Legal Representation of Patients with Dementia in Long Term Care Settings
Introduction: Dementia is a neurodegenerative disease which affects cognitive, physical, and behavioural abilities. To date there is no effective disease-modifying treatment, so the course of disease is progressive [1]. Worsening cognition in advanced stages can impair the person’s mental capacity to make decisions. Consequently, advanced care planning (ACP) is an important aspect in dementia management [2]. Guardianship is an integral part of ACP where the patient legally appoints a trusted person to make best interest decisions for them should they lose capacity. As a result, this study aims to assess the legal representation of patients suffering from dementia. Method: Patients residing in all the nine dementia wards at Saint Vincent De Paul Residence (SVPR), were recruited (203 patients). A diagnosis of dementia is a requirement for admission to these wards. A data collection sheet was designed and included data on the patient’s demographics, MMSE scores and guardianship statuses. Data was collected retrospectively from the patient’s medical records and their caring medical team where documentation was lacking. The data collection period included September to October 2022. Results: Only 7 patients had a guardianship present (3%). The patients’ children (57.1%) were more likely to apply for guardianship, followed by the patients’ spouses (28.6%). The guardianship status was clearly documented in the doctors’ notes and next of kin (NOK) paper, together with the name and contact details of the guardians. 196 patients (97%) did not have guardianship. 5 of these had a power of attorney (POA) but the type was not specified. 190 patients had a relative or friend listed as the next of kin (NOK) and a patient had no legal guardian or NOK. Conclusion: Most patients with Dementia did not have formal legal representation like guardianship or valid POAs. However, the majority of NOK documented were in line with the legal definition of the responsible carer according to the MHA
Introduction
Dementia is an important condition associated with old age. It affects around 50 million people globally and the number is expected to increase by 24% from the year 2018 to the year 2050 [1]. This is a neurodegenerative disease which affects cognitive, physical, and behavioural abilities. It can be caused by various aetiologies which may affect different cognitive domains leading to different signs and symptoms. However, to date there is no effective disease- modifying treatment for dementia, so the course of disease is progressive in nature irrespective of the underlying pathophysiology [2]. Worsening cognition in advanced stages of dementia is most likely to impair the person’s mental capacity to make important decisions.
Mental capacity refers to a person’s ability to make a decision [3]. Every human being has a right to autonomy [4] while society has the responsibility to safeguard vulnerable people against harm and abuse [5]. The challenge arises when trying to achieve a balance between autonomy and beneficence. A tool to aid in achieving such a balance is advanced care planning (ACP) which is the hallmark of dementia management [6]. ACP enables individuals with dementia to make informed future decisions about their health and financials while they still possess the mental capacity to do so. This process can also allow them to choose a designated person of trust to make decisions on their behalf in the future should they lose capacity [7]. ACP is also a dynamic and continuous process which evolves according to the patient’s changing needs and wishes. In fact, it should involve multiple members of the multidisciplinary team (MDT), but most importantly the patient and their family and friends. Moreover, a diagnosis of dementia can be very distressing for the patient, so an ACP has the potential of empowering the patients leading to greater peace of mind [8]. In fact, a Cochrane review carried out by Walsh SC, et al. [9], concluded that palliative care at end of life and ACP in dementia management has the potential to improve the patient’s quality of life and improve concordance of care [9]. However, results were of poor quality and there were very few studies which included patients with advanced dementia in view of ethical considerations.
Consequently, ACP should be done in the early stages of disease while the patient still retains mental capacity. However, these are quite difficult discussions to have, especially when tackling end of life care. In fact, it might cause more anxiety if done at the time of diagnosis which is already distressing in itself. As a result, certain patients might be reluctant to have such conversations [8]. Moreover, reluctance of these discussions are also effected by cultural aspects. For instance, Tetrault A, et al. [8] conducted a qualitative study on the views of Finish patients suffering from Dementia on ACP. This concluded that some patients liked the idea to plan ahead but others preferred living day by day. However, this study also went into the patient’s knowledge of the dementia diagnosis and revealed that most patients and their care givers didn’t acknowledge that disease progression was inevitable [8]. This can be due to either lack of knowledge on the disease or denial. Either way, this highlights the importance of proper education of the disease to newly diagnosed patients and their caregivers, as well as continued follow up on both medical and psychosocial needs. In fact, lack of education can be a potential barrier to ACP since the patient might not acknowledge its importance. In fact, another pilot study carried out by Bosisio F, et al. [10] on dementia patients in Switzerland, had similar findings. It concluded that patients and relatives who were given an opportunity to carry out an ACP were satisfied with the process. However, it also identified some challenges which might impede the ACP process including misconceptions about dementia and ACP, to identify eligible patients, as well as structural and institutional challenges [10].
