A Study on Knowledge, Attitude and Practice of Hand Hygiene among Healthcare Professionals at a Tertiary Care Hospital, India
Hand hygiene is recognized as a leading measure to prevent cross-transmission of microorganisms responsible of healthcare associated infection. The present study aimed to compare the knowledge, attitude and practice of hand hygiene of health professionals of Nootan Medical College and Research Centre, and Nootan General Hospital, Visnagar, Gujarat, India. Out of total of 191 responses from an online survey, 39 (31 males and 8 females) medical staff, 67 (18 males and 49 females) nursing staff and 85 (42 males and 43 females) medical students were recorded. Majority of participants were young (18-30 years). Overall 29.31% of participants had good knowledge and 65.4% of participants had moderate knowledge of hand hygiene. Majority (65.44%) of participants with good attitude towards hand hygiene with higher number of participants (62.94%) with good hand hygiene practices were observed. Feedback about WHO five moments of hand hygiene, techniques of hand wash/hand rub, factors affecting hand hygiene practice, choice of cleaning agents and approaches for improving hand hygiene practices were not significantly different between medical staff, nursing staff and medical students. Results will serve as a base line data for continuous evaluation to find gaps, to create intervention for the improvement of hand hygiene practice, to frame hand hygiene curriculum for students and to allocate budget for hand hygiene facilities for the management of the hospital which ultimately improve patient safety.
Bipin RS¹, Varsha JG²* and Tej JG³
¹Nootan Medical College and Research Center, India ²Department of Pharmacology, Indubhai Patel College of Pharmacy and Research Centre, India ³Mohawk College, Canada
Introduction
Healthcare associated infection is a leading cause of morbidity and mortality globally. The burden of health-care- associated infection in developing countries is as high as 19%, poses a challenge to health care providers [1]. According to World Health Organization (WHO) report (2022), out of every 100 patients in acute-care hospitals, 7 patients in high- income countries and 15 patients in low- and middle-income countries will acquire at least one health care-associated infection during their hospital stay. On average, 1 in every 10 affected patients will die from their health care-associated infection [2]. Health care associated infections include central line-associated bloodstream infections, catheter-associated urinary tract infections, surgical site infections, hospital- acquired pneumonia, ventilator-associated pneumonia, and Clostridium difficile infections [3]. Multi-drug resistant and pathogenic microorganisms in a health care environment can often spread directly through contaminated hands of healthcare workers or the surrounding contaminated environment. Health care workers are reluctant to take preventable steps with simple hand washing to control these infections. Prolonged hospital stays, long-term disability, increased antibiotic resistance, huge additional costs for health systems, and unnecessary deaths are adverse outcomes of health care-associated infections [4].
The WHO guidelines on core components of infection prevention and control programs at the national and acute health care facility level cover best hand hygiene practices at the bedside as a part of standard precautions [5]. Further, WHO activities like “My five moments for hand hygiene” concept, the SAVE LIVES: Clean Your Hands global campaign and World Hand Hygiene Day (5th May) celebration helps for global promotion, visibility and sustainability of hand hygiene in health care and to ‘bring people together’ in support of hand hygiene improvement around the world [6, 7, 8]. Recently, WHO released its first-ever research agenda on hand hygiene in health care focusing on 6 core hand hygiene domains of research including system change, training and education, evaluation and feedback, reminders and communication, institutional safety climate, and impact of hand hygiene improvement on healthcare associated infection and antimicrobial resistance [9]. World Hand Hygiene Day 2024 is celebrated on the theme of promoting knowledge and capacity building of health and care workers through innovative and impactful training and education, on infection prevention and control, including hand hygiene [10].
