7, albumin 3.4g/dL, calcium 8.4meq/L, phosphorus 8meq/L, and glucose 66mg/dl. His urinalysis revealed trace protein and leukocyte esterase, 2-5 RBCs per high power field, and 2-5 WBCs per high power field. Ultrasonography of kidneys showed normal sized kidneys with no hydronephrosis. There was an abnormal appearance with prominent pyramids and increased echogenicity in the renal parenchyma. Upon admission, he was initiated intravenous hydration 150 mL of normal saline per hour, kayexalate 30 grams for two doses, and Zosyn 2.25grams intravenous every 8 hours. Despite aggressive intravenous hydration, the level of serum creatinine did not improve and increased to 8.7 mg/ dL, therefore he underwent hemodialysis and continued to require it for three months at which point had renal recovery. A renal biopsy was performed and revealed mild to moderate tubulointerstitial fibrosis with numerous calcium oxalate crystals with an average of approximately 6 crystal deposits present per glomerulus (Figures 1A & 1B).
A B Figure 1A: H&E-cross polarized light: focal birefringent crystals consistent with calcium oxalate. Figure 1B: Trichrome: mild to moderate interstitial fibrosis.
Discussion
Oxalate arises in the body from a combination of dietary sources and endogenous production from precursors. Hyperoxaluria considered being a primary risk factor for calcium oxalate stones, which are present in up to 75% of patients diagnosed with renal lithiasis [12, 13]. Additionally it may cause deposition of calcium oxalate crystals in the kidney and result in the variable degrees of atrophy and inflammatory reaction. In setting of decreased tubular flow calcium oxalate crystals causes luminal obstruction with an increase in cytokine release leading to cell death, tubular atrophy and eventual fibrosis. With decreased calcium oxalate clearance perpetuates for further precipitation in the tubules and continued irreversible damage [14]. Oxalate crystals are injurious to renal epithelial cells via the generation of free radicals [15, 16, 17] and inducing apoptosis [18, 19]. Therefore based on the etiology and hyperoxaluria severity, the presentation is different, from kidney stones to renal failure and other tissue depositions (oxalosis).