Another challenge is the communication with patients with Dementia. As outlined above, Dementia affects various cognitive abilities including language and the ability to make abstract decisions about things that may happen in the future. As a result, the healthcare professional (HCP) has to possess a certain skill when communicating with patients suffering from cognitive problems. However, not all HCP may be comfortable in doing that and are more likely to discuss ACP with the patient’s caregiver rather than with the patients themselves [11]. On the other hand, in the more advanced stages, the patient will ultimately lose the ability to communicate and make decisions for themselves, so it is important to address the choice of a legal proxy in earlier stages of disease. However, ACP, including the appointment of a legal proxy, is highly influenced by the country’s legislations [7].
Scope and Aims
The increasing ageing population and the increasing prevalence in Dementia, is leading to a higher socioeconomic burden worldwide. Various countries have been adopting dementia management strategies to try and alleviate this burden. Malta is not immune to this phenomenon. ACP is a potential tool that can be used for this scope. In fact, a systematic review carried out by Sakamoto A, et al. [12], concluded that ACP reduced visits to the emergency department in nursing home residents, including those suffering from Dementia [12]. However, ACP is a fairly new concept in Malta. In fact, pilot projects on ACP are being carried out by the Geriatric Society in Malta in an attempt to introduce this concept in clinical practice.
However, there are no specific legislations on ACP in Malta. This often leads to reluctance among HCP to carry out an ACP in fear of medicolegal implications including its validity. However, there is a section dedicated to mental capacity and best interest decisions in the Maltese Mental Health Act (MMHA) [13]. There are also legislations regarding legal proxies for people who cannot manage their own affairs or lack capacity to do so. This is an essential component of an ACP. As a result, HCP should be familiar with local legislations. This knowledge will facilitate any decision making if the patient is unable to make their own decision, especially if there is disagreement between family members or there are no caregivers available. Table 1 outlines the type of legal representations available in Malta. This study aims at exploring the legal representation of patients suffering from dementia in Malta and whether this is in line with local legislation [14].
| Legislation | Description |
|---|---|
| Power of Attorney (POA) [15] | · Covered by Articles 1856-1890 of the Maltese Civil Law and is referred to as a mandate. |
| · It is defined as a “contract whereby a person gives to another the power to do something for him”. | |
| · In order for someone to do a POA, they need to be above 18 years of age and have mental capacity to do so. | |
| Types of POA | |
| Article 1863 and Article 1886 b: POAs for administrative tasks only which are terminated as soon as the patient is incapacitated. | |
| · General POA: This enables the mandatory to act on behalf of the mandator for any type of action. | |
| · Special POA: This enables the mandatory to act on behalf of the mandator for a specific action only. | |
| Article 1864A: POA/Mandate made in anticipation of mental incapacity and can include both administrative and care needs. However, the mandate has to be above 18 years, at least two witnesses must be present, and a medical declaration is needed. This is similar to an Enduring POA but it becomes valid once the mandate losses mental capacity. It can be revoked at any time. | |
| Guardianship [16,17] | · The Guardianship Act is separate from the Mental Health Act. |
| · The guardianship process values greatly the patient’s opinion. | |
| · The process can be initiated if the patient has already lost mental capacity. | |
| · Applications are processed by a Guardianship board as opposed to court. | |
| · Application process: Guardianship application form accessible online. There are two applications, one to be filled in by the applicant and the other one is a medical report to be filled in by a doctor. Once the application and the necessary documents are received by the guardianship board, the board meets with the people involved including the person subject to guardianship, the people applying to become guardians and any other relevant individuals. The board can also appoint any experts to assist them in the decision making process. If the guardianship is granted, a Guardianship Order is issued, and the Board must notify the Court of Voluntary Jurisdiction. | |
| · One or more people can apply for guardianship. | |
| · The Guardianship act also defines the responsibilities of the guardian. | |
| · A guardian is not expected to receive any rewards for his/her role. In fact, the board can revoke any guardianship statuses if they deem that the guardian is not fulfilling their responsibilities. | |
| · The guardian is then obliged by law to submit an income and expenditure account confirmed by oath of any assets pertaining to the guardianship. This account is to be submitted on a yearly basis to the Guardianship Board or on termination or revocation of guardianship. | |
| Incapacitation and/or Interdiction [18] | · Incapacitation or interdiction are used if the mental incapacity is expected to last longer than 26 weeks or be permanent, and/or guardianship is not possible or not granted. |