Despite evidence report of WHO that good hand hygiene can prevent majority of infections and guidelines for procedural hand washing, yet practices at the point of care remain sub optimal worldwide. Average hand hygiene compliance without specific improvement interventions remains at around 40% but can be as low as 2% in low-income countries and 20% in high-income countries [11, 12]. After COVID-19, hand hygiene technique is becoming very familiar and improving its compliance is observed in the community worldwide still lack of hand hygiene facilities, knowledge, practices and culture have adverse outcome on patients and health care worker safety. For the last few decades, hospitals have taken the healthcare associated infections seriously and established infection tracking and surveillance systems in place, along with robust prevention strategies to reduce the rate of hospital-acquired infections. The most important barriers to practice hand hygiene in the hospitals are lack of knowledge of healthcare workers and their attitude. It is also lack of practice due to unavailability of hand hygiene facilities and instruments, lack of proper training and heavy workload. As a part of continuous quality improvement program, this project was designed with the aim to study knowledge, attitude and practice of health hygiene among health professionals of the hospital staffs of a tertiary care hospital and its affiliated medical college students.
Methodology
Cross-sectional (online survey) study was carried out including subjects of both gender and any age, who have been either working as healthcare professionals or students at Nootan Medical College and Research Centre and Nootan General Hospital, Visnagar, Gujarat, India. A structured validated self-administered Google Form questionnaire was created after extensive review of the literature and later distributed through the social media platforms for the data collection.
The form comprised V sections: section I with 6 questions for socio-demographics information; section II with 25 questions for knowledge of hand hygiene; section III with 8 questions concerning attitude of participants regarding hand hygiene; section IV with 6 questions regarding practice approaches of hand hygiene and section V with 21 questions of WHO’s hand hygiene information (five movements of hand wash, hand washing and hand rubbing techniques), feedback and recommendations for future research. Participants had to give their opinion ranging from strongly disagrees to strongly agree. Incomplete Google form data were excluded from the study.
A score of 0 was given for negative knowledge answers, attitudes and puny practices. 1 point was given for each correct response to positive knowledge answers, attitudes and good practices so that maximum score for knowledge is 25, attitude is 8 and for practice it is 6. A score of more than 75% was considered good, 50–74% moderate, and less than 50% was taken as poor. Responses of participants were recorded in Microsoft Excel spread sheet and were analyzed using Microsoft Excel 2010. Descriptive statistics was calculated using frequencies and percentages. Chi-square test was used to find out association between variables at a significance level of p< 0.05.
Results
Demographic data respondents such as gender wise and age group wise distribution are shown in Table 1. In the present study, a total of 191 responses were recorded. 39 medical staff, 67 nursing staff and 85 medical students were participated in the study and majority of them were young (belong to 18 - 30 years age group).
| Medical staff (n=39) | % | Nursing staff (n=67) | Nursing staff % | Medical students (n=85) | % | Overall (n=191) | % | p value | |
|---|---|---|---|---|---|---|---|---|---|
| Gender | |||||||||
| Male | 31 | 79.48 | 18 | 26.87 | 42 | 49.41 | 91 | 47.64 | <0.05 |
| Female | 8 | 20.51 | 49 | 73.13 | 43 | 50.58 | 100 | 52.36 | <0.05 |
| Age group (Years) | |||||||||
| 18-30 | 22 | 56.41 | 59 | 88.06 | 84 | 98.82 | 165 | 86.39 | <0.05 |
| 31-40 | 12 | 30.76 | 7 | 10.45 | 0 | 0 | 19 | 9.95 | |
| 41-50 | 2 | 5.13 | 0 | 0 | 1 | 1.18 | 3 | 1.57 | |
| 51-60 | 2 | 5.13 | 1 | 1.49 | 0 | 0 | 3 | 1.57 | |
| 61-70 | 1 | 2.56 | 0 | 0 | 0 | 0 | 1 | 0.52 |
Table1: Comparison of demographics of healthcare professionals.