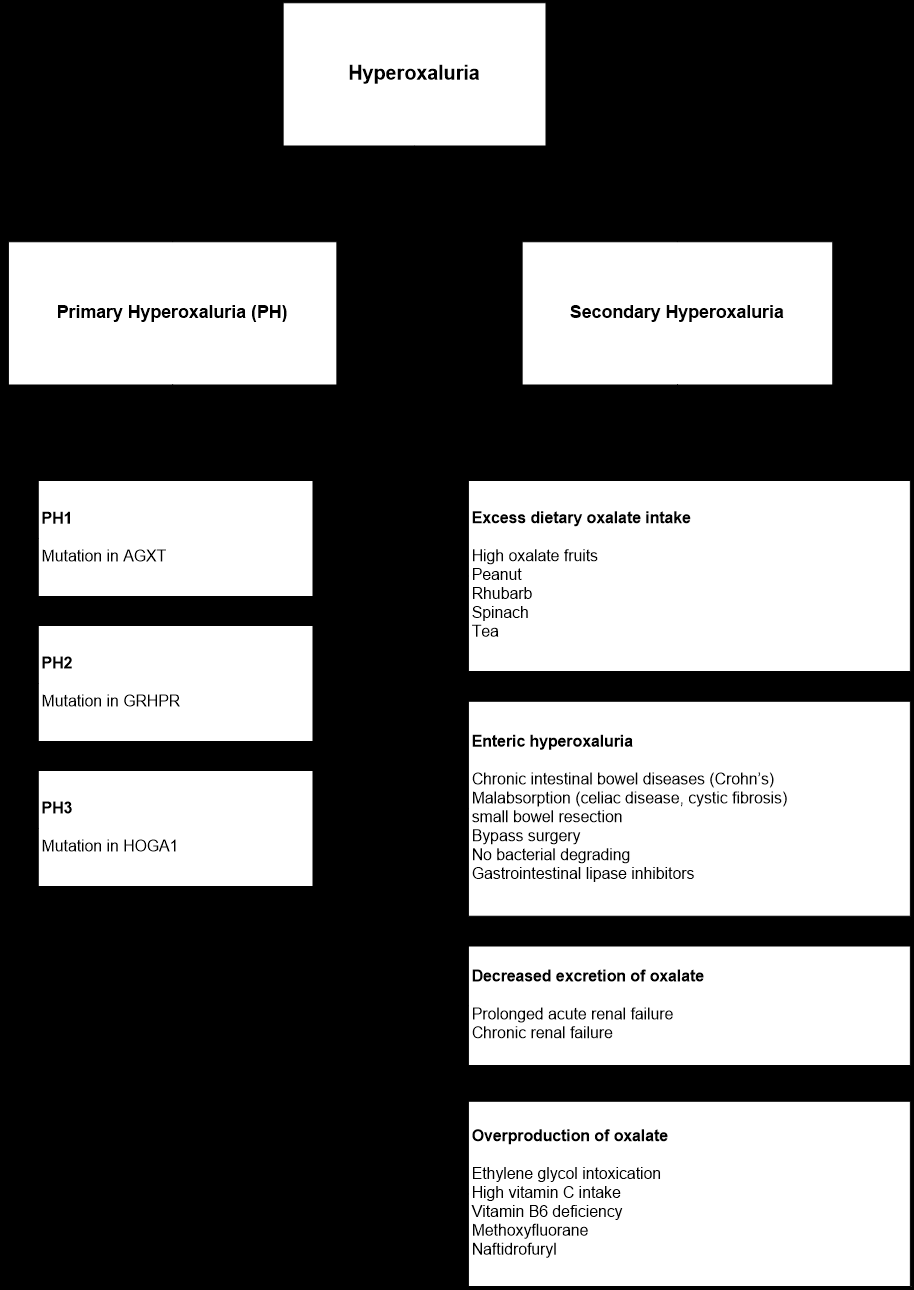
Hyperoxaluria is classified as either primary or secondary. Primary hyperoxaluria (PH) is a rare autosomal recessive inherited disorder of the glyoxylate metabolism in the liver and is classified to PH I-III based on the enzyme defect. It is characterized by renal failure, progressive deposition of diffuse calcium oxalate crystals, and severe recurrent kidney stones. Secondary hyperoxaluria may occur as a result of excess dietary intake, increased endogenous production, or decreased excretion (Figure 2). Secondary hyperoxaluria can occur by one or more of these mechanisms:
Excess Dietary Oxalate Intake
Oxalate is a natural component of fruits and vegetables. Increase in oxalate serum levels and hyperoxaluria can occur upon increased dietary ingestion of foods with high oxalate content [20, 21, 22, 23, 24]. Several reports describe excessive fruit juice ingestion leading to hyperoxaluria and subsequent acute oxalate nephropathy [25, 26, 27, 28]. Also, there are some reports on oxalate nephropathy due to excessive peanut [29] or rhubarb [30, 31] intake.
Enteric Hyperoxaluria
Enteric hyperoxaluria was first described in patients with small bowel resection who subsequently began to develop recurrent calcium oxalate stones in their urinary tract [32]. It has been reported in certain intestinal diseases like chronic inflammatory bowel disease [33, 34, 35, 36], celiac disease [37, 38], Roux-en-Y gastric bypass surgery [39, 40, 41, 42] and orlistat therapy [43, 44, 45, 46] and showed that can lead to end- stage renal disease requiring kidney transplantation [47, 48].
Calcium normally binds to oxalate in the intestinal lumen leading to fecal elimination of calcium oxalate. In malabsorption, excessive intraluminal free fatty acids competitively bind to the intraluminal calcium ions and thereby allow unbound oxalate to be absorbed in colon [49, 50]. In addition, bile salts and free fatty acids are toxic to colonic mucosa and may increase oxalate absorption by increase the permeability of colonic wall [51].