| · Approved by the courts of law. The application can be submitted directly to the Court of Voluntary Jurisdiction. | |
| · The person’s spouse, relatives or State Attorney can make the demand. | |
| · The court has the obligation to question the person for whom interdiction/ incapacitation has been requested and appoint three independent specialist reviews for examination. | |
| · Appointment of a Curator: Until a decision is made, a temporary curator may be appointed by the court. The term of the curator is 3 years but may be re-appointed after this period. The curator will take care of the property of the person incapacitated/interdicted. The curator needs to present a yearly report to the court outlining how he/she fulfilled his/her responsibilities. | |
| · Incapacitation and interdiction are more restrictive on the rights of the person when compared to guardianship and may also lead to invalidation of any decisions made by the person being incapacitated/interdicted before this process occurred if the court deems that the cause for incapacitation or interdiction was present at the time of decision making. | |
| · There is also an online register of interdicted/incapacitated persons. | |
| · This process can be reversed if the cause for application ceases to exist. | |
| The Responsible Carer [13] | · The above legal proceedings take time, but sometimes urgent decisions need to be made. |
| · In that case, Part VII of the MHA concerns special treatment, restrictive care and research. It describes that if a person lacks capacity to give consent, this should be obtained by the responsible carer. | |
| · Description: A person that is ordinarily resident in Malta, maintains a close personal relationship with the patient, manifests concern for his welfare; or a person appointed in writing by the patient while they had mental capacity to act on his behalf. | |
| If the patient lacks capacity and there is no appointed carer in writing, the following should be considered as the responsible carer in order of preference: | |
| (1) Husband or wife, | |
| (2) Sons and daughters over the age of 18 years, | |
| (3) Either parent by mutual consent, | |
| (4) Close friends or other relatives of patient. | |
| · If the latter are absent or refuse to give consent, a health care professional is appointed by the Commissioner to act as a responsible carer with regards to healthcare needs only . | |
| · Paragraph c of Part VII of the MHA, stipulates that the person providing care can act in the best interest of the person who lacks capacity in emergency situations where the patient’s life is at risk. |
Table 1: Legislations on Legal Proxies in Malta.
Method
Study Setting
Saint Vincent De Paul Residence (SVPR) is a long term care facility for frail and highly dependent older adults, including those suffering from moderate to severe dementia. It has a capacity of 1500 residents with 24-hour medical care available at the facility itself. There are also nine specialised closed dementia wards to tailor for the wide spectrum of disease presentation. A diagnosis of dementia is a requirement for admission to these wards. Documentation of all the patients residing in the closed dementia wards at SVPR was analysed.
Study Design
This is a retrospective quantitative observational study. Approval to carry out this study and permission to collect data from patients’ files was obtained from the Medical Director at SVPR via e-mail. The data protection act was followed in regards of data collection and storage.
Case Definitions
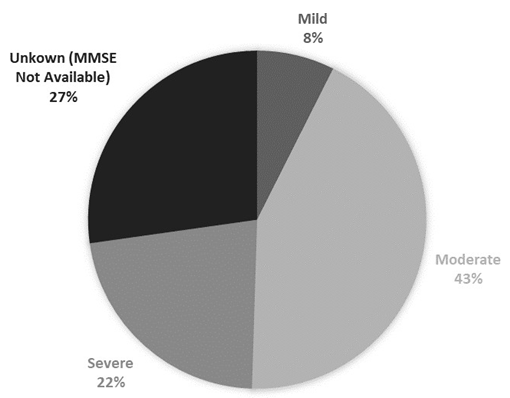
The DSM-V criteria were used for Dementia diagnosis [11]. Dementia severity was defined by the Mini Mental State Examination (MMSE) scores. An MMSE score of 21 -24 was used to define mild dementia, an MMSE score of 10-20 was used to define moderate dementia and an MMSE score of 9 or less was used to define severe dementia.
Data Collection and Analysis
A data collection sheet was designed as shown in Appendix A. Data was collected from the patient’s medical records. Medical records were analysed from the patient’s physical medical notes stored in the wards. Where documentation was lacking, data was collected from the patients’ caring medical team. The data collection period included September to October 2022. Each ward was visited once during the data collection period. Data was then organised in an Excell sheet from which results were drawn.
Results
Patient Demographics
The medical records of 203 patients were analysed. The average age was 80.3 years, ranging from 59 years to 99 years. 95 were males (46.8%) and 108 were females (53.2%). Figure 1 illustrates the percentage of dementia severity, with moderate severity being the most common. An MMSE was not available in 27% of patients, so their dementia severity could not be ascertained. The average MMSE score for the total population was 12 out of 30.
Guardianship Status
Only 7 (3.4%) patients had a guardianship present. The average MMSE did not differ significantly from the total population and from those patients without a guardianship as shown in Table 2. The average MMSE score of 13 indicates that dementia of moderate severity was the most common amongst patients who had guardianship. However, the average MMSE score was based on the latest MMSEs since only 3 out of 7 patients had the MMSE score documented at the time of guardianship application. In all these 3 cases, total scores remained stable over an average time span of 2 years.