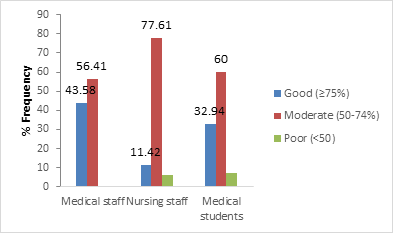
Frequency distribution of medical staff, nursing staff and medical students answered 25 knowledge questions in right manner is shown in Table 2. Highest positive responses of medical staff were observed followed by nursing staff and medical students regarding knowledge about routes of transmission of infection. Positive responses of students were more than nursing and medical staff regarding most frequent source of germs responsible for health care- associated infections. Differences between the medical staff, nursing staff and students while comparing correct responses of the most appropriate timing for performing hand hygiene actions that prevent transmission of germs to the patients and healthcare workers are shown in Table 2, however overall responses are more than 80%. Majority of the participants felt that hand rubbing is more rapid for hand cleansing than hand washing. Few participants were disagreed for hand rubbing cause skin dryness more than hand washing. 56.41% of doctors, 28.36% of nurses and 51.77% of students were not consented that hand rubbing is more effective against germs than hand washing. No significant difference of opinion of healthcare professionals regarding disagreement of recommendation of sequential performance of hand washing and hand rubbing. 71.73% and 52.88% participants with no difference among groups preferred rubbing for hand hygiene before palpation of the abdomen of patient and before giving injection respectively. Major proportion of respondents adopted rubbing/washing after removing examination gloves. Greater part of healthcare professionals was followed washing method after emptying a bedpan (58.11%) and visible exposure to blood (64.92%) while 42.41% of them were used rubbing method of hand hygiene after making patient bed. 83.25% of healthcare providers were removing hand accessories before the hand hygiene practices. Larger part of caregivers avoided damaged skin, artificial nails and preferred regular use of hand cream. Major percentage of participants (65.44%) in all groups had moderate knowledge level (Figure 1). Average knowledge score is higher in doctors followed by medical students and nursing staff.
| Sr. No. | Question | Medical staff (n=39) | Nursing staff (n=67) | Medical students (n=85) | Overall (n=191) | p value |
|---|---|---|---|---|---|---|
| 1 | Which of the following is the main route of cross-transmission of potentially harmful germs between patients in a health-care facility? | |||||
| Health-care workers’ hands when not clean | 22 | 29 | 30 | 81 | NS | |
| 56.41% | 43.28% | 35.29% | 42.41% | |||
| 2 | What is the most frequent source of germs responsible for health care-associated infections? | |||||
| Germs already present on or within the patient | 7 | 16 | 29 | 52 | NS | |
| 17.91% | 23.88% | 34.12% | 27.23% | |||
| 3 | The most appropriate timing for performing hand hygiene actions that prevent transmission of germs to the patient? | |||||
| Before touching a patient (Yes) | 38 | 63 | 80 | 181 | NS | |
| 97.44% | 94.03% | 94.11% | 94.76% | |||
| Immediately after a risk of body fluid exposure (Yes) | 33 | 53 | 78 | 164 | NS | |
| 84.62% | 79.10% | 91.76% | 85.86% | |||
| After exposure to the immediate surroundings of a patient (Yes) | 32 | 52 | 68 | 152 | NS | |
| 82.05% | 77.61% | 80% | 79.58% | |||
| Immediately before a clean/aseptic procedure (Yes) | 37 | 57 | 73 | 167 | NS | |
| 94.87% | 85.08% | 85.88% | 87.44% | |||
| 4 | The most appropriate timing for performing hand hygiene actions that prevent transmission of germs to the health care worker? | |||||
| After touching a patient (Yes) | 37 | 63 | 80 | 180 | NS | |
| 94.87% | 94.03% | 94.11% | 94.24% | |||
| Immediately after a risk of body fluid exposure (Yes) | 36 | 52 | 84 | 172 | <0.05 | |
| 92.31% | 77.61% | 98.82% | 90.05% | |||
| Immediately before a clean/aseptic procedure (Yes) | 35 | 58 | 70 | 163 | NS | |
| 89.74% | 86.57% | 82.35% | 85.34% | |||
| After exposure to the immediate surroundings of a patient (Yes) | 34 | 51 | 78 | 163 | <0.05 | |