In addition, oxalate is metabolized by Oxalobacter formigenes, gram-negative anaerobic bacteria that colonizes the gastrointestinal tract [52, 53]. O. formigenes is sensitive to a variety of antibiotics [54] and its low count after antibiotic therapy may cause hyperoxaluria by increasing oxalate absorption.
Decreased Excretion of Oxalate
The kidney is the primary organ for oxalate excretion via glomerular filtration and tubular secretion (mediated via SLC26 anion exchangers) [55, 56, 57]. It has been shown that serum oxalate level is elevated about 10 fold in patients with chronic renal failure (uremic oxalosis) due to decrease oxalate clearance [58, 59, 60]. In addition, dialysis patients tend to lose ascorbic acid during dialysis and as a result, should receive vitamin C supplementation [61]. Subsequently, there have been reports of cases of patients on dialysis who developed oxalate crystal deposition in various organs secondary to vitamin C supplementation [62]
Overproduction of Oxalate
Endogenous production of oxalate precursor, glyoxylate, occurs in liver by oxidation of glycolate or by catabolism of hydroxyproline, a component of collagen. This mechanism is associated with hyperoxaluria in ethylene glycol intoxication [63, 64]. Overproduction of oxalate may occur due to high doses of vitamin C, which is a precursor of oxalate, or vitamin B6 (cofactor of AGT enzyme) deficiency [65]. Vitamin C has been shown to have antioxidant effects as a free radical scavenger. Vitamin C has a protective effect against drug- induced nephrotoxicity [66, 67]. However, excessive use and in setting of renal injury, there are several reports on hyperoxaluria and nephropathy due to intravenous high dose of vitamin C [68, 69, 70]. Further reports showed that hyperoxaluria and nephropathy can be associated with high dose oral vitamin C [71, 72, 73], but may even occur in regular doses [74]. In the setting or regular doses of Vitamin C the toxicity of vitamin C can be further compounded with renal insufficiency [14, 75].
Vitamin C is one of the most popular over-the-counter supplements (http://newhope360.com/2012-supplement- business-report). Vitamin C is widely used in various diseases from the common cold to cancers. It is also widely used by alternative medicine practitioners as a treatment for various diseases and conditions [76, 77]. After the first studies showing benefits of vitamin C in cancer patients [4, 5] it is frequently used as a treatment in alternative medicine.
Volume depletion, hypomagnesemia, metabolic acidosis, and reduced urinary citrate excretion are causes of oxalate precipitation. Our patient volume depletion at the time of presentation that together with long-term vitamin C intake cause oxalate nephropathy.
Conclusions
Our case emphasizes the importance of close monitoring of renal function in chronic vitamin C users. Additionally physicians should be aware of vitamin C effects on the kidney and use it with caution in patients with pre-existing renal disease, those who receive nephrotoxic medications, and patients with a history of oxalate nephrolithiasis.
Acknowledgment: None
Consent
The patient reported here is deceased and we have unsuccessfully attempted to contact the next of kin. In order to preserve confidentiality, the report is de-identified and no identifiable information or pictures are being submitted.
Competing Interests
The authors report no competing interests. All authors consents to publication and give permission to publish.
Authors Contributions
MG contributed to care of the patient. AA and WG were specialty consultants. AH and AA did the literature review. All authors participated in drafting, revision and editing of the manuscript.
References
-
Block G (1991) Epidemiologic evidence regarding vitamin C and cancer. The American journal of clinical nutrition 54(6): 1310S-1314S.
-
Frei B (1994) Reactive oxygen species and antioxidant vitamins: Mechanisms of action. The American Journal of Medicine 97(3): S5-S13.
-
Willcox JK, Ash SL, Catignani GL (2004) Antioxidants and prevention of chronic disease. Critical reviews in food science and nutrition 44(4): 275-295.