The patients’ children (57.1%) were more likely to apply for guardianship, followed by the patients’ spouses (28.6%). The relationship of the remaining two guardians included a sibling and a niece.
| Guardianship status | Average MMSE score |
|---|---|
| Total population | 12 |
| Guardianship present | 13 |
| Guardianship not present | 12 |
Table 2: Average MMSE scores.
The Responsible Carer
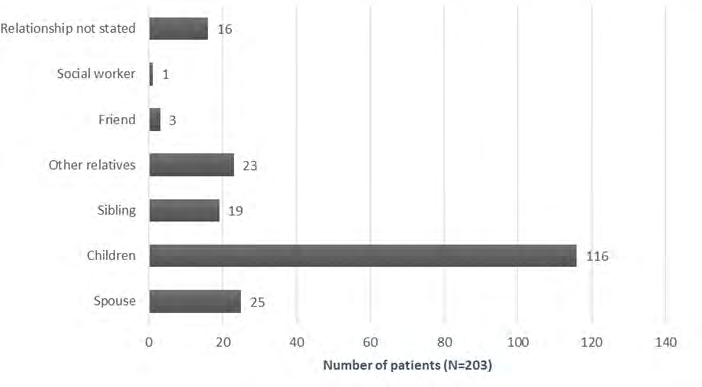
196 patients (97%) did not have guardianship. 5 of these patients had a power of attorney present, 190 patients had a relative or friend listed as the next of kin (NOK) and 1 patient had no legal guardian or NOK. The type of power of attorney was not documented. Figure 2 describes the relationship of the responsible carers. The children are the most common NOK, followed by spouses, siblings and other family members.
Documentation
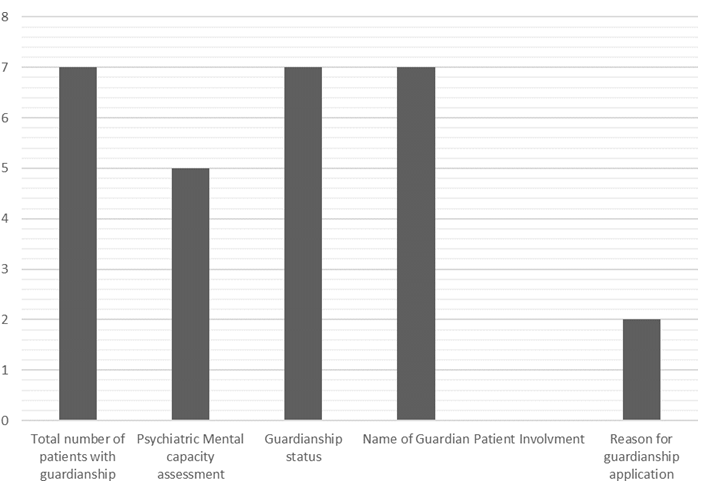
Guardianship application is a process that involves the MDT. Figure 3 shows information about the documentation of this process in our cohort of patients. In all the seven cases, the guardianship status was clearly documented in the doctors’ notes and Relatives’ contact form, together with the name and contact details of the guardians. In all cases, only one guardian was present. In 5 of these cases, a formal mental capacity assessment was performed by a psychiatrist.
Patient involvement was not documented in any of these cases, so it is difficult to ascertain whether they were involved in the decision making process. Moreover, the events that prompted guardianship application, were only documented in two cases, both being progression in cognitive decline. In those patients who had no guardianship, the name and relationship of the NOK, were clearly documented in the Relatives’ contact form.
Discussion
These results illustrate the unpopularity of formal legal representation (guardianship or POA) amongst patients suffering from dementia. Moreover, the average MMSE of 13/30 indicated that the majority of patients already had moderate stages of Dementia. The more advanced the Dementia, the greater the chance that capacity could be impaired. This highlights the importance of ACP and early intervention.
The Use of MMSE in Capacity Assessment
The MMSE is a widely used tool to quantify dementia severity [19]. There are various studies exploring the predictive value of the MMSE in determining mental capacity. On the other hand, we also know that mental capacity is decision specific, therefore the predictive accuracy may differ according to the specific decision it is used for [3, 13, 14]. For instance, a study conducted by Gregory R, et al. [19], explored The use of the MMSE in capacity assessment to create an enduring power of attorney (EPA) in 74 participants. It concluded that there was a statistically significant association between the degree of cognitive impairment quantified by the MMSE and capacity. In fact, an MMSE cut off score of 18 had a sensitivity of 86.6%, a specificity of 82.2%, positive predictive value (PPV) of 75.8% and a negative predictive value (PNV) of 90.2% [19]. On the other hand, Ripley S, et al. [20], explored the use of the MMSE in predicting capacity to decide regarding relocation from home to long term care in 38 participants. It concluded that a cut off score of 17 yielded a PPV of 93% and a NPV of 83%, with a misclassification rate of 13% [20]. Another study conducted by Whealan PJP, et al. [21], assessed the predictive accuracy of the MMSE for capacity to consent for research participation. It concluded that a cutoff score of 13/14, had a PPV of 0.84 and an NPV of 0.69. However, it also mislabelled 24% of capable subjects as lacking capacity, and 21% of incapable subjects as having capacity [21].