| 87.18% | 76.12% | 91.76% | 85.34% | |||
| 5 | With respect to Hand cleansing which of the following statements on alcohol-based hand rub and hand washing with soap and water are true? | |||||
| Hand rubbing is more rapid for hand cleansing than hand washing (True) | 32 | 60 | 67 | 159 | NS | |
| 82.05% | 89.55% | 78.82% | 83.25% | |||
| Hand rubbing causes skin dryness more than hand washing (False) | 8 | 21 | 26 | 55 | NS | |
| 20.51% | 31.34% | 30.59% | 28.79% | |||
| Hand rubbing is more effective against germs than hand washing (False) | 22 | 19 | 44 | 85 | <0.05 | |
| 56.41% | 28.36% | 51.77% | 44.50% | |||
| Hand washing and hand rubbing are recommended to be performed in sequence (False) | 13 | 14 | 21 | 48 | NS | |
| 33.33% | 20.89% | 24.71% | 25.13% | |||
| 6 | Which type of hand hygiene method is required in the following situations? | |||||
| Before palpation of the abdomen (rubbing) | 28 | 52 | 57 | 137 | NS | |
| 71.79% | 77.61% | 67.06 | 71.73% | |||
| Before giving an injection (rubbing) | 24 | 38 | 39 | 101 | NS | |
| 61.53% | 56.71% | 45.88% | 52.88% | |||
| After emptying a bedpan (washing) | 27 | 29 | 55 | 111 | <0.05 | |
| 69.23% | 43.28% | 64.71% | 58.11% | |||
| After removing examination gloves (rubbing/washing) | 39 | 63 | 84 | 186 | NS | |
| 100% | 92.65% | 98.82% | 97.38% | |||
| After making a patient’s bed (rubbing) | 21 | 37 | 23 | 81 | <0.05 | |
| 53.84% | 55.22% | 27.06% | 42.41% | |||
| After visible exposure to blood (washing) | 24 | 35 | 65 | 124 | <0.05 | |
| 61.53% | 52.24% | 76.47% | 64.92% | |||
| 7 | Which of the following should be avoided, as associated with increased likelihood of colonisation of hands with harmful germs? | |||||
| Wearing Jewelry (Yes) | 34 | 62 | 63 | 159 | <0.05 | |
| 87.18% | 92.54% | 74.11% | 83.25% | |||
| Damaged Skin (Yes) | 38 | 52 | 77 | 167 | <0.05 | |
| 97.44% | 77.61% | 90.59 | 87.43% | |||
| Artificial Finger Nails (Yes) | 35 | 57 | 72 | 164 | NS | |
| 89.74% | 85.07% | 84.71% | 85.86% | |||
| Regular use of a hand cream (No) | 22 | 52 | 45 | 119 | <0.05 | |
| 56.41% | 77.61% | 52.94% | 62.30% | |||
| 9 | What is the minimal time needed for alcohol-based hand rub to kill most germs on your hands? (20 sec) | 28 | 34 | 33 | 95 | <0.05 |
| 71.79% | 50.75% | 38.82% | 49.74% | |||
| Average frequency of knowledge score | 28.24 | 44.76 | 57.64 | 130.64 | NS | |
| 72.41% | 66.81% | 67.81% | 68.39% |
Table 2: Comparison of knowledge levels of hand hygiene among healthcare professionals.
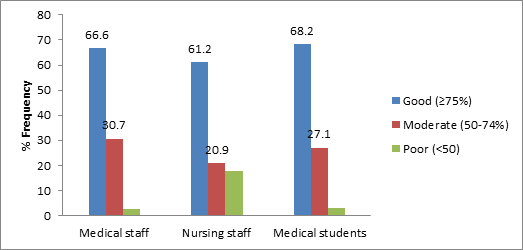
Data analysis of medical staff, nursing staff and medical students having positive attitude of hand hygiene practice are shown in Table 3. No significant difference was observed in medical staff (87.18%), nursing staff (76.12%) and medical students (85.88%) regarding their attitude of following correct hand hygiene all the time. Similar number of participants in all the groups had positive opinion that health care personnel should have sufficient knowledge and training about hand hygiene. Doctors were most serious about hand hygiene practice among all the groups; feel guilty if omit hand hygiene practice. 68.66% of nursing staff, 46.15% of medical staff and 58.82% of medical students were feeling hand washing cumbersome in emergency conditions. 74.36% of doctors, 76.12% of nursing staff and 77.65% of medical students were feeling uncomfortable when other omits hand hygiene practice. Highest frequency of nursing staff (77.61%) followed by medical students (56.47%) and medical staff (46.15%) were feeling reluctant to ask others to engage in hand hygiene. All groups had similar opinion that health care personnel should act as a role model for others and they should enrol in regular training sessions of hand hygiene practice. Out of total 191 participants 65.44%, 25.65% and 7.85% of participants have good, moderate and poor attitude respectively (Figure 2). Average attitude score is higher in medical students followed by nursing staff and doctors.