-
Cameron E, Pauling L (1976) Supplemental ascorbate in the supportive treatment of cancer: Prolongation of survival times in terminal human cancer. Proceedings of the National Academy of Sciences 73(10): 3685-3689.
-
Cameron E, Pauling L (1978) Supplemental ascorbate in the supportive treatment of cancer: Reevaluation of prolongation of survival times in terminal human cancer. Proceedings of the National Academy of Sciences 75(9): 4538-4542.
-
Cameron E, Campbell A (1991) Innovation vs. quality control: An ‘unpublishable’ clinical trial of supplemental ascorbate in incurable cancer. Medical Hypotheses 36(3): 185-189.
-
Creagan ET, Moertel CG, O’Fallon JR, Schutt AJ, O’Connell MJ, et al. (1979) Failure of high-dose vitamin C (ascorbic acid) therapy to benefit patients with advanced cancer. A controlled trial. The New England journal of medicine 301(13): 687-690.
-
Moertel CG, Fleming TR, Creagan ET, Rubin J, O’Connell MJ, et al. (1985) High-dose vitamin C versus placebo in the treatment of patients with advanced cancer who have had no prior chemotherapy. A randomized double- blind comparison. The New England journal of medicine 312(3): 137-141.
-
Hodgkinson A (1977) Oxalic acid in biology and medicine: Academic Press 101: 2.
-
Atkins GL, Dean BM, Griffin WJ, Watts RW (1964) Quantitative aspects of ascorbic ascid metabolisim in man. The Journal of biological chemistry 239: 2975- 2980.
-
Baker EM, Saari JC, Tolbert BM (1966) Ascorbic acid metabolism in man. The American journal of clinical nutrition 19(6): 371-378.
-
Williams HE, Wandzilak TR (1989) Oxalate synthesis, transport and the hyperoxaluric syndromes. The Journal of urology 141(3): 742-749.
-
Robertson WG, Hughes H (1993) Importance of mild hyperoxaluria in the pathogenesis of urolithiasis--new evidence from studies in the Arabian Peninsula. Scanning microscopy 7(1): 391-401.
-
Rathi S, Kern W, Lau K (2007) Vitamin C-induced hyperoxaluria causing reversible tubulointerstitial nephritis and chronic renal failure: a case report. J Med Case Rep 1: 155.
-
Scheid C, Koul H, Hill WA, Luber-Narod J, Kennington L, et al. (1996) Oxalate toxicity in LLC-PK1 cells: role of free radicals. Kidney international 49(2): 413-419.
-
Thamilselvan S, Byer KJ, Hackett RL, Khan SR (2000) Free radical scavengers, catalase and superoxide dismutase provide protection from oxalate-associated injury to LLC-PK1 and MDCK cells. The Journal of urology 164(1): 224-229.
-
Thamilselvan S, Khan SR, Menon M (2003) Oxalate and calcium oxalate mediated free radical toxicity in renal epithelial cells: effect of antioxidants. Urological research 31(1): 3-9.
-
Koul S, Fu S, Koul H (2003) Oxalate exposure promotes reinitiation of the DNA synthesis and apoptosis of HK-2 cells, a line of human renal epithelial cells. Annals of the New York Academy of Sciences 1010: 292-295.
-
Jeong BC, Kwak C, Cho KS, Kim BS, Hong SK, et al. (2005) Apoptosis induced by oxalate in human renal tubular epithelial HK-2 cells. Urological research 33(2): 87-92.
-
Holmes RP, Goodman HO, Assimos DG (2001) Contribution of dietary oxalate to urinary oxalate excretion. Kidney international 59(1): 270-276.
-
Holmes RP, Assimos DG (2004) The impact of dietary oxalate on kidney stone formation. Urological research 32(5): 311-316.
-
Holmes RP, Ambrosius WT, Assimos DG (2005) Dietary oxalate loads and renal oxalate handling. The Journal of urology 174(3): 943-947.
-
Robijn S, Hoppe B, Vervaet BA, D’Haese PC, Verhulst A (2011) Hyperoxaluria: a gut-kidney axis? Kidney international 80(11): 1146-1158.