All the results in these studies identified MMSE cutoff score above the average MMSE scores of our patient population, indicating that capacity to make certain decisions was most likely impaired in most of them. This highlights the importance of ACP including the discussion or appointment of a legal proxy in the early stages of dementia when capacity is more likely to be reserved. In fact, another interesting factor from the results is the lack of patient involvement when making such decisions. For instance, in the 7 cases where guardianship was done, patient involvement was not documented in either case. This could be merely an oversight during the documentation process, but it could also be that the patients were not consulted. This is especially so if the patient had moderate to severe dementia and his/her communication abilities were impaired [22]. On the other hand, just because a patient has cognitive impairment or lack of capacity, doesn’t imply that his/her views should be ignored completely. Then one should utilise the MDT and the patient’s family/ friends to reach a best interest decision based on all the information available [3].
Moreover, certification of lack of capacity is a very serious matter which might affect the patient’s quality of life and autonomy. As a result, one should ensure that it is done thoroughly. As a result, any test that has suboptimal accuracy in predicting mental capacity should be used with caution. This includes the MMSE, where above studies indicated that there were cases of misclassification when predicting capacity to various decisions. In fact, the UK Mental Capacity Act 2005, describes what a mental capacity should consist of, including the components of mental capacity. It describes two separate components [23]. Diagnostic Component: For mental incapacity to be present, this must be a result of an impairment or disturbance in the functioning of the mind or brain. Functional Components: If any of the below components are absent, a patient is said to lack mental capacity.
- Understand the information relevant to the decision: The relevant information needs to be given in a way that the patient is able to understand it.
- Retain that information long enough for the patient to be able to make the relevant decision at the material time.
- Use or weigh that information to make a decision, including the consequences of the decision.
- Communicate his decision by any means including verbal and non-verbal communication.
In fact, the MMSE would only cover the first component by diagnosing the presence of cognitive impairment. On the other hand, it would not address the functional component which can only be assessed by a formal mental capacity assessment. Despite this, only 5 patients in this study had a formal mental capacity assessment done.
Timing of Mental Capacity Assessment
Both the UK MCA 2005 and the Maltese MHA 2012, state that lack of mental capacity should not be assumed based on the patient’s condition and it should be questioned only when indicated [13, 23]. As a result, one could argue that unless there is a specific reason or new event that requires a best interest decision, a mental capacity assessment should not be done. However, appointing a legal proxy, takes time to arrange. Prolongation of decision making in view of legal conflict may be detrimental to the patients with dementia, especially with regards to health issues. This process can be further complicated or delayed by conflict between family members. As a result, this should be prompted in the initial stages of patient contact, rather than in crisis situations when a decision is needed. Moreover, potential future ethical decisions can be predicted in Dementia, including decisions on tube feeding, procedure consents or other end of life decisions. This highlights the importance of introducing ACP during which the patient’s wishes are documented, thereby facilitating the process.
The POA is a form of ACP since one of the requirements for a POA is the presence of mental capacity [12]. However, only 5 patients in this study had a POA. Moreover, for those patients who had a POA, the type of POA was not documented. This is especially important since certain types of POA might not be valid if there is lack of mental capacity as described in Table 1 [12]. As outlined in Table 1, those POAs which get invalidated by incapacitation, concern administrative tasks only. These often include management of finances, property or other affairs, so third parties involved in any transactions might not be aware of the patient’s Dementia diagnosis and possible lack of capacity. As a result, the validity of the POA is rarely questioned. The following ethical dilemmas arise here:
- If the POA is not questioned by third parties but the HCP suspects incapacity, should one perform a formal capacity assessment to actively invalidate the POA if incapacity is confirmed? And then apply for guardianship/Incapacitation/Interdiction to appoint a legal guardian? OR
- Only request a formal capacity assessment for invalidation of a POA if the patient’s capacity is questioned by the administrators or one is suspecting financial abuse from the caregiver? Otherwise, the POA would remain valid in the absence of formal incapacitation.