| Sr. No. | Question | Medical staff (n=39) | Nursing staff (n=67) | Medical students (n=85) | Overall (191) | P value |
|---|---|---|---|---|---|---|
| 1 | Correct hand hygiene practices should be followed at all times | 34 | 51 | 73 | 158 | NS |
| 87.18% | 76.12% | 85.88% | 82.72% | |||
| 2 | Health care personnel should have sufficient knowledge and training about hand hygiene. | 33 | 51 | 78 | 162 | <0.05 |
| 84.62% | 76.12% | 91.77% | 84.81% | |||
| 3 | I feel guilty if I omit hand hygiene. | 33 | 53 | 67 | 153 | NS |
| 84.62% | 79.11% | 78.82% | 80.11 | |||
| 4 | Hand washing is cumbersome in case of emergencies. | 18 | 46 | 50 | 114 | NS |
| 46.15% | 68.66% | 58.82% | 59.68% | |||
| 5 | I feel uncomfortable when others omit hand hygiene. | 29 | 51 | 66 | 146 | NS |
| 74.36% | 76.12% | 77.65% | 76.44% | |||
| 6 | I am reluctant to ask others to engage in hand hygiene. | 18 | 52 | 48 | 118 | <0.05 |
| 46.15% | 77.61% | 56.47% | 61.78% | |||
| 7 | A health care personnel should act as a role model for others. | 35 | 57 | 78 | 170 | NS |
| 89.74% | 85.07% | 91.76% | 89.00% | |||
| 8 | A health care personnel should enroll in regular training sessions regarding hand hygiene practices. | 35 | 54 | 77 | 166 | NS |
| 89.74% | 80.60% | 90.59% | 86.91% | |||
| Average frequency of attitude score | 29.37 | 51.88 | 67.13 | 148.38 | NS | |
| 75.32% | 77.43 | 78.97 | 77.68 |
Table 3: Comparison of attitude of hand hygiene among healthcare professionals.
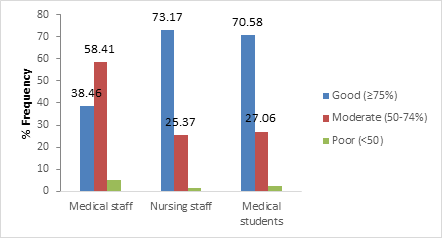
Data of practice level score is shown in Table 4. Almost all participants believed that hand hygiene is essential part of their role. Majority of student (95.29%) viewed that Infection prevention team has positive influence on their hand hygiene. Infection prevention notice boards reminder for hand hygiene poll was similar in all the groups. However, doctors had less influence of it. Nurses (77.61%) were experiencing more difficulties than medical staff (38.46%) and students (68.24%) to carry out hand hygiene due to more frequency required. Less number of medical staff (48.71%) missed out hand hygiene than nursing staff (77.61%) and medical students (51.76%) to their forgetfulness. Highest number of nursing staff (77.61%) was experienced difficulty to attend hand hygiene courses due to time pressure. While no significant difference was observed among doctors (48.72%) and students (51.76). Good ((≥75%) practice score was observed in majority of participants in all groups, Average practice score was higher in nursing staff than medical staff and medical students (Figure 3).