-
Bsc SN (1999) Oxalate content of foods and its effect on humans. Asia Pacific Journal of Clinical Nutrition 8(1): 64-74.
-
Chen CL, Fang HC, Chou KJ, Wang JS, Chung HM (2001) Acute oxalate nephropathy after ingestion of star fruit. American journal of kidney diseases: the official journal of the National Kidney Foundation 37(2): 418-422.
-
Niticharoenpong K, Chalermsanyakorn P, Panvichian R, Kitiyakara C (2006) Acute deterioration of renal function induced by star fruit ingestion in a patient with chronic kidney disease. Journal of nephrology 19(5): 682-686.
-
Getting JE, Gregoire JR, Phul A, Kasten MJ (2013) Oxalate Nephropathy Due to ‘Juicing’: Case Report and Review. The American Journal of Medicine 126(9): 768-772.
-
Bakul G, Unni VN, Seethaleksmy NV, Mathew A, Rajesh R, et al. (2013) Acute oxalate nephropathy due to ‘Averrhoa bilimbi’ fruit juice ingestion. Indian Journal of Nephrology 23(4): 297-300.
-
Sasaki M, Murakami M, Matsuo K, Matsuo Y, Tanaka S, et al. (2008) Oxalate nephropathy with a granulomatous lesion due to excessive intake of peanuts. Clinical and experimental nephrology 12(4): 305-308.
-
Sanz P, Reig R (1992) Clinical and pathological findings in fatal plant oxalosis. A review. The American journal of forensic medicine and pathology 13(4): 342-345.
-
Albersmeyer M, Hilge R, Schrottle A, Weiss M, Sitter T, et al. (2012) Acute kidney injury after ingestion of rhubarb: secondary oxalate nephropathy in a patient with type 1 diabetes. BMC nephrology 13: 141.
-
Smith LH, Fromm H, Hofmann AF (1972) Acquired hyperoxaluria, nephrolithiasis, and intestinal disease. Description of a syndrome. New England Journal of Medicine 286(26): 1371-1375.
-
Hueppelshaeuser R, von Unruh GE, Habbig S, Beck BB, Buderus S, et al. (2012) Enteric hyperoxaluria, recurrent urolithiasis, and systemic oxalosis in patients with Crohn’s disease. Pediatric nephrology 27(7): 1103-1109.
-
Hylander E, Jarnum S, Frandsen I (1979) Urolithiasis and hyperoxaluria in chronic inflammatory bowel disease. Scandinavian journal of gastroenterology 14(4): 475- 479.
-
Kyle J (1980) Urinary complications of Crohn’s disease. World journal of surgery 4(2): 153-160.
-
Mandell I, Krauss E, Millan JC (1980) Oxalate-induced acute renal failure in Crohn’s disease. Am J Med 69(4): 628-632.
-
Ciacci C, Spagnuolo G, Tortora R, Bucci C, Franzese D, et al. (2008) Urinary Stone Disease in Adults With Celiac Disease: Prevalence, Incidence and Urinary Determinants. Journal of Urology 180(3): 974-979.
-
Gama R, Schweitzer FAW (1999) Renal calculus: A unique presentation of coeliac disease. BJU International 84(4): 528-529.
-
Nelson WK, Houghton SG, Milliner DS, Lieske JC, Sarr MG (2005) Enteric hyperoxaluria, nephrolithiasis, and oxalate nephropathy: potentially serious and unappreciated complications of Roux-en-Y gastric bypass. Surgery for obesity and related diseases: official journal of the American Society for Bariatric Surgery 1(5): 481-485.
-
Nasr SH, D’Amato VD, Said SM, Stokes MB, Largos MV, et al. (2008) Markowitz GS: Oxalate nephropathy complicating Roux-en-Y Gastric Bypass: an under recognized cause of irreversible renal failure. Clin j Am Soc Nephron 3(6): 1676-1683.
