An Unusual Cause of Cannon Ball Metastasis-Squamous Cell Carcinoma of Lung
Image Article
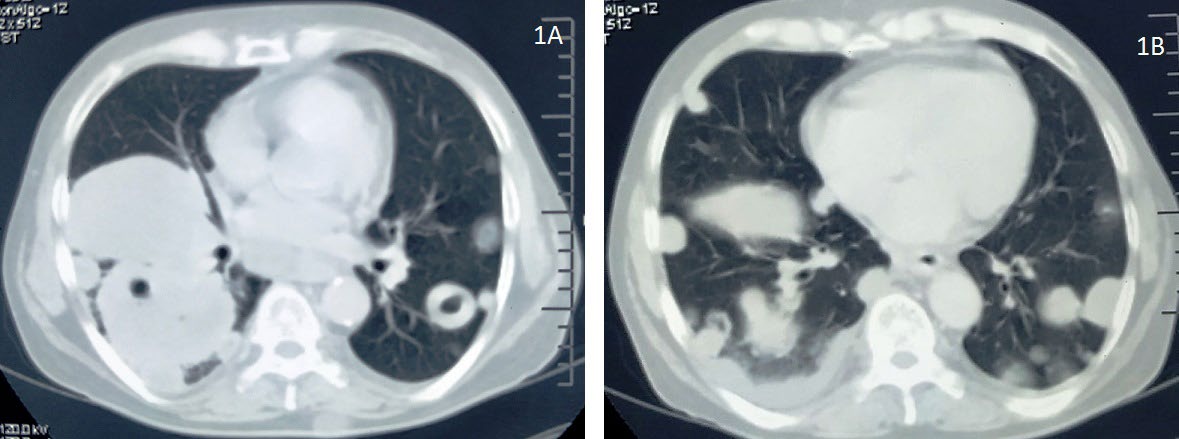
A 68-year-old male patient who is a chronic smoker with smoking index of 450 presented to outpatient department with complains of right sided dull aching chest pain, hemoptysis and shortness of breath for the preceding 3 months. Before visiting to us he was taking anti-tuberculosis drugs for the last 2months on clinic-radiological basis without much symptomatic improvement. His vitals were stable and on general examination there was no pallor, lymphadenopathy, clubbing or pedal edema. Breath sounds were decreased on the right infrascapular and infraaxillary area. Computed Tomography of thorax revealed mass in the Image Article basal segments of the right lower lobe with multiple masses in the bilateral lung fields with some of them showing cavitations, mediastinal lymphadenopathy and mild right pleural effusion consistent with neoplastic etiology (shown in figure 1A and 1B). Ultrasound guided transthoracic biopsy was performed from the right lung mass and nodule in the left lung and histopathology revealed squamous cell carcinoma in both the reports. So, he was diagnosed as advanced stage squamous cell carcinoma of lung with cannon ball metastasis in the opposite lung (stage IV, M1a).
Discussion
Cannon ball metastasis in the lungs are usually caused by renal cell carcinoma, gastrointestinal malignancies or choriocarcinoma [1]. These metastasis usually represent hematogenous spread of the cancer in the organs like lung. Other benign causes for this presentation are tuberculosis, fungal infections and arteriovenous malformations [2, 3]. Some of these lesions can cavitate if the blood supply of the lesion in the centre is compromised due to its rapid growth. Here in this case we report a case of biopsy proven squamous cell carcinoma of the lung with cannon ball metastasis in both the lung fields. To the best of our knowledge till now only few cases were reported in the literature [4].
References
-
Kshatriya R, Patel V, Chaudhari S, Purvesh P, Dhaval P, et al. (2016) Cannon ball appearance on radiology in a middle-aged diabetic female. Lung India 33(5): 562-568.
-
Seaton A (2000) Other pulmonary neoplasm and related conditions. Crofton and Douglas’s Respiratory Diseases. In: Seaton A, Seaton D, Leitch AG, 5th(Eds.), Oxford, Blackwell science ltd.
-
The WHO manual of diagnostic imaging (2006) Radiographic anatomy and interpretation of the chest and the pulmonary system. In: Ostensen H, Petterson H, (Eds.), World Health Organization, Geneva.
-
Sachdeva R, Sachdeva S, Gupta PP (2013) Cannon ball opacities in chest from primary lung cancer: A rare presentation. Clin Cancer Investig J 2(3): 269-270.
- Cancer Diagnosis from RNA Sequence of Blood Cells by Using AI
- Field Cancerization in Oral Cavity, Case Report and Review of Literature. Oncologic Program Salud Integral Hospital, Managua, Nicaragua
- Identification of B Lymphocytes in Cancer Patient’s Blood
- A Case Report of a Breast Cancer Patient Developing Pneumonitis as a Result of Abemaciclib Therapy
- Immune Checkpoint Therapeutics for Today’s Fight and Beyond
- The Amalgamated Sophomore-Gonadoblastoma