| Sr. No. | Question | Medical staff (n=39) | Nursing staff (n=67) | Medical students (n=85) | Overall (n=191) | P value |
|---|---|---|---|---|---|---|
| 1 | Hand hygiene is an essential part of my role. (Yes) | 39 | 67 | 83 | 189 | NS |
| 100% | 100% | 97.65% | 98.95% | |||
| 2 | Infection prevention team has a positive influence on my hand hygiene. | 34 | 58 | 81 | 173 | NS |
| 87.18% | 86.56% | 95.29% | 90.57% | |||
| 3 | Infection prevention notice boards remind me to do hand hygiene. | 32 | 61 | 78 | 171 | NS |
| 82.05% | 91.05% | 91.76% | 89.53% | |||
| 4 | The frequency of hand hygiene required makes it difficult for me to carry it out as often as necessary. | 15 | 52 | 58 | 125 | <0.05 |
| 38.46% | 77.61% | 68.24% | 65.45% | |||
| 5 | Sometimes I miss out hand hygiene simply because I forget it. | 19 | 46 | 48 | 113 | NS |
| 48.71% | 68.66% | 56.47% | 59.16% | |||
| 6 | It is difficult for me to attend hand hygiene courses due to time pressure. | 19 | 52 | 44 | 115 | <0.05 |
| 48.72% | 77.61% | 51.76% | 60.21% | |||
| Average practice score | 26.33 | 56 | 65.33 | 147.67 | NS | |
| 67.52% | 83.58% | 78.86% | 77.31% |
Table 4: Comparison of practice of hand hygiene among healthcare professionals.
Responses of hand hygiene information awareness and feedback of types of cleaning agents, reasons for poor compliance and approaches for improving hand hygiene compliance among healthcare professionals are recorded in Table 5. Education is given to the participants regarding 5 moments of hand hygiene, steps of hand washing and hand rubbing recognized by WHO. After that most of healthcare professionals (94.87% doctors, 97.02% nurses, and 91.76% medical students) gave positive feedback about awareness of 5 moments of hand hygiene and hand washing/hand rubbing methods described by WHO.
| Sr. No. | Question | Medical staff (n=39) | Nursing staff (n=67) | Medical students (n=85) | Overall (n=191) | P value |
|---|---|---|---|---|---|---|
| 1 | Hand hygiene is an essential part of my role. (Yes) | 39 | 67 | 83 | 189 | NS |
| 100% | 100% | 97.65% | 98.95% | |||
| 2 | Infection prevention team has a positive influence on my hand hygiene. | 34 | 58 | 81 | 173 | NS |
| 87.18% | 86.56% | 95.29% | 90.57% | |||
| 3 | Infection prevention notice boards remind me to do hand hygiene. | 32 | 61 | 78 | 171 | NS |
| 82.05% | 91.05% | 91.76% | 89.53% | |||
| 4 | The frequency of hand hygiene required makes it difficult for me to carry it out as often as necessary. | 15 | 52 | 58 | 125 | <0.05 |
| 38.46% | 77.61% | 68.24% | 65.45% | |||
| 5 | Sometimes I miss out hand hygiene simply because I forget it. | 19 | 46 | 48 | 113 | NS |
| 48.71% | 68.66% | 56.47% | 59.16% | |||
| 6 | It is difficult for me to attend hand hygiene courses due to time pressure. | 19 | 52 | 44 | 115 | <0.05 |
| 48.72% | 77.61% | 51.76% | 60.21% | |||
| Average practice score | 26.33 | 56 | 65.33 | 147.67 | NS | |
| 67.52% | 83.58% | 78.86% | 77.31% |
Table 5: Comparison of responses hand hygiene information feedback among healthcare professionals.
Feedback of healthcare providers regarding types of cleaning agents used concluded that alcohol based hand rub (94.87% doctors, 88.06% nurses, 95.29% students) was widely used followed by antiseptic (84.61% doctors, 88.06% nurses, 94.12% students), liquid soap (89.74% doctors, 79.11% nurses, 80% students) and soap bar (38.46% doctors, 68.66% nurses, 54.12% students). 87.18% of doctors, 83.58% of nurses and 71.76% of students felt convenient location of hand washing facilities.