-
Lieske JC, Kumar R, Collazo-Clavell ML (2008) Nephrolithiasis after bariatric surgery for obesity. Semin nephrol 28(2): 163-173.
-
Sinha MK, Collazo-Clavell ML, Rule A, Milliner DS, Nelson W, et al. (2007) Hyperoxaluric nephrolithiasis is a complication of Roux-en-Y gastric bypass surgery. Kidney int 72(1): 100-107.
-
Courtney AE, O’Rourke DM, Maxwell AP (2007) Rapidly progressive renal failure associated with successful pharmacotherapy for obesity. Nephrol dial transplant 22(2): 621-623.
-
Singh A, Sarkar SR, Gaber LW, Perazella MA (2007) Acute oxalate nephropathy associated with orlistat, a gastrointestinal lipase inhibitor. Am j kidney dis 49(1): 153-157.
-
Karamadoukis L, Shiva Shankar GH, Lederman L, Williams AJ (2009) An unusual complication of treatment with orlistat. Clin nephrol 71(4): 430-432.
-
Kwan TK, Chadban SJ, McKenzie PR, Saunders JR (2013) Acute oxalate nephropathy secondary to orlistat-induced enteric hyperoxaluria. Nephrology (Carlton) 18(3): 241- 242.
-
Ceulemans LJ, Nijs Y, Nuytens F, De Hertogh G, Claes K, et al. (2013) Combined kidney and intestinal transplantation in patients with enteric hyperoxaluria secondary to short bowel syndrome. Am j transplant 13(7): 1910-1914.
-
Wharton R, D’Agati V, Magun AM, Whitlock R, Kunis CL, et al. (1990) Acute deterioration of renal function associated with enteric hyperoxaluria. Clin nephrol 34(3): 116-121.
-
Chadwick VS, Modha K, Dowling RH (1973) Mechanism for hyperoxaluria in patients with ileal dysfunction. N Engl j med 289(4): 172-176.
-
Binder HJ (1974) Intestinal oxalate absorption. Gastroenterology 67(3): 441-446.
-
Dobbins JW, Binder HJ (1976) Effect of bile salts and fatty acids on the colonic absorption of oxalate. Gastroenterology 70(6): 1096-1100.
-
Allison M, Cook HM, Milne DB, Gallagher S, Clayman RV (1986) Oxalate degradation by gastrointestinal bacteria from humans. J Nutr 116(3): 455-460.
-
Hoppe B, Von Unruh G, Laube N, Hesse A, Sidhu H (2005) Oxalate degrading bacteria: New treatment option for patients with primary and secondary hyperoxaluria? Urol res 33(5): 372-375.
-
Duncan SH, Richardson AJ, Kaul P, Holmes RP, Allison MJ, et al. (2002) Oxalobacter formigenes and its potential role in human health. Appl Environ Microbiol 68(8): 3841-3847.
-
Salyer WR, Keren D (1973) Oxalosis as a complication of chronic renal failure. Kidney int 4(1): 61-66.
-
Williams HE (1978) Oxalic acid and the hyperoxaluric syndromes. Kidney int 13(5): 410-417.
-
Sindic A, Chang MH, Mount DB, Romero MF (2007) Renal physiology of SLC26 anion exchangers. Curr opin nephrol hypertens 16(5): 484-490.
-
Constable AR, Joekes AM, Kasidas GP, O’Regan P, Rose GA (1979) Plasma level and renal clearance of oxalate in normal subjects and in patients with primary hyperoxaluria or chronic renal failure or both. Clin sci (Lond) 56(4): 299-304.
-
Worcester EM, Nakagawa Y, Bushinsky DA, Coe FL (1986) Evidence that serum calcium oxalate supersaturation is a consequence of oxalate retention in patients with chronic renal failure. Jclin invest 77(6): 1888-1896.
-
Petrarulo M, Cerelli E, Marangella M, Cosseddu D, Vitale C, et al. (1994) Assay of plasma oxalate with soluble oxalate oxidase. Clin chem 40(11 Pt 1): 2030-2034.