Various factors come into play here. For instance, a POA only covers financial and administrative tasks, so the problem of a legal proxy with regards to healthcare decisions is still lacking here. The other options would be incapacitation or guardianship. On the other hand, some patients and caregivers who do not have medical knowledge, might want to leave care decisions in the medical team’s hand whom they trust. Tetrault A, et al. [8] conducted a qualitative study on the views of Dementia patients regarding ACP. In the majority of cases, the management of finances prompted them to do a POA or any form of ACP [8]. In fact, when offering guardianship to someone with a POA in clinical practice locally, most do not feel the need for it since their major issues would be the managing of finances and leave the medical decisions in the medical team’s hands. In fact, only 3.4% of this study population had a formal guardianship application done. Additionally, Tetrault A, et al. [8] study, showed that some participants expressed a wish not to burden their relatives and friends with decisions regarding healthcare issues and reported that they trusted the HCP to care for them [8]. On the other hand, there were participants who were fearful and doubtful about the care they would receive in a nursing home based on their experience with other family and friends. Despite this, most patients were open to such discussions and caregivers were also thankful for initiating them [8]. This illustrates the importance of discussion with patients and relatives.
Legislation on Mental Capacity in Malta
Most medical training in Malta involves UK based exams. This may be adequate with regards to medical management but less so with managing ethical issued associated with medicolegal implications. In fact, Maltese and UK laws associated with mental capacity differ greatly (Refer to the supplementary material for more detail regarding the differences) [8, 14]. This will inevitably impact decision making.
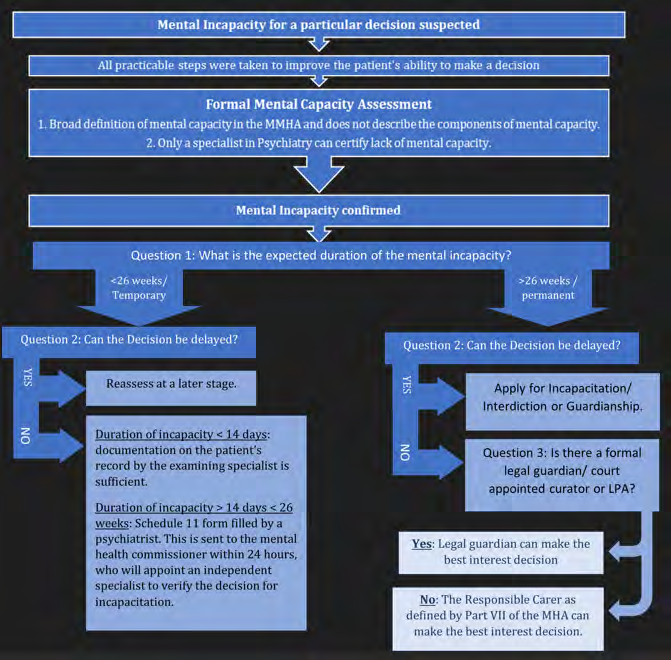
In Malta, Part V of the Mental Health Act 2012 concerns laws regarding mental capacity. The MHA defines mental capacity as follows: “the patient’s ability and competence to make different categories and types of decisions and to be considered responsible for his actions” [13]. It also states that mental capacity in patients suffering from mental disorders should be assumed unless proven otherwise. Moreover, it specifies that only a specialist in Psychiatry can perform a mental capacity assessment [13]. The MHA also refers to the duration of the mental incapacity where it gives instructions on how to proceed if the incapacitation is transient or long standing. Figure 4 illustrates the steps one can follow with regards to decision making in lack of capacity according to local legislation [13, 14].
Moreover, mental capacity is decision specific [3]. In fact, the specialist needs to state the reason for mental incapacity, the category or type of decision that the patient is unable to make and the estimated duration of lack of capacity. This implies that the patient might have capacity to decide regarding his financial assets but not on decisions pertaining to health. Consequently, the MMHA 2012 also describes the use of the Schedule 12 form which is used to revoke a mental incapacity decision in those patients who regain their mental capacity during any periods outlined above [13].
However, dementia is a neurodegenerative condition with progressive cognitive deterioration. As a result, if the lack of mental capacity is secondary to the disease process, it will unlikely be reversed. The concept of best interest decision should apply in such cases where another person is legally appointed to make decisions on behalf of the patient with mental incapacity [3]. There are several options on how to do this legally, namely appoint a responsible carer via a guardianship application or a court appointed curator via the processes of interdiction or incapacitation as described in Table 1.