Majority of caregivers affirmed that WHO recommended hand washing instructions was displayed in their working areas. 91.67% of healthcare professionals (87.18% doctors, 94.03% nurses, and 91.76% students) believed that lack of knowledge of guidelines/ protocols was a major reason for poor hand washing compliance. 79.49% of doctors, 82.09% of nurses and 76.47% of students identify lack of role model among staff may lead to poor compliance of hand hygiene practice.
Lack of manpower as per overburden patient flow and hand hygiene facilities were also viewed as noncompliance factors by medical staff, nursing staff and students. Some participants acknowledged noncompliance due to wearing gloves/ gowns or irritating nature of hand hygiene agents. Almost all the groups viewed in a similar way regarding hand hygiene approaches to improve hand hygiene compliance.
Discussion
Hospital acquired infection is a troublesome problem in any healthcare organisation around the world which ultimately lead to negative impact on the patient treatment provokinghealth complications and prolong hospital stay period. This burden is several folds higher in low- and middle-income countries than in high-income ones. Semmelweis demonstrated more than a century ago that hand washing itself was sufficient in reducing the incidence of infections. The COVID-19 pandemic and other recent large disease outbreaks have highlighted the importance of infection prevention and control in healthcare settings and in the community. WHO guideline for COVID-19 preventive measures also included effective hand washing technique with soap and water or alcohol based sanitizer as a major step for prevention of infection [13, 14, 15].
As per research agenda of WHO (2023), present study was focused on evaluation of knowledge, attitude and practice of hand hygiene and feedback about hand hygiene education. In the present study, 65.44% of total doctors, nurses and students have moderate knowledge and only 29.31% of them have good knowledge. Similar results were also observed in other research studies [16, 17, 18, 19]. The results showed deficits in the knowledge of the participants most notably in the areaof health-care workers’ hands when not clean are main route of transmission to patients and germs already present on or within the patient are source of infection of healthcare associated infections. More than 80% of the participants had update about most appropriate timing for performing hand hygiene actions that prevent transmission of germs to the patient and health care workers. Majority of the participants were aware about risk of colonization of harmful microorganisms in hand by wearing jewelry, damaged skin and artificial finger nails. Lack of awareness and scientific knowledge regarding hand hygiene is considered serious issue that impart improper infection control during training programs, resulting in bad hand hygiene practice among peers and students. It is important to address the gaps of knowledge with proper understanding and education/training.
Positive attitude score toward hand washing were good among the majority (65.44%) of the study participants. Students had more positive attitude compared to doctors and nursing staff might be due to their continuous learning about hand hygiene in their course curriculum and practical training. Overall64.92% of participants had good and 32.46% had moderate practice score with highest in the nursing staff. Several studies also recorded similar results [16, 17, 18, 19].
Thus, standard performance of hand hygiene in this hospital reflected the commitment of the top management and the health care workers towards the patient safety. Staff accountability and behavioural change are required to achieve 100% hand hygiene compliance. A multidisciplinary approach at hospital administration, healthcare professionals, nursing level, medical interns and students’ level is require to enhance hand hygiene compliance within the hospital. Targeted, multi-faceted approaches focusing on system change, administrative support, motivation, availability of alcohol-based hand rubs, training and intensive education of healthcare workers and reminders in the workplace have been recommended for improvement in hand hygiene.
Conclusion
Hand hygiene served as one of the primary modes of reducing healthcare associated infection and antibiotic resistance. Hand hygiene is an important quality indicator for patient safety recommended by WHO and National Accreditation Board of Hospitals and Healthcare Providers. To prevent healthcare associated infections as a part of infection control and prevention program, patient safety is continuously evaluated by Nootan General Hospital and Nootan medical College. Findings of the present study indicated high level of knowledge, attitude and practice of hand hygiene by the healthcare providers and medical students indicated standard quality of care of patient in this teaching hospital that serve as a base line data for continuous evaluation to find gaps and creation of intervention for the improvement of hand hygiene practice. Further, these results will serve as a guide to frame hand hygiene curriculum, education and training and innovative intervention development among students to improve hand hygiene. It will also serve as a torch bearer to the management for budget allocation to hand hygiene materials and facilities, training of newly recruited staff, display of advertisements of hand hygiene and need for monitoring of hand hygiene practice. This will ultimately reduce health care associated infections and economic burden to the society.