-
Sullivan JF, Eisenstein AB (1970) Ascorbic acid depletion in patients undergoing chronic hemodialysis. Am j clin nutr 23(10): 1339-1346.
-
Ono K (1986) Secondary hyperoxalemia caused by vitamin C supplementation in regular hemodialysis patients. Clin nephrol 26(5): 239-243.
-
Brent J (2009) Fomepizole for ethylene glycol and methanol poisoning. N Engl j med 360(21): 2216-2223.
-
Eder AF, McGrath CM, Dowdy YG, Tomaszewski JE, Rosenberg FM, et al. (1998) Ethylene glycol poisoning: toxicokinetic and analytical factors affecting laboratory diagnosis. Clin chem 44(1): 168-177.
-
Bobrowski AE, Langman CB (2006) Hyperoxaluria and systemic oxalosis: current therapy and future directions. Expert opin on pharmacother 7(14): 1887-1896.
-
Sadat U, Usman A, Gillard JH, Boyle JR (2013) Does ascorbic acid protect against contrast-induced acute kidney injury in patients undergoing coronary angiography: a systematic review with meta-analysis of randomized, controlled trials. J Am Coll Cardiol 62(23): 2167-2175.
-
Mohamed Abd E, Lasheen NN (2014) Comparative study on the protective role of vitamin C and L-arginine in experimental renal ischemia reperfusion in adult rats. Int J Physiol Pathophysiol Pharmacol 6(3): 153-165.
-
McAllister CJ, Scowden EB, Dewberry FL, Richman A (1984) Renal failure secondary to massive infusion of vitamin C. JAMA 252(13): 1684.
-
Lawton JM, Conway LT, Crosson JT, Smith CL, Abraham PA (1985) Acute oxalate nephropathy after massive ascorbic acid administration. Arch intern med 145(5): 950-951.
-
Alkhunaizi AM, Chan L (1996) Secondary oxalosis: a cause of delayed recovery of renal function in the setting of acute renal failure. J Am Soc Nephrol 7(11): 2320- 2326.
-
Mashour S, Turner JF Jr, Merrell R (2000) Acute renal failure, oxalosis, and vitamin C supplementation: a case report and review of the literature. Chest 118(2): 561- 563.
-
Nasr SH, Kashtanova Y, Levchuk V, Markowitz GS (2006) Secondary oxalosis due to excess vitamin C intake. Kidney int 70(10): 1672.
-
McHugh GJ, Graber ML, Freebairn RC (2008) Fatal vitamin C-associated acute renal failure. Anaesth intensive care 36(4): 585-588.
-
Lamarche J, Nair R, Peguero A, Courville C (2011) Vitamin C-induced oxalate nephropathy. Int j nephrol 2011: 146927.
-
Nankivell BJ, Murali KM (2008) Images in clinical medicine. Renal failure from vitamin C after transplantation. N Engl j med 358(4): e4.
-
Gonzalez MJ, Miranda-Massari JR, Mora EM, Guzman A, Riordan NH, et al. (2005) Orthomolecular oncology review: ascorbic acid and cancer 25 years later. Integr cancer ther 4(1): 32-44.
-
Padayatty SJ, Sun AY, Chen Q, Espey MG, Drisko J, et al. (2010) Vitamin C: intravenous use by complementary and alternative medicine practitioners and adverse effects. PLoS One 5(7): e11414.
- Cancer Diagnosis from RNA Sequence of Blood Cells by Using AI
- Field Cancerization in Oral Cavity, Case Report and Review of Literature. Oncologic Program Salud Integral Hospital, Managua, Nicaragua
- Identification of B Lymphocytes in Cancer Patient’s Blood
- A Case Report of a Breast Cancer Patient Developing Pneumonitis as a Result of Abemaciclib Therapy
- Immune Checkpoint Therapeutics for Today’s Fight and Beyond
- The Amalgamated Sophomore-Gonadoblastoma