Guardianship has the potential to be a good solution to reduce medicolegal issues associated with decision making in patients without mental capacity. The advantage of Guardianship over POA is that Guardianship can be done even if the patient lacks capacity; a doctor can apply for it as opposed to a POA which is taken care of by lawyers or notaries; and there is a designated board which monitors the action of the guardian. If POA is absent and there is established lack of capacity, there is also the option of incapacitation or interdiction. However, the process of incapacitation and interdiction has to go through the court proceedings which may prove to be lengthy and expensive for the patient’s carers. Moreover, the latter are more restrictive in the rights of the patients since they generalise mental incapacity. On the other hand, we know that mental incapacity is often decision specific. In fact, guardianship gives one the opportunity to highlight which area of capacity is lacking and to what degree. For instance, capacity in the medical report of the guardianship application is divided into three categories: decisions pertaining to (1) personal health care, (2) lifestyle/accommodation choices and (3) financial and legal affairs. These are further subdivided into simple and complex decisions [17].
However, there are inconsistencies between the MMHA and the Maltese Guardianship Act which might lead to confusion amongst the caring team on how to approach decision making. For instance, as opposed to the MMHA, the guardianship act does not specify who are the specialists who can fill the medical report [16, 17]. The dilemma arises since the guardianship application requires a mental capacity assessment which according to the MMHA can only be done by psychiatrists. This often causes confusion or reservations amongst doctors other than psychiatrists on whether or not they can fill out such forms. On the other hand, it is the guardianship board’s responsibility to process the applications and they have a right to appoint any experts when in doubt [16]. Moreover, a formal mental capacity assessment by a psychiatrist can be requested before applying for guardianship and this could be included in the medical report. In fact, 71.4% of the patients who had a guardianship application in this study, had a formal mental capacity assessment by a psychiatrist. On the other hand, it might not be practical to request a psychiatry assessment for every patient with dementia, especially when it would be quite evident that a patient lacks capacity. In fact, the patient’s caring physician might be more than capable to ascertain whether a patient has mental capacity to make a specific decision, especially in the later stages of diseases. In fact, in the UK, any HCW can do an MCA since the components needed for mental capacity are stated clearly in the Mental Capacity Act 2005 [3, 23].
Study Limitations
Data from this study was collected from the medical notes. As a result, the quality of documentation might have affected the results. Moreover, medical records are in paper form and can also get lost. For instance, 27% of patients did not have an MMSE documented. There are various possible reasons including the possibility that this was not done by the caring firm, the MMSE form was misplaced, or the patient had severe dementia with impaired communication abilities. Moreover, patients might have had a guardianship or POA in place but if this was not documented in the medical notes and/or a copy of the legal document was not present, it would have been difficult to confirm the presence or absence of it. For instance, documentation about patient involvement in guardianship applications and the reason for application where not documented in any or most cases where guardianship was in place. This may indicate that documentation could have been improved [29].
In fact, we also tried to gather information from the patients’ medical firm where we felt information was missing. However, the lack of documentation predisposes them to recall bias, especially due to the large amount of patients under a firm’s care. On the other hand, it is important that legal representation is properly documented, especially during on call hours when patients are reviewed by other doctors or during emergency situations when the information needs to be easily accessible [30].
Moreover, information on guardianship status was gathered from patients in only one long term care facility in Malta, therefore practices might not be representative of all residential care homes.
Conclusion
Only a small proportion of patients in this study had formal legal representation, despite the fact that their dementia severity was already in the moderate stages when lack of capacity could be an issue. This confirms the unpopularity of ACP in patients with Dementia in Malta. In fact, there are no laws regarding advanced directives. It would also be interesting to perform studies aimed at identifying the obstacles encountered by physicians when discussing ACP and managing ethical issues in Dementia. These might help shed a light on any problems that are present and try to find ways to improve the process for everyone involved.
As highlighted in the discussion, lack of knowledge might be a problem in this area. The formulation of local guidelines on decision making in dementia based on local legislations would help the health care workers in decision making. In addition, more education on medicolegal issues in dementia for health care professionals is required. In fact, this should be included in the medical school or speciality training curricula, focusing on local legislature rather than foreign based ones. The availability of legal advice for the caring team is also important, especially in facilities housing residents with advanced Dementia. Moreover, the proper documentation of the dementia diagnosis, mental capacity and the details, of the responsible carer is very important. This should be made accessible to anyone caring for the patients with dementia, ideally via an electronic platform while respecting the patient’s privacy and data protection laws.
In conclusion, this study highlights that despite the evidence on the importance of ACP in patients with Dementia, this is not a popular concept everywhere. Moreover, HCW should be properly trained in communicating with patients with cognitive and sensory impairments. Medical schools and training programmes should acknowledge the importance of training their HCW on management of ethical issues in Dementia, including performing an ACP as well as provide their trainees with the necessary legal knowledge to be as safe as possible for both their patients and themselves.
Conflicts of Interest: Nil
Funding: Nil
References
-
World Health Organisation (WHO) (2020) Dementia
-
Regier NG, Hodgson NA, Gitlin LN (2017) ‘Characteristics of Activities for Persons with Dementia at the Mild, Moderate, and Severe Stages’. Gerontologist 57(5): 987- 997.