References
-
WHO (2010) the burden of health care-associated infection worldwide.
-
WHO (2022) WHO launches first ever global report on infection prevention and control.
-
Haque M, Sartelli M, McKimm J, Abu BM (2018) Health care-associated infections - an overview. Infect Drug Resist 11: 2321-2333.
-
Allegranzi B, Bagheri NS, Combescure C, Graafmans W, Attar H, et al. (2011) Burden of endemic health-care- associated infection in developing countries: systematic review and meta-analysis. Lancet 377(9761): 228-241.
-
WHO (2016) Guidelines on core components of infection prevention and control programmes at the national and acute health care facility level.
-
Allegranzi B, Kilpatrick C, Sax H, Pittet D (2022) ‘My Five Moments’: understanding a user-centred approach to hand hygiene improvement within a broader implementation strategy. BMJ Qual Saf 31(4): 259-262.
-
Salmon S, Pittet D, Sax H, McLaws ML (2015) the ‘My five moments for hand hygiene’ concept for the overcrowded setting in resource-limited healthcare systems. J Hosp Infect 91(2): 95-99.
-
World Hand Hygiene Day (2021) Seconds save lives – clean your hands.
-
WHO (2023) First-ever WHO research agenda on hand hygiene in health care to improve quality and safety of care.
-
World Hand hygiene day (2024) Why is sharing knowledge about hand hygiene still so important? Because it helps stop the spread of harmful germs in health care.
-
WHO (2022) WHO launches first ever global report on infection prevention and control.
-
WHO (2023) WHO research for hand hygiene in health care 2023–2030.
-
Lane HJ, Blum N, Fee E (2010) Oliver Wendell Holmes (1809-1894) and Ignaz Philipp Semmelweis (1818- 1865): preventing the transmission of puerperal fever. Am J Public Health 100(6): 1008-1009.
-
WHO (2020) Hand Hygiene for All Global Initiative.
-
WHO (2023) Infection prevention and control guideline for coronavirus disease 2019 (COVID-19): Executive summary.
-
Nair SS, Hanumantappa R, Hiremath SG, Siraj MA, Raghunath P (2014) Knowledge, attitude, and practice of hand hygiene among medical and nursing students at a tertiary health care centre in Raichur, India. ISRN Prev Med, pp: 608927.
-
Maheshwari V, Kaore NC, Ramnani VK, Gupta SK, Borle A, et al. (2014) A study to assess knowledge and attitude regarding hand hygiene amongst residents and nursing staff in a tertiary health care setting of Bhopal city. J Clin Diagn Res. 8(8): DC04- DC07.
-
Shinde MB, Mohite VR (2014) A study to assess knowledge, attitude and practices of five moments of hand hygiene among nursing staff and students at a tertiary care hospital at Karad. Int J Sci and Res 3(2): 311-321.
-
Arthi E, Abarna V, Bagyalakshmi R, Anitharaj M, Vijayasree S (2016) Assessment of knowledge, attitude and practice of hand hygiene among nursing and medical students in a tertiary care hospital in Puducherry, India. IJCMR 3(4): 1203-1206.
- Acido Labile or Gastro Irritant Apis and Enteric Release in Galenic Practice: An Overview
- Influence of Inoculum Concentration on In Vivo Incubation Period of Emmia lacerata, Pathogenesis and Management of Wilt in Pepper (Capsicum annuum L.)
- Vanilla’s Chemistry
- Marine Anti-Cancer Compounds and Adverse Effects of Global Warming on Oceans: An Overview
- Serological Investigation of Chikungunya Virus Antibody among Malaria-Suspected Febrile Patients in Some Healthcare Facilities in Rivers State
- Pharmaceutical Applications of White Button Mushroom (Agaricus Bisporus)