-
British Geriatric Society (2010) ‘Fact Sheet: Mental capacity: an ethical conundrum’.
-
(1998) Human Rights Act (1998). Legislation.gov.uk.
-
(2015) Mental Capacity Assessment Tool Guidance. Social Care Institute for Excellence.
-
National Institute for Health and Care Excellence (NICE) (2018) NG97: Dementia: assessment, management and support for people living with dementia and their carers.
-
Piers R, Albers G, Gilissen J, De Lepeleire J, Steyaert J, et al. (2018) Advance care planning in dementia: recommendations for healthcare professionals. BMC Palliat Care 17(1): 88.
-
Tetrault A, Nyback MH, Vaartio-Rajalin H, Fagerström L (2022) Advance care planning in dementia care: Wants, beliefs, and insight. Nurs Ethics 29(3): 696-708.
-
Walsh SC, Murphy E, Devane D, Sampson EL, Connolly S (2021) Palliative care interventions in advanced dementia. Cochrane Database Syst Rev 9(9): CD011513.
-
Bosisio F, Sterie AC, Rubli Truchard E, Jox RJ (2021) Implementing advance care planning in early dementia care: results and insights from a pilot interventional trial. BMC Geriatr 21(1): 573.
-
Visser M, Smaling HJA, Parker D, van der Steen JT (2022) How Do We Talk with People Living with Dementia about Future Care: A Scoping Review. Front Psychol 13: 849100.
-
Sakamoto A, Inokuchi R, Iwagami M, Sun Y, Tamiya N (2023) Association between advanced care planning and emergency department visits: A systematic review. Am J Emerg Med 68: 84-91.
-
Mental Health Act (2012) Ministry for health and active ageing. Health.
-
Zahra A, Camilleri M, Cachia J (2014) ‘A new Mental Health Act for Malta’. International Psychiatry 11(3): 67.
-
LEĠIŻLAZZJONI MALTA (2023) Civil Code CHAPTER 16. pp: 401-409.
-
GEORGE A (2012) President Act XXIV. LEĠIŻLAZZJONI MALTA, pp: 728-277.
-
(2023) Application Process. Guardianship.gov.mt.
-
(1855) Code of Organisation and Civil Procedure Article. Legislation.mt.
-
Gregory R, Roked F, Jones L, Patel A (2007) Is the degree of cognitive impairment in patients with Alzheimer’s disease related to their capacity to appoint an enduring power of attorney. Age Ageing 36(5): 527-531.
-
Ripley S, Jones S, Macdonald A (2008) Capacity assessments on medical in-patients referred to social workers for care home placement. Psychiatric Bulletin 32(2): 56-59.
-
Whelan PJ, Oleszek J, Macdonald A, Gaughran F (2009) The utility of the Mini-Mental State Examination in guiding assessment of capacity to consent to research. Int Psychogeriatr 21(2): 338-344.
-
Aworinde J, Ellis-Smith C, Gillam J, Roche M, Coombes L, et al. (2022) How do person-centered outcome measures enable shared decision-making for people with dementia and family carers?-A systematic review. Alzheimers Dement (NY) 8(1): e12304.
-
(2005) Mental Capacity Act 2005. Legislation.gov.uk.
-
Sun W, Matsuoka T, Narumoto J (2021) Decision- Making Support for People With Alzheimer’s Disease: A Narrative Review. Front Psychol 12: 750803.
-
Kelley R, Godfrey M, Young J (2021) Knowledge Exchanges and Decision-Making within Hospital Dementia Care Triads: An Ethnographic Study. Gerontologist 61(6): 954-964.
-
Murphy J, Oliver T (2013) The use of talking Mats to support people with dementia and their carers to make decisions together. Health Soc. Care Commun 21(2): 171-180.
-
Waller A, Bryant J, Bowman A, Willmott L, Pickles R, et al. (2022) Junior medical doctors’ decision making when using advance care directives to guide treatment for people with dementia: a cross-sectional vignette study. BMC Med Ethics 23: 73.
-
Mitropoulos J, Austin N, Hunter P, Cairney H, Parikh S (2019) Decision-making for older patients by Australian and New Zealand doctors with Advance Care Directives: a vignette-based study. Intern Med J 49(9): 1146-1153.
-
Hugo J, Ganguli M (2014) ‘Dementia and cognitive impairment: epidemiology, diagnosis, and treatment’. Clin Geriatr Med 30(3): 421-442.
-
Lewis TJ, Trempe CL (2017) The End of Alzheimer’s. In: 2nd (Edn.), Academic Press, pp: 52-77.
-
Johnston C, Liddle J (2007) ‘The Mental Capacity Act 2005: a new framework for healthcare decision making’. J Med Ethics 33(2): 94